
ABSTRACT
Meningitis remains an important cause of mortality and morbidity. Clinicians should be alert to this diagnosis and have a low threshold for investigation and treatment of meningitis. This article provides an update of current evidence and existing guidelines for the management of suspected acute meningitis in adults in the UK.
Key points
Lumbar puncture should be performed as soon as possible in all cases of suspected meningitis, unless contraindicated, in order to determine the aetiology, guide treatment decisions, and prevent unnecessary treatment and prolonged hospital stays.
Brain imaging is not required in the majority of cases prior to lumbar puncture and results in unnecessary delays in lumbar puncture and antibiotic initiation.
Steroids should be initiated just prior to or in conjunction with antibiotics in all cases of suspected bacterial meningitis.
Important risk factors for specific aetiologies should be ascertained and guide empirical antibiotic decisions; for example, relative immunocompromise including age >60 years, chronic disease and alcohol excess (risk of Listeria monocytogenes) and a travel history to areas with a high incidence of penicillin-resistant Streptococcus pneumoniae.
Mortality from bacterial meningitis remains significant and future treatments are being developed that aim to reduce the inflammation associated with the disease.
Definitions
Meningitis is inflammation of the meninges and is a pathological diagnosis. Elevated cerebrospinal fluid (CSF) leukocytes and proteins are used as proxy markers of inflammation. Bacterial or viral meningitis are diagnosed when the relevant pathogen is identified in the CSF along with an appropriate clinical syndrome and evidence of inflammation in the CSF.1
Aetiology
A viral cause is identified in up to half of meningitis cases where a cause is found.2 Enteroviruses are the most common cause followed by herpes simplex virus (HSV) and varicella-zoster virus (VZV). Less common causes can be linked to travel such as Toscana virus.2–4 Many cases of viral meningitis are assumed when no pathogen is detected.
Streptococcus pneumoniae and Neisseria meningitidis are the most common bacterial causes in the UK. Other causes such as Haemophilus influenzae, Listeria monocytogenes, Mycobacterium tuberculosis and fungi are less common. In up to 40% of patients, no cause is identified.2,3,5
Clinical features
