
ABSTRACT
Introduction A rare disease is defined by the European Health Commission as a disorder affecting less than 5/10,000 of the population. There are at least 20 rare liver diseases (RLDs) seen frequently in the adult and paediatric liver clinic, signifying that the hepatology community can be influential in developing such patient databases for registering patients with rare hepatic conditions. The aim of this review was, first, to identify registries for RLDs in Europe, and, second, to design a universal blueprint for the development of a registry for RLD by using lessons learnt from the European registries that have already been established.
Methods We searched PubMed, Google Scholar and clinicaltrials.gov using the MESH terms ‘registries’, ‘database management systems’, ‘database’ and the non-MESH terms ‘database$’, ‘registry’, ‘repository’ and ‘repositories’. We only included studies in English from countries/consortia of the European Union (EU). Our literature search was performed in 2020.
Results We identified 37 registries for RLDs in Europe. Using information from the design of these registries we designed a blueprint for the development of a patient registry for an RLD consisting of a theoretical, technical and maintenance phase.
Discussion It is believed that rare diseases may affect as much as 6–8% of the EU population across its 28 member states. Here we have provided a toolkit for designing a registry for an RLD. Our article will complement the efforts of loco-regional, national and international groups seeking to establish robust systems for data collection and analysis for orphan liver diseases.
Introduction
A rare disease (RD) or an orphan disease is defined by the European Health Commission as a disorder that occurs in <5/10,000 individuals. A disease is defined as ultra-rare if less than 1/100,000 people is affected.1 It has been estimated that there are 5,000–8,000 RDs affecting 6–8% of the European Union (EU) population.2 Rare liver diseases (RLDs) are often encountered in the hepatology clinic (Table 1).
Some of the commonest rare liver diseases often encountered in the hepatology and metabolic clinic according to www.orpha.net
Unmet needs for RDs include diagnostic delays, lack of awareness and education, inequalities in the accessibility of care, fragmented delivery of care, poor availability of treatments and paucity in research initiatives.3 Various initiatives and policies have been conceived to influence the adoption and implementation of plans for RDs including those from the EU (the Europlan project and Eurordis),4,5 the UK and the Royal College of General Practictioners,6–9 the Asia-Pacific region,10–15 the USA16 and the World Health Organization (WHO).17
More recently, we have seen the development of the European Reference Networks (ERNs). These are virtual networks aimed at facilitating multidisciplinary discussions on patients with RDs within European borders, encouraging the concentration of knowledge resources and streamlining the delivery of highly specialist treatments to patients with RDs. The networks employ telemedicine technology to allow specialists from various disciplines to meet and discuss individual patient cases. The first ERNs were launched in 2017 and there are currently 24, including ERN RARE-LIVER, which focuses on hepatological conditions.5 Of note, these networks have played a pivotal role in the European COVID-19 response, providing support to patients with RDs and their clinicians, including advice on vaccination, disease prevention and medical management for those infected with COVID-19 and its variants.
One of the most important aspects in the field of RDs is the establishment of disease registries. The term ‘registry’ has been broadly used to cover both the act of recording healthcare data and the collection of records. In recent years, we have seen significant advances in the field of disease registration and patient registries. These tools have evolved beyond the simplified scope of being ‘monolithic’ silos for patient characteristics and demographics. Disease registries for RDs are now being used not only to understand the patient journey and the life cycle of the disease but also to shape the care of patients and provide insights into the available treatments. For example, some of the outcomes of the United Kingdom Primary Biliary Cholangitis (UK-PBC) registry include the development of financial models for healthcare costs for patients with PBC,18 assessment of the quality of life of patients19 and the exploration of new pharmacotherapy targets for this rare condition.20 Similarly, registries for α1-antitrypsin deficiency are looking to understand the natural history of the disease across its different phenotypes and to provide insights into the effectiveness of augmentation therapy as a treatment modality for this cohort of patients.21 The multiple benefits of registries for RDs are outlined in detail in next section.
