
ABSTRACT
The patient in case 1 was a 50-year-old man who presented to the emergency department of the local hospital with chest pain and syncope for 3 hours due to acute myocardial infarction. He underwent cardiopulmonary resuscitation (CPR) followed by extracorporeal membrane oxygenation (ECMO), and intestinal perforation was detected on day 9. The patient in case 2 was a 58-year-old man who was admitted to the hospital with abdominal pain lasting for 3 days. He also required CPR and ECMO for cardiogenic shock, and intestinal perforation was identified on day 7 of ECMO. We believe that this case report will be important to alert clinicians to the possibility of this complication and to encourage early detection and intervention to improve prognosis. Conventionally, the gastrointestinal tract has received secondary attention in patients receiving ECMO support because the vital organs tend to be considered first. However, this case report illustrates the importance of monitoring gastrointestinal function in patients undergoing ECMO.
Introduction
Extracorporeal membrane oxygenation (ECMO) is a life support therapy for patients with cardiac or pulmonary failure, and its application is continually expanding.1 Notably, the application of ECMO increased during the COVID-19 pandemic, to stabilise patients with hypoxaemic or hypercapnic pulmonary failure. However, many complications can occur during ECMO and seriously affect the prognosis. Mesenteric artery embolism refers to a series of complications caused by thrombi or emboli leading to intestinal ischaemia; however, there are currently no reports of this complication during ECMO. In this study we share the details of two consecutive cases of this kind at our centre to alert other clinicians to the possibility of this rare complication.
Case 1
A 50-year-old man presented to the emergency department of the local hospital on 4 September 2021 with chest pain and syncope for 3 hours. Electrocardiography (ECG) suggested acute myocardial infarction (AMI) with elevated troponin I (TNI). Cardiogenic shock was apparent, and dobutamine was administered to increase his blood pressure. The patient was then transferred to Hangzhou First People's Hospital, which took approximately 2 hours. A veno-arterial (VA)-ECMO was then performed. After 67 minutes of cardiopulmonary resuscitation (CPR), circulatory support was established, and the patient was sent to the catheterisation laboratory for coronary angiography.
The patient had a history of fatty liver disease and hypertension for 5 years, but his highest blood pressure was unknown. He had smoked an average of 30 cigarettes/day for >30 years and consumed 250–500 mL white wine per day for the past 30 years. The patient also previously underwent appendectomy.
Emergency coronary angiography showed no significant left main coronary artery (LMCA) stenosis and complete occlusion of the proximal segment of the left anterior descending (LAD) artery. The proximal segment of the gyral branch was 99% narrowed, and the distal end formed a collateral circulation to supply the right crown. The right coronary artery (RCA) opening was completely occluded, and the distal end formed a bridge to the collateral circulation. The LAD artery was opened because of difficulty in opening the RCA. The patient was transferred to the intensive care unit (ICU) after intra-aortic balloon pumping (IABP). To maintain circulatory assistance with ECMO and treat AMI, postoperative systemic heparin anticoagulation, aspirin (100 mg four times a day (qd)) and ticagrelor (90 mg twice a day (bid)) were administered. Abdominal dilation was observed, and bladder pressure was 25 mmH2O. Approximately 500 mL of a coffee-like fluid was drained from the gastric tube, and proton pump inhibitor therapy was administered. Subsequently, intra-abdominal pressure fluctuated between 20 and 30 mmH2O. Continuous gastrointestinal decompression and intermittent enemas were administered, and the patient had poor bowel movement without defecation.