Clinical features of meningitis alone cannot be used to discriminate between viral and bacterial meningitis. One study showed that 95% of patients with bacterial meningitis had at least two out of fever, headache, neck stiffness or altered consciousness but these can also occur in other diagnoses.5,6 Therefore, meningitis should be considered in any patient presenting with two or more of these symptoms but lumbar puncture (LP) is essential, unless contraindicated, to diagnose or rule out meningitis, and to determine the aetiology.
Certain features can make a specific aetiology more likely. A rash is seen in approximately half the cases of meningococcal meningitis but can be seen in other causes of viral and bacterial meningitis.2 Listeria meningitis is more likely with a history of relative immunocompromise (such as older age, diabetes, chronic disease and alcohol excess) as well as overt immunocompromise.7 Other important points include travel history, HIV status, extra-meningeal foci of infection (such as otitis and sinusitis (more common in pneumococcal meningitis)), features of sepsis or contact with another meningitis case.1,6
Investigations
Lumbar puncture
LP is the key investigation as it enables confirmation of meningitis and reveals the aetiology. In the UK, the median time from admission to LP is 17 hours despite national recommendations for an LP to be performed within 1 hour of arrival to hospital and preferably prior to antibiotics.3 The likelihood of detecting a pathogen decreases over time and, while getting an LP done within an hour is not always possible, it should be done as soon as is practically possible.2,8 In patients with predominantly sepsis or a rapidly evolving rash, LP is not recommended (Box 1).1
Contraindications to immediate lumbar puncture
Cerebrospinal fluid cell count
Van de Beek and colleagues reported that >90% of adults with bacterial meningitis had a CSF leukocyte count >100 cells/μL.6 Absence of leukocytosis makes meningitis unlikely, but does not rule it out. A Danish study found an absence of leukocytosis in 2% of patients with bacterial meningitis, with a higher frequency in pneumococcal meningitis, a finding that was replicated in a Dutch study, which found immunocompromise was also a risk factor.9,10
Cerebrospinal fluid leukocyte differential