A comprehensive guideline for creating a registry for RLDs does not currently exist. Stanimirovic et al22 propose a framework for the construction of a registry ecosystem; however, their work is focused on Slovenian registries only and was conceptualised as a hypothesis in a country which does not yet have a national RD registration programme. D'Agnolo et al23 used their experience from building a registry for polycystic liver disease to deliver a methods-based paper, describing a template which can be used to design a registry for RDs, but did not include key aspects such as safeguarding of information governance, ethics considerations, registry funding and registry sustainability. Recent published work by Boulanger et al24 (funded by the US Food and Drug Administration) outlines the importance of collaborative research, and highlights the significance of research registries for RDs in an integrated healthcare environment and provides a very useful analysis of important considerations for registry development, including the challenges associated with research in this area, establishing clear and achievable objectives, early assembly of research consortia, ethical considerations, and active participation of all stakeholders to align registries towards common objectives; however, their efforts were not directed towards providing a structure for designing registries for RLDs, and they provide a descriptive overview rather than a blueprint.
The aim of this review was to identify registries for RLDs in Europe and to design a universal blueprint for the development of a registry for an RLD by using lessons learnt from these established registries.
Benefits of creating rare disease registries
Epidemiology and public health
Clinical registries are often used to register patients with an RD. They are not usually capable of giving prevalence and incidence estimates of rare illnesses and are subject to specialist centre bias. They do not often include deceased patients (but this can be decided when considering the scope and information governance of the registry) and only include patients who have consented. However, they are excellent tools for elucidating the natural history of an RD and facilitating the study of rare exposures and outcomes. They have the ability to improve the clinical interface by capturing data on individual patient journeys. Population-based registries (national and international) on the other hand may hold less granular data on individual patients but are more appropriate in studying the epidemiological aspects of rare and ultra-rare diseases because they focus more on numbers of patients and the chronological data around diagnosis.
Clinical benefits
The data within registries can be used to perform multiple subgroup analyses for patients with rare diagnoses, eg patients with Wilson Disease with stage 3 liver fibrosis. The data can be used to risk-stratify patients, identify high-risk patients requiring screening and aid the development of decision support tools in order to promote proactive clinical management. Registries can also help to initiate, optimise and monitor pharmacotherapy.
Financial benefits
In the long term, registries can help improve health economics, even considering the initial set-up costs. Electronic data extraction is often possible, for example linking lab results directly to the registry. Moreover, they can identify gaps and inefficiencies in clinical care and improve the financial efficiency of health services. They can achieve cost savings by promoting correct prescribing and can help services achieve targets that may be financially incentivised. Data derived from patient registries can influence commissioning and therefore shape delivery of care.
Educational benefits
Disease registries can signpost educational resources, such as online evidence-based guidelines. Registries can also be integral to care bundles such as action sets for the management of gastrointestinal bleeding.25 They can even facilitate the creation of clinical guidelines, especially when the registry is multinational and captures clinical practice from multiple countries.
Governance benefits
Health registries can improve data quality and facilitate audit and reporting of outcomes which can further improve local services, increase the quality of care delivered to patients and help to identify gaps in clinical pathways.
Research and audit benefits
Conducting clinical trials for rare liver diseases is challenging due to the small numbers of patients. Registries can provide relatively large amounts of data to study orphan diseases, especially when data is inputted from multiple recruiting sites. Candidate patients can be screened electronically for eligibility for inclusion into clinical trials. Furthermore, some registries, such as population-based registries, may promote and facilitate clinical audit. For example, the UK National Lung Cancer Audit is carried out with support from the population-based National Cancer Registry.