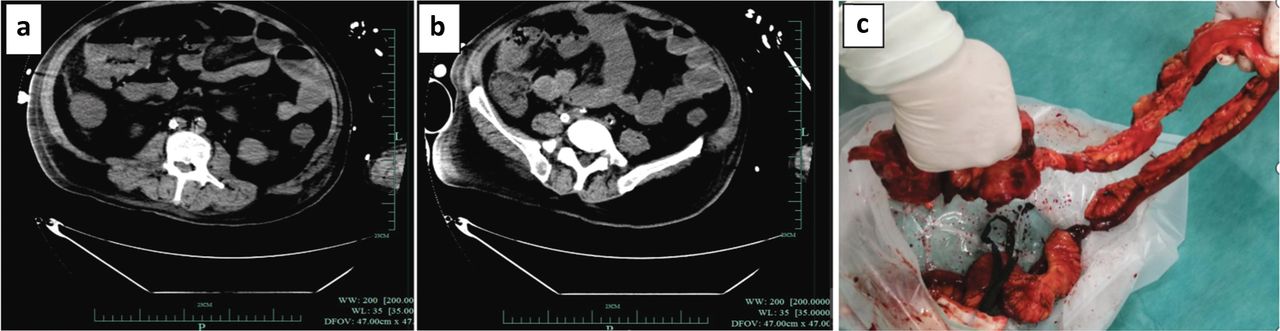
The patient was transferred to veno-arterial-venous (VAV)-ECMO on 10 September 2021 due to poor oxygenation. His circulation and oxygenation gradually improved, but he continued to demonstrate a high abdominal pressure and poor gastrointestinal motility. On the ninth day of ECMO (11 September 2021), abdominal computed tomography (CT; Fig 1a and 1b) suggested significant intestinal canal dilatation with multiple air–fluid levels, as well as multiple small gas shadows in the right upper and middle abdominal wall and part of the small intestinal wall in the middle and upper abdomen. A dense and blurred intestinal space and a small amount of fluid in the abdominopelvic cavity were observed. To reduce gastrointestinal pressure, gastroscopy was performed, which revealed an ulcer in the gastric sinus, and a small bowel decompression tube was placed. Abdominal pressure was still high, so surgical exploration was performed, which suggested ileal necrosis. The necrotic ileum was resected, and an ileostomy fistula was performed (Fig 1c). Poor postoperative cardiac recovery and difficulty with ECMO evacuation led this patient to be placed on the heart transplantation waiting list. He was subsequently referred to the transplant centre for a heart transplant evaluation. However, the patient declined further treatment; thus, he was discharged on day 16 of ECMO support.

Case 1. a and b) Preoperative abdominal computed tomography (CT). a) CT showing intestinal obstruction. b) CT showing an increased density in the intestinal wall. c) Postoperative intestinal perforation and necrosis.
Case 2
A 58-year-old man was admitted to Hangzhou First People's Hospital on 11 September 2021 with abdominal pain lasting for 3 days, which was aggravated by irritability for half a day. The patient vomited and experienced weakness and night sweats. He attended the hospital emergency department by ambulance. Upon presentation, sudden ventricular tachycardia and failure to palpate the aorta were noted. The sinus rate was restored after 7 minutes of defibrillation and CPR, and ECG showed ST-segment elevation in the anterior and high lateral leads with a TNI concentration of 1.4 ng/mL. Emergency coronary angiography showed sub-total occlusion of the LMCA opening and approximately 50% stenosis of the middle segment of the LAD artery, with no significant gyral branch or right crown stenosis. IABP was performed via the right femoral artery with 1:1 balloon counterpulsation, and drug stents were placed in the LAD and gyral branches to open the vessel. After surgery, the patient was in cardiogenic shock, so VA-ECMO was performed to assist his circulation. Systemic heparin anticoagulation, aspirin (100 mg qd) and ticagrelor (90 mg bid) were administered. On 13 September 2021, the patient's platelet count was 34 × 109/L. Aspirin was discontinued, and ticagrelor monotherapy (90 mg bid) was continued.
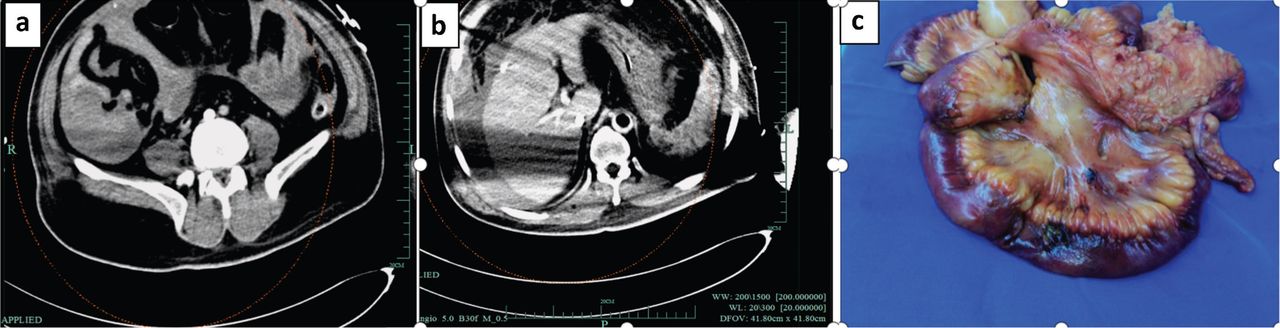
The patient's cardiac function gradually improved, his circulation was stable under maintenance with small doses of norepinephrine, and haemoglobin was maintained at around 8 g/dL. On 18 September 2021, his blood pressure dropped significantly and required maintenance with high-dose norepinephrine (0.8 μg/kg/minute). His heart rate reached 200 beats per minute. Arterial blood gas analysis showed that haemoglobin was 5.2 g/dL (significantly lower than before) and lactate was 9.2 mmol/L. Intra-abdominal pressure was elevated, and bedside ultrasonography revealed a dark area of fluid in the abdominal cavity. Diagnostic puncture was performed to remove the non-coagulated blood. Abdominal CT (Fig 2a and 2b) revealed fluid accumulation and haematoma formation in the posterior lateral wall of the ileocaecal region, and submucosal haemorrhage in the posterior lateral wall of the ileocaecal region was considered. A dissection was performed and it was found that the abdominal cavity was bleeding (around 4,000 mL), free faecal fluid was visible, part of the small intestine was covered with faecal moss, the caecum and part of the ileum were dark (similar to the purple colour of the mesentery) with no obvious peristalsis, and perforation of the intestinal wall (around 1 cm) was visible 30 cm from the end of the ileum. Around 1.5 m of the ileocaecal portion with part of the necrotic small intestine was removed (Fig 2c). The patient was successfully withdrawn from ECMO assistance on day 11 (21 September 2021); however, he developed short bowel syndrome after ECMO withdrawal.