A predominance of neutrophils in the CSF suggests bacterial meningitis while predominance of lymphocytes suggests viral meningitis. Important exceptions include a predominance of lymphocytes in bacterial meningitis if antibiotics have been given prior to LP and with certain bacteria (such as Listeria monocytogenes and in tuberculous meningitis).11 A predominance of neutrophils can be seen in early viral meningitis as well, especially with enterovirus.12
CSF biochemistry
CSF protein, glucose and lactate give an indication as to the aetiology of meningitis but are not definitive (Table 1).1 In a recent cohort study, a CSF:blood glucose ratio <0.6 detected all cases of bacterial meningitis but was not specific.5 A CSF protein of <0.6 g/L makes bacterial meningitis unlikely.13 CSF lactate has a high sensitivity and specificity in distinguishing between bacterial and viral meningitis if antibiotics have not been given beforehand, a cut off of 35 mg/dL has been suggested to have the best sensitivity for distinguishing between bacterial and viral meningitis.14
Cerebrospinal fluid parameters for different aetiologies of meningitis1
Clinical prediction models
A recent systematic review and validation of clinical prediction models found that none of the tested models had both sufficient sensitivity and specificity to be recommended for routine clinical use.15
Pathogen detection
CSF microscopy and culture
CSF microscopy with Gram stain is useful for rapid detection of bacteria. CSF culture is diagnostic in 70%–85% of cases prior to antibiotic exposure.11 However, in a recent UK study, CSF culture was positive in only 23% of cases of bacterial meningitis when the median time to LP was several hours after antibiotic administration.2 CSF sterilisation can occur within 2 hours and 4 hours of antibiotic administration for meningococci and pneumococci, respectively.8
CSF polymerase chain reaction
CSF polymerase chain reaction (PCR) can rapidly detect viruses and bacteria in the CSF with high specificity. It is the gold standard for detection of viruses and is increasingly relied upon in the diagnosis of bacterial meningitis, especially when antibiotics have been given prior to LP. Over 50% of meningococcal disease is diagnosed by PCR alone in the UK.16 Multiplex PCR, which can detect multiple pathogens at once, are increasingly being used with reasonable diagnostic accuracy reported.17
Whole genome sequencing techniques
Although not currently in routine clinical use, studies have shown that different sequencing methods on CSF identified unexpected pathogens not detected by conventional methods. However, they failed to detect some pathogens found by conventional microbiological testing.4,18 Further work is needed to evaluate the clinical impact of such techniques.