Literature review methodology
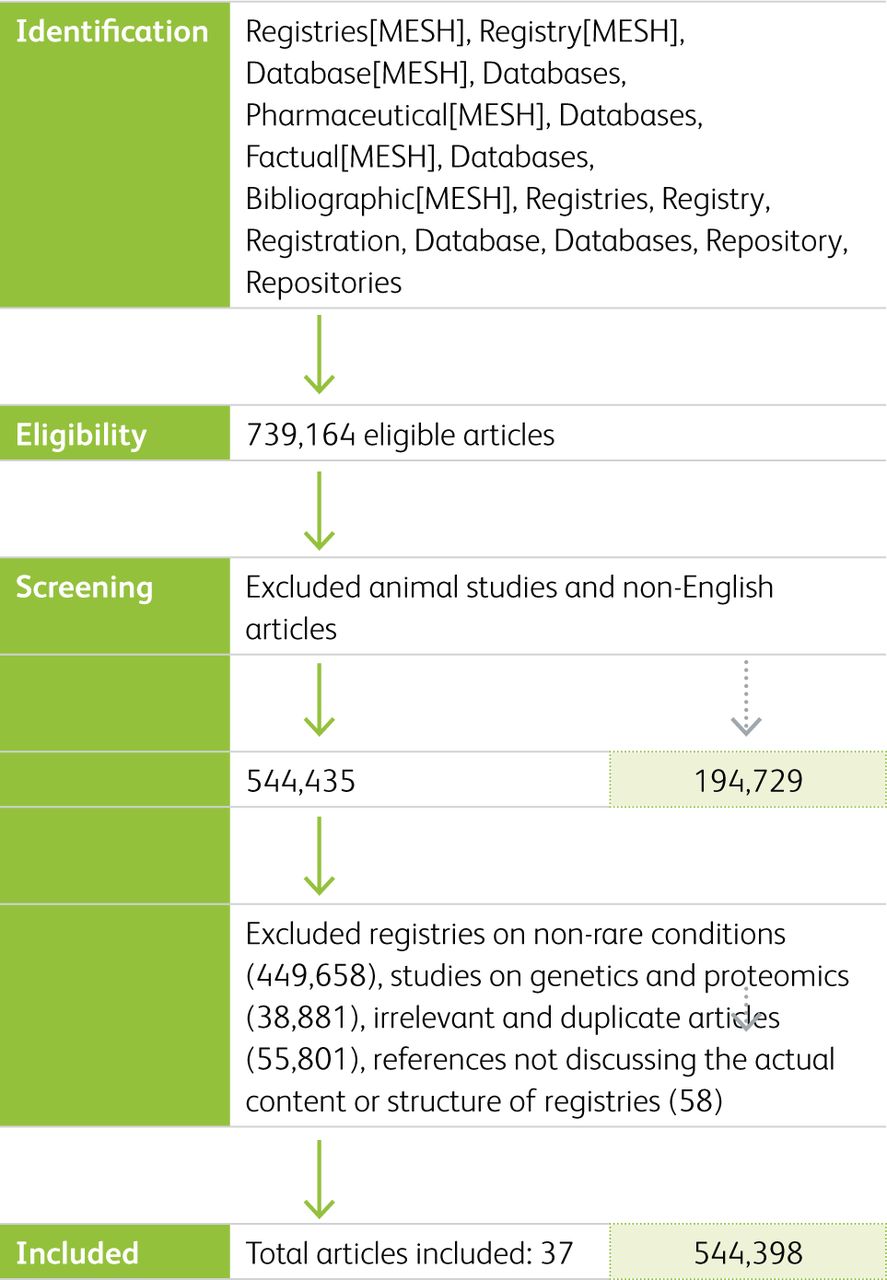
We carried out a search to identify registries for liver conditions within the EU. Medical subject headings (MESH) and non-MESH criteria were used to search international academic databases (MEDLINE®/PubMed® and Cochrane), grey literature, clinicaltrials.gov and Google Scholar. The MESH terms used included ‘registries’, ‘database management systems’, ‘database’. The non-MESH terms used were ‘database$’, ‘registry’, ‘repository’ and ‘repositories’. We limited our search to articles published in English and on humans only. Our literature search was performed in 2020. A total of 37 articles were included (Fig 1). We acknowledge that there are several registries for RLDs; however, here we only included those which are non-interventional and with published outcomes within the EU. The final papers to be included were validated by an external collaborator.