Case 2. a and b) Preoperative abdominal computed tomography. a) CT showing ileocaecal effusion. b) CT showing perihepatic effusion. c) Postoperative intestinal perforation and necrosis.
Discussion
Many complications can occur during ECMO, which can affect prognosis. The underlying disease in both patients in this study was AMI. The patient in case 1 underwent extracorporeal CPR (E-CPR) followed by ECMO, and intestinal perforation was detected on day 9. The patient in case 2 underwent percutaneous coronary intervention (PCI) after 7 minutes of CPR and VA-ECMO for postoperative cardiogenic shock, and intestinal perforation was identified on day 7 of ECMO. There are no previous reports of intestinal ischaemic perforation in patients undergoing ECMO.
Both patients had terminal ileal perforation, which may not be a coincidence. Studies have shown that the coeliac artery, superior mesenteric artery (SMA) and inferior mesenteric artery constitute a collateral circulation with a high compensatory capacity.2 However, the SMA only has central collateral branches, resulting in a fragile peripheral circulation. Around 85% of patients with acute mesenteric artery infarction demonstrate SMA involvement, which plays a major role in the diagnosis of intestinal ischaemia. In contrast, the terminal ileum is supplied by the ileocolic artery, which is the SMA branch furthest from the SMA origin. An inadequate blood supply during cardiogenic shock may lead to mesenteric ischaemia, which develops into mesenteric embolism in 20% of patients.3 This condition results from reduced mesenteric perfusion due to a decrease in cardiac output. A case–control study in patients undergoing haemodialysis found that the incidence of mesenteric ischaemia was higher in hypotensive patients than in normotensive patients, and concluded that a systolic blood pressure of <100 mmHg may indicate mesenteric ischaemia. 4 Other studies observed a high incidence of mesenteric ischaemia in patients with chronic heart failure, sepsis, severe hypotension and hypovolaemia.5,6 Both patients in this case report had prolonged hypoperfusion, which may have contributed to mesenteric vessel ischaemia. If prior vascular sclerosis and chronic occlusion exist, intestinal ischaemia will be aggravated. Therefore, an adequate perfusion pressure should be achieved during cardiogenic shock.
In addition to the above-mentioned causes, acute mesenteric artery embolism may have been responsible. Although thromboembolism was possible, several cardiac ultrasound evaluations were performed, cardiac thrombosis was not detected, and heparin anticoagulation was continued during ECMO. The commonly mentioned risk factors for acute mesenteric infarction are cardiac arrhythmia, previous myocardial infarction, systemic atherosclerosis and hypertension. There is also a separate type of functional non-occlusive mesenteric ischaemia (NOMI) that is caused by ischaemia from vasospasm in the intestinal circulation. It can occur at sites of low blood flow, such as after cardiac surgery or during dialysis. NOMI can also be caused by sepsis and certain drugs, such as digitalis. The prognosis of NOMI is very poor (mortality of 50%–70%) due to vasospasm in extensive intestinal segments and to the difficulty of diagnosis.7 Both patients in this case report had a history of cardiac arrhythmia and high-risk factors for vascular sclerosis. Based on postoperative resection of the small intestine, we later considered that ischaemic perforation could have been caused by acute mesenteric embolism or spasm. Thus non-malignant arrhythmias, such as atrial fibrillation, may require more aggressive management during ECMO.
Early recognition of acute mesenteric ischaemic perforation is necessary. Complete occlusion of the mesenteric artery initially leads to vasospasm in the ischaemic area, inducing hyperperistalsis accompanied by paroxysmal abdominal pain. Simultaneously, a vicious cycle is established at the cellular level, leading to enhanced metabolism in the ischaemic zone, formation of oxygen free radicals and secondary mucosal cell disintegration. After 3–6 hours, the peristaltic cycle stops and a pseudo-painless mild interval begins, which results from ischaemic damage to nociceptive receptors in the intestinal wall. In the final stage, the mucosal defect becomes irreversible. As inflammatory cells infiltrate the intestinal wall, bacteria migrate, leading to intestinal gangrene. As the disease progresses, diffuse peritonitis, intestinal obstruction, sepsis and multi-organ failure may develop. Therefore, early recognition is paramount.