Blood tests
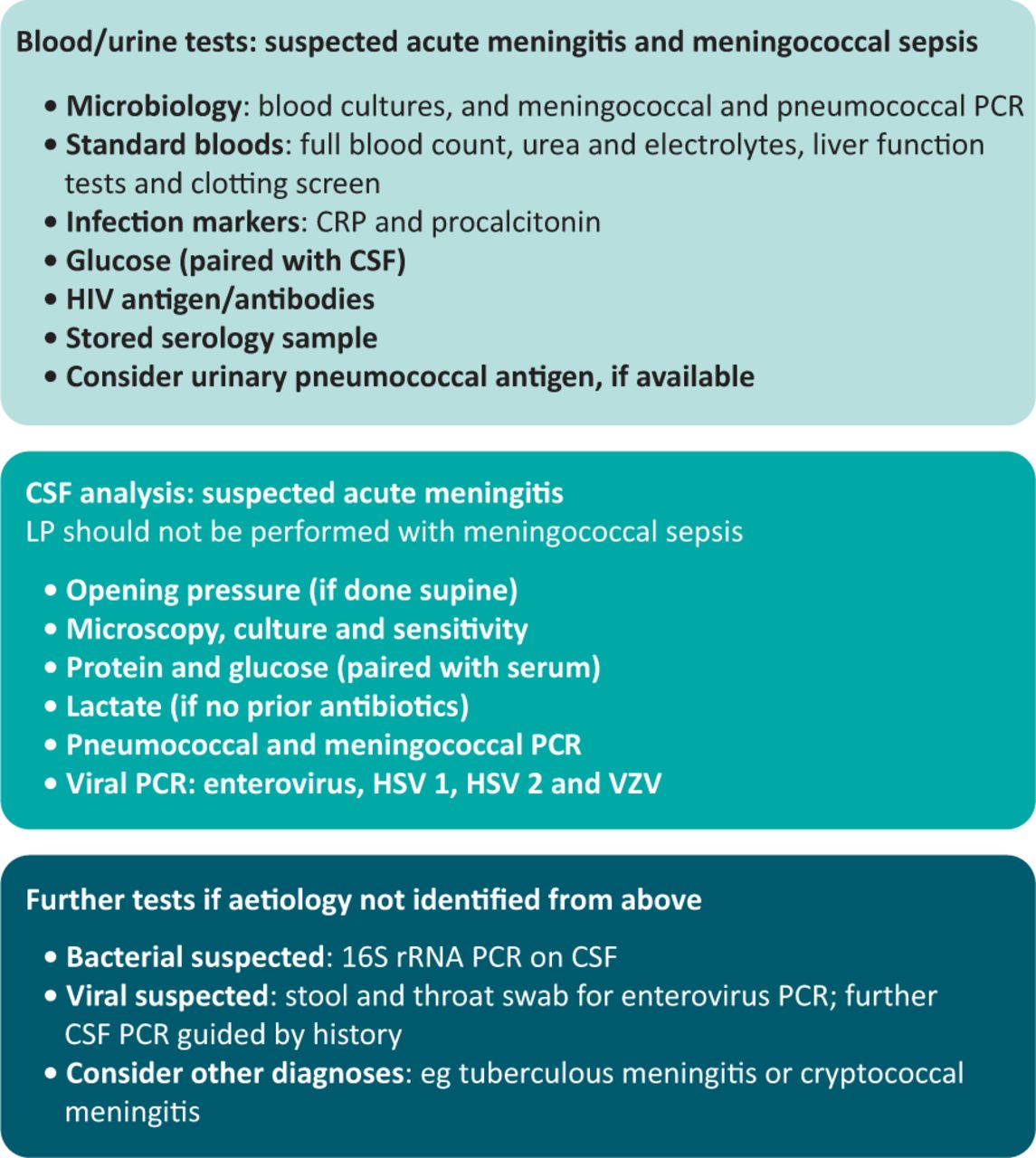
Blood cultures should be taken in all cases of suspected meningitis prior to administration of antibiotics (Fig 1).1 Blood meningococcal and pneumococcal PCR are also recommended and have been shown to substantially increase detection of meningococcal disease, and remain positive for several days after antibiotic initiation.2,19
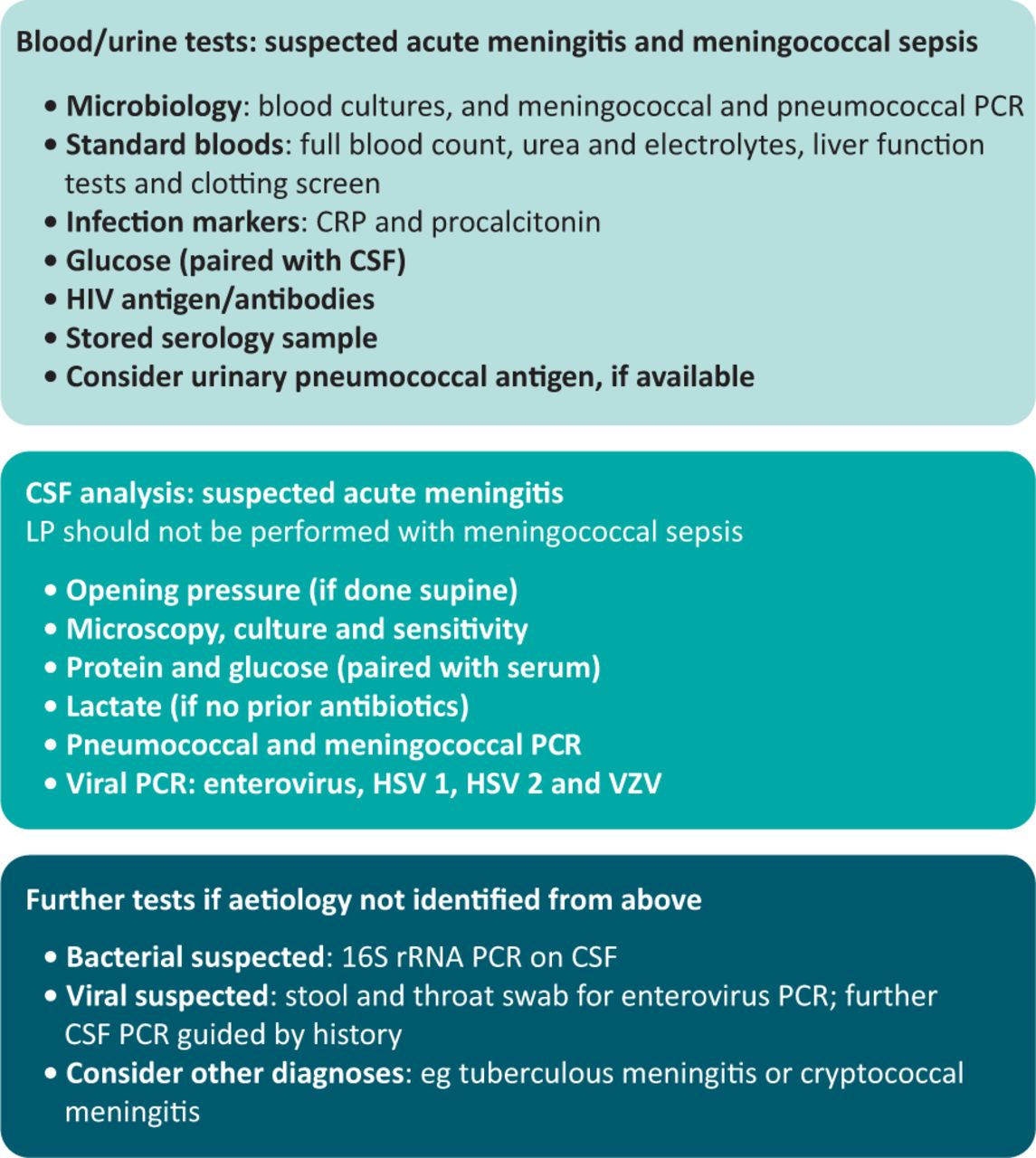
Recommended investigations in acute meningitis and meningococcal sepsis. CSF = cerebrospinal fluid; CRP = C-reactive protein; HSV = herpes simplex virus; LP = lumbar puncture; PCR = polymerase chain reaction; rRNA = ribosomal ribonucleic acid; VZV = varicella-zoster virus. Adapted with permission from McGill F, Heyderman RS, Michael BD et al. The UK Joint Specialist Societies Guideline on the diagnosis and management of acute meningitis and meningococcal sepsis in immunocompetent adults. J Infect 2016;72:405–38 under CC BY-NC-ND 4.0 licence.
Although some studies have shown procalcitonin has good sensitivity and specificity for differentiating bacterial from viral meningitis, it should be interpreted with the rest of the clinical picture not be the sole determinant.20
Swabs
Throat, nasopharyngeal and stool swabs are useful for detecting enteroviruses if the CSF PCR is negative. Methicillin-resistant Staphylococcus aureus screening swabs should be taken. A bacterial throat swab should also be taken from cases with suspected meningococcal disease to provide information about the infecting strain in PCR-confirmed cases.1
Brain imaging
In the majority of cases of suspected meningitis brain imaging is not required and LP can be performed without. Despite this, a UK study showed that 94% of patients had brain imaging prior to LP and an earlier study showed brain imaging resulted in delays in LP of 10 hours.2,3 Furthermore, brain imaging prior to LP results in delays to antibiotic initiation, which leads to increased mortality.21 An urgent computed tomography should be performed if there are clinical signs of brain shift that may indicate a contraindication to LP. When brain shift is identified, liaison with critical care and neurosurgical teams are essential.1 Imaging should also be considered if there has been a deterioration following an initial improvement to look for complications, such as subdural empyema.