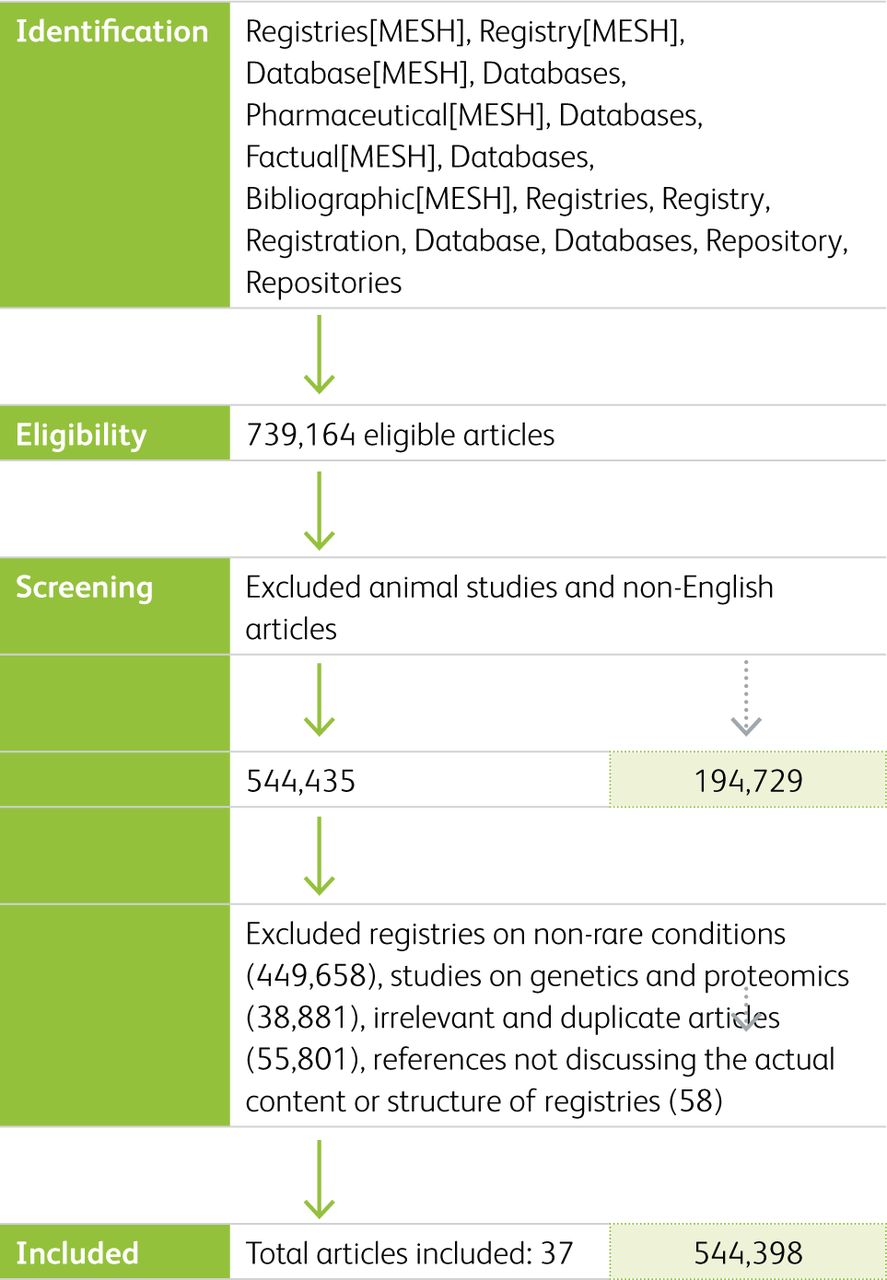
PRISMA flow chart of included studies.
Through a careful analysis of each article and accompanying registry protocols (where available), we identified threads which constitute towards the construction of a framework for registry design. The decision on which threads were chosen for inclusion was based on the frequency they appeared in the included articles and the relevance to the aims of this paper. This has led to the development of a blueprint, which the authors propose should be used as the gold standard for the design of registries for RLDs.
From our search, we identified multiple registries with published outcomes, as summarised in Table 2. Two of the identified registries involved hepatobiliary cancers, eight were focused on autoimmune liver diseases and four included patients with metabolic liver disease. The remaining registries included outcomes from patients with congenital and vascular liver disorders. Most of these registries included both patient and investigator-derived data.
Examples of registries for rare liver diseases
The following aspects of registry design were recurrent threads in the identified articles. Below, we extrapolate on their merits, as discussed in the included articles.
A blueprint for registry design
The following aspects of registry design were recurrent threads in the articles identified in our literature search. Below, we extrapolate on each of these aspects, as discussed in the included articles.