During ECMO, the ECMO access and pump compromise multiple inherent primary and secondary haemostatic mechanisms. Therefore, bleeding and thrombotic complications plague clinicians and affect patient prognosis. Some studies have shown that during ECMO, the bleeding rate is 29%, with 10% of patients experiencing life-threatening major bleeding and 4%–10% experiencing intracranial haemorrhage.8,9 Also, there is a 10%–16% chance of thrombosis during ECMO. Extracorporeal Life Support Organization guidelines recommend that heparin anticoagulation should be used during ECMO to minimise thrombosis formation.10 Both of our patients experienced AMI, underwent PCI and were anticoagulated according to international guidelines. Antiplatelet agents were reduced during treatment because of gastrointestinal bleeding and low platelet counts, and no lower-extremity venous thrombosis was detected; however, ileal ischaemia and necrotic perforation developed, and mesenteric artery embolism was considered postoperatively. We refer to the treatment protocol for acute mesenteric thrombosis, where heparin should be started after diagnosis to prevent thromboembolic occlusion of the intestinal arteries. It is recommended to administer 2,000 IU heparin intravenously, followed by 5,000–10,000 IU heparin continuously over 24 hours to control the activated partial thromboplastin time (aPTT) to 60 seconds.11 A balance between anticoagulation and controlling the risk of bleeding needs to be achieved in these patients. Patients on ICU often require high doses of vasopressors and may demonstrate coagulation disorders. In such cases, the doses of vasoactive drugs should be reduced by aggressive volume supplementation.12 Ideally, the use of vasoactive drugs should be minimised, especially of those that reduce blood flow to the abdominal organs.
For patients undergoing ECMO, if open surgery is traumatic, early intervention and endovascular treatment at the stage of mesenteric ischaemia will greatly improve patient prognosis and shorten the ECMO evacuation time. Some studies have shown that the rate of complications in patients after endovascular intervention is reduced to 23%–26%, compared with 36%–56% after open surgery.13,14 It can also reduce the incidence of postoperative short bowel syndrome, so early detection and treatment are desirable.
Although ideal, early detection of this condition is difficult. Most patients who undergo ECMO after E-CPR have ischaemic–hypoxic encephalopathy due to a long period of ischaemia and hypoxia, which leads to pain insensitivity. Moreover, patients who undergo ECMO tend to be treated with sedative and analgesic drugs, which make it difficult to identify intestinal ischaemia early. Thus, systematic clinical monitoring is needed to detect early evidence of intestinal ischaemic obstruction. Early imaging is usually performed with ultrasonography or bedside X-ray, which have poor specificity compared with CT. Diagnostic signs on plain CT include reduced or absent intestinal wall enhancement and gas in the intestinal wall, but these signs are rarely seen. The common manifestations are intestinal wall thickening, intestinal lumen dilatation and intra-abdominal fluid accumulation; however, these are non-specific to this condition.15
When acute mesenteric embolism is suspected, SMA CT angiography is the diagnostic method of choice. This method is universally available and time-saving, and has high diagnostic value for all abdominal diseases (sensitivity of 93%, specificity of 100%, positive predictive value of 94% and negative predictive value of 100%).16 However, ECMO causes blood flow changes; thus, contrast-enhanced CT is difficult and the risk associated with transporting ECMO-assisted patients can be high. There is an urgent need for more sensitive methods to monitor bowel function, and we will address this concern in the next phase of our work. Other diagnostic tools, such as abdominal ultrasonography, abdominal X-ray, catheter angiography and magnetic resonance imaging, are time-consuming and do not provide a complete picture of all abdominal organs. Laboratory tests with sufficient sensitivity and specificity are limited in their diagnostic performance. A previous study suggested elevated lactate as a sign of acute mesenteric embolism, but with poor specificity. However, in patients with colorectal or peripheral ischaemia, lactate can be normal.17 In this study, we attempted to identify similarities between the two patients; both had AMI, prolonged periods of hypoperfusion, arrhythmia and high intra-abdominal pressure during ECMO, which seems to be a cause for alarm in such patients.
In conclusion, we report two patients with intestinal ischaemic perforation to alert clinicians to the possibility of this complication and to encourage early detection and intervention to improve prognosis. In the past, the gastrointestinal tract often received secondary attention in patients receiving ECMO support because the vital organs tend to be considered first. However, it is important to monitor abdominal signs. Monitoring methods with higher sensitivity are required, and the use of enhanced abdominal CT should be actively pursued.
Funding
This study was funded by the Construction Fund of Medical Key Disciplines of Hangzhou (OO20200485).
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.