Establishing aims and objectives
A well-designed registry should be able to translate a clinical/academic question into measurable exposures and outcomes. Setting aims and objectives should consider existing registries and hence avoid duplication. Many registries may have more than one purpose or rationale.26 For example, the main aim of the EuroWilson registry was to assess the feasibility of conducting randomised controlled trials for the treatment of Wilson's disease, while the UK-PBC registry aims to identify subsets of PBC patients such as those not responding to ursodeoxycholic acid (UDCA), elucidate the molecular mechanisms behind treatment non-response and strengthen relationships between clinicians, the NHS, patients and industry. Some registries for the same RLD may have different aims and objectives. For example, the European Liver Transplant Registry (ELTR) has been collecting prospective transplant data on patients with polycystic liver disease (PLD). However, this registry was not designed to collect retrospective long-term data to address research questions around the natural history of PLD, quality of life, disease prognostication or risk-stratification of patients. Drenth et al have set up an international registry of patients with PLD to serve exactly this gap.23,27
The main aims and objectives used in the identified articles are listed in Box 1.
Commonest aims and objectives for rare liver disease registries
Defining the target population and observation period
The definition of the target population will determine which patients are eligible for inclusion into the registry. Having very extensive and strict inclusion/exclusion criteria for registries can miss patients. It is generally preferrable to have broader criteria to accommodate protocol amendments in the future as the understanding of the studied disease improves.
Existing epidemiological data can guide decisions around planning, costing, IT infrastructure and workforce. Inclusion and exclusion criteria should be included in the registry protocol. For example, D'Agnolo et al used a cut-off of 20 liver cysts for inclusion into their polycystic liver disease registry study, whilst the United Kingdom Autoimmune Hepatitis (UK-AIH) registry study excludes all patients who have HIV.23
Establishing information, research and clinical governance
The design protocols for disease registries include sections describing both the lawful basis of data collection as well as the process of accessing and extracting registry data. Different countries have different bases for collecting data. For example, in England, the National Disease Registration Service collects RD patient data without consent under direction from the secretary of state under Section 254 of the Health and Social Care Act 2012. Governance regulations for each country should be identified early in the process of registry design in order to ensure compliance. Specific approaches to data, such as pseudonymisation/anonymisation of records, should be considered to protect patient identity. This is particularly important for RDs where many members of one family may have the same RD, symptoms or phenotype.
Securing sponsorship and funding
The sustainability and efficient running of a registry are reliant on sufficient funding and sponsorship. It is therefore important to pilot a smaller-scale feasibility registry initially. Registry funding can be sourced from various bodies including government organisations, non-profit disease foundations, patient groups, charitable foundations, private funds from philanthropists, industry and professional societies.28
The European Commission receives regular applications for funding support for RDs and its third Health Programme (covering the period from 2014–2020) supports the setting up of RD registries as part of its operating framework.29 Collaborative rather than individual efforts are encouraged. The European Association for the Study of the Liver (EASL) also provides registry funding for liver diseases through its EASL registry data collection grant scheme. To date, it has awarded grants for the development of several orphan hepatic disease registries.30 Other organisations which also accept applications for registry funding include the UK's medical research council (MRC) and the UK's National Institute for Health and Care Research (NIHR).
Recruiting the registry team
The workforce required for designing, running and maintaining the registry should be defined early. A multidisciplinary team approach is key to the successful implementation and ongoing success of any registry. It is therefore important to set realistic and achievable targets. It is desirable to appoint project managers with financial and leadership experience to facilitate conversations with funding bodies and sponsors. Registry operators with roles in data liaison should be considered to ensure the effective negotiation of data from data providers. Team members with legal and information-governance expertise as well as a strong grounding in epidemiology, medical statistics and population-based studies should be considered.
Identifying stakeholders and setting up wider collaborations
A registry may have one or more stakeholders: people or organisations who have an interest in the research question the registry is trying to address. Stakeholders can be either primary or secondary.28 A primary stakeholder is responsible for the logistics of setting up the registry while a secondary stakeholder is identified as the party who will benefit from the data and the answers to the clinical endpoints of the registry. Stakeholders will probably include clinicians, researchers, academic institutions, patients, the public, community leaders, policy makers, professional societies, regulatory agencies and industry partners.
The importance of collaborations in the field of RDs, where data is scarce and fragmented, has already been highlighted. Examples of successful large-scale registry collaborations on RLDs include the international Primary Sclerosing Cholangitis (PSC) registry, the α1 International registry (for α1 antitrypsin deficiency), the European Registry for Liver Disease in Pregnancy and the European Repository of Patients with IgG4-related Disease, all of which have been funded through the registry programme of the EASL.30
Setting up a data management system
Data management systems (DMSs) serving registries for RD must be dynamic, integrative, extendable, customisable and intuitive in order to serve the designed purpose and objectives. The best choice of DMS depends on the expertise available within the team and the available funding. Ideally, the DMS should be able to derive data automatically from electronic patient records as soon as a patient is registered into the database. However, while this may be a desirable functionality for local registries, it may not be feasible for regional, national and international registries for many reasons, including heterogeneous data coding, multitude of patient workflow products, differences in ethics committee (or Institutional Review Boards equivalent in North America) standards across regions/borders, differences in local security protocols and the lack of electronic patient records. Therefore, the most resource-efficient way of achieving a common and shared data exchange could be a web-based model that can provide various database access levels. For example, the European Network for the Study of Cholangiocarcinoma (ENS-CCA) have achieved this by using an established secure platform called REDcap (Research Electronic Data capture) to bring together data from 33 groups from 12 European countries, while other consortia such as UK-AIH use bespoke software solutions.
Data validation should be introduced at various checkpoints to ensure that variables follow the expected format and to prompt users to input missing data.
The use of a data dictionary to define and standardise each variable is encouraged. As part of the registry's maintenance processes, regular data cleaning should also be undertaken to address problems that might not be addressed by validation, such as logical inconsistencies. Data validation/integrity can be further improved through a multi-source approach to registration. This means that data should be collected from various independent sources when possible. An example is the UK's National Congenital Anomaly and Rare Disease Registration Service (NCARDRS), which collates, validates and registers data from various sources at local, regional and international level at various stages of the patients' journey. This approach enables NCARDRS to achieve the highest possible ascertainment and completeness of cases in the population.31
Disease registries for RD should be expandable and customisable to allow data linkage from different sources such as primary care, by providing options for integration with their databases.32 One of the biggest challenges for RD data is heterogeneous coding and isolated silos of data. Notably, many RDs do not have an International Classification of Disease 10 (ICD-10) code. Moreover, it is not unusual to find RD being misclassified in generalist registries. For example, from our own experience, primary biliary cholangitis is often coded as secondary biliary cholangitis, and different codes are used between primary and secondary care, ie Read vs. ICD-10.33 The EU has recommended that member states should ensure correct and traceable coding of RDs using ICD and that future versions of ICD should include refined codes for RDs. The use of other diagnostic coding systems, including the Orphanet Rare Disease Ontology or SNO-MED CT should be considered, particularly if granularity of diagnosis is important or if these are used in local routinely collected healthcare data systems.
As we move towards in the era of complete online data integration, it is particularly important to design registries for RLDs with full online capabilities and options for direct patient activation.34 Electronic surveys and questionnaires could feed directly into the DMS and patient-entered data could automatically update the data fields in the registry. One example is the PBC-40 questionnaire, which has been studied and validated in various settings and languages for PBC.35,36 Carbone et al37 also successfully collected self-reported data from patients with PBC utilising the PBC-40 questionnaire, the Epworth sleepiness scale, the orthostatic grading scale, the hospital anxiety and depression scale, and the pruritus visual analogue scale. Moreover, data from the DMS can help the development of decision support tools and provide reminders for clinical decision-making, eg biannual ultrasound and α-fetoprotein (AFP) screening for hepatocellular carcinoma (HCC) surveillance.
Ensuring registry sustainability
Plans for registry sustainability need to be developed early, with the close involvement of project managers, investigators, the steering committee and other relevant stakeholders. Sustainability plans will need to involve funders and sponsors, as the value of grants and support will dictate the size of the registry and the timescale for data acquisition. Procedures around patient registration, consent and participant retention (and loss to follow-up) will need to be outlined in the registry protocol. Exit strategies from the registry in the event of funding running out should be clearly discussed.
Gathering feedback
Feedback from participants and team members is very important. Engagement of the registry team with participants is encouraged to disseminate updates, information and newsletters and participants are given a platform to express their opinions and concerns about the running of the registry. Telephone helplines, online patient forums and feedback to appropriate patient charities can be used to engage those on the registry or those considering registering or opting out. All sources of patient communication should be reviewed regularly by the project team and steering committee to improve services and participant experience.
Authorship and contribution of published outcomes
A successful registry for RLDs will invariably yield outputs including newsletters, short abstracts and publications. The research protocol should provide explicit definitions for the roles of authors and contributors so that credit is appropriately awarded and responsibility for the published outcomes is acquired. The International Committee of Medical Journal Editors (ICMJE) has published widely accepted criteria for both authors and non-author contributors and we advocate for the use of these criteria in the protocols of disease registries for RLDs. Moreover, the registry protocol should provide clear explanation as to whether the work forms part of a wider consortium and whether the consortium will be cited alongside the named authors and contributors.38 We therefore recommend an organised approach to consensus building for authorship and, if possible, a separate publications committee that can advise on whether a subject merits full study-wide recognition or just writing group recognition, and reports back to the larger steering committee for discussion and ratification. We recognise that it might be challenging to introduce all the parameters that might arise from publication authorship into the registry protocol of a multiyear and multinational study, but it is always good practice to discuss this with all stakeholders upfront.
Discussion
Registries for RLDs can have an abundance of benefits, such as improving patient care and public health and facilitating medicine regulation, research, commissioning and patient empowerment to name a few. Registries are particularly important for RLDs because clinical trials may not be feasible due to low patient numbers and they are therefore the cornerstone for evaluating patient outcomes.
The aim of this review was to identify registries for RLDs in Europe and to design a universal blueprint for the development of a registry for an RLD by using lessons learnt from these established registries. Using a carefully described methodology to keep the work focused, we carried out a systematic literature review for European registries and included 37 papers. Using the data collected during this study, the authors were able to develop a novel blueprint for the design and delivery of registries for RLDs. The design process is divided in three phases: the theoretical, technical and maintenance phase. The framework can be delivered in 11 steps, and these are summarised in Box 2.
Essential components for creating a successful and sustainable registry for rare diseases
A strength of our paper is that it includes aspects not comprehensively covered by previous work, such as safeguarding of information governance, ethics considerations, sponsorship and funding, the technical aspects of the data management system and the importance ensuring sustainability and gathering feedback. Another strength of our paper is how it complements the efforts of the EASL ‘Registry Grants’ scheme and ERN Rare liver for the promotion of registration of patients with an RLD.
Our paper has some identified limitations. Our final list of included papers does not include registries without published outcomes. Moreover, our methodology also excluded registries outside the EU. This is not a reflection on the quality of non-EU registries but simply a deliberate focus on the EU registries, which have been conceived and developed within the European governance structure and in response to EU policy initiatives. The authors acknowledge that Brexit has undoubtedly had a detrimental impact on healthcare collaborations between the UK and the EU, potentially affecting the seamless sharing of data with the UK. Even though the UK/EU trade and cooperation agreement allows UK researchers to still participate in Horizon Europe programme, it does not mention the UK's participation in the 24 ERNs.39 This is particularly important as UK researchers, clinicians and patient advocates have been at the forefront of the development of the ERN concept and led six of these networks. Absence from these networks will no doubt deprive patients and clinicians of the opportunity to discuss their patients, have direct access to clinical trials and overall affect the care of patients with RLDs. At the time of writing this manuscript, 1,411 clinical centres were contributing to the 24 ERNs across 29 countries.40 Regrettably, none of these centres appeared to be in the UK. Even outside the ERNs, participation of the UK in European disease registries has become very challenging due to the disparities in information governance processes, constitutional disharmony, and enhanced ethics considerations. Future efforts should focus on how the UK can return to the ERNs and how the ERNs can collect important registry data from UK cohorts.
In conclusion, we believe that diseases registries should form the backbone for studying RLDs and should sit high in national agendas. While we acknowledge that a ‘one size fits all’ model may not be suitable when a registry is designed, we do believe that multidisciplinary registry developers, including academics, clinicians and industry, should consider our blueprint to navigate through the process and maximise the chances of making the registry relevant and fit for purpose.
Acknowledgments
We are very grateful to Mary Bythell, head of rare disease registration, National Disease Registration Service, NHS Digital, UK, for her critical review and advice on the manuscript.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/clinmedicine:
S1 – Expanded aims and objectives for rare liver disease registries.
- © Royal College of Physicians 2022. All rights reserved.
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.