Treatment
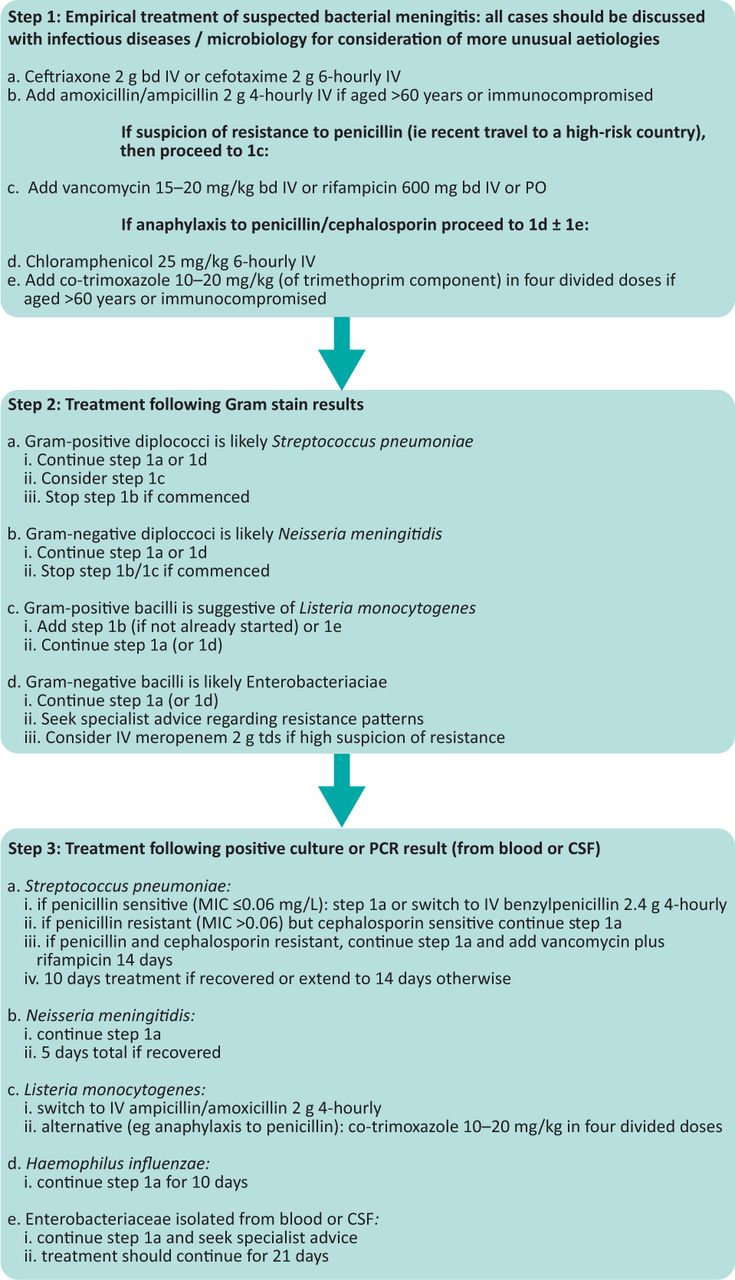
Stabilisation of the patient's airway, breathing and circulation is an immediate priority. The patient's consciousness level should be documented using the Glasgow coma score (GCS). A decision regarding the need for senior review and/or intensive care admission should be made within the first hour. A GCS ≤12 should prompt discussion with critical care for consideration of intubation. All patients should be cared for with input from an infection specialist (Fig 2).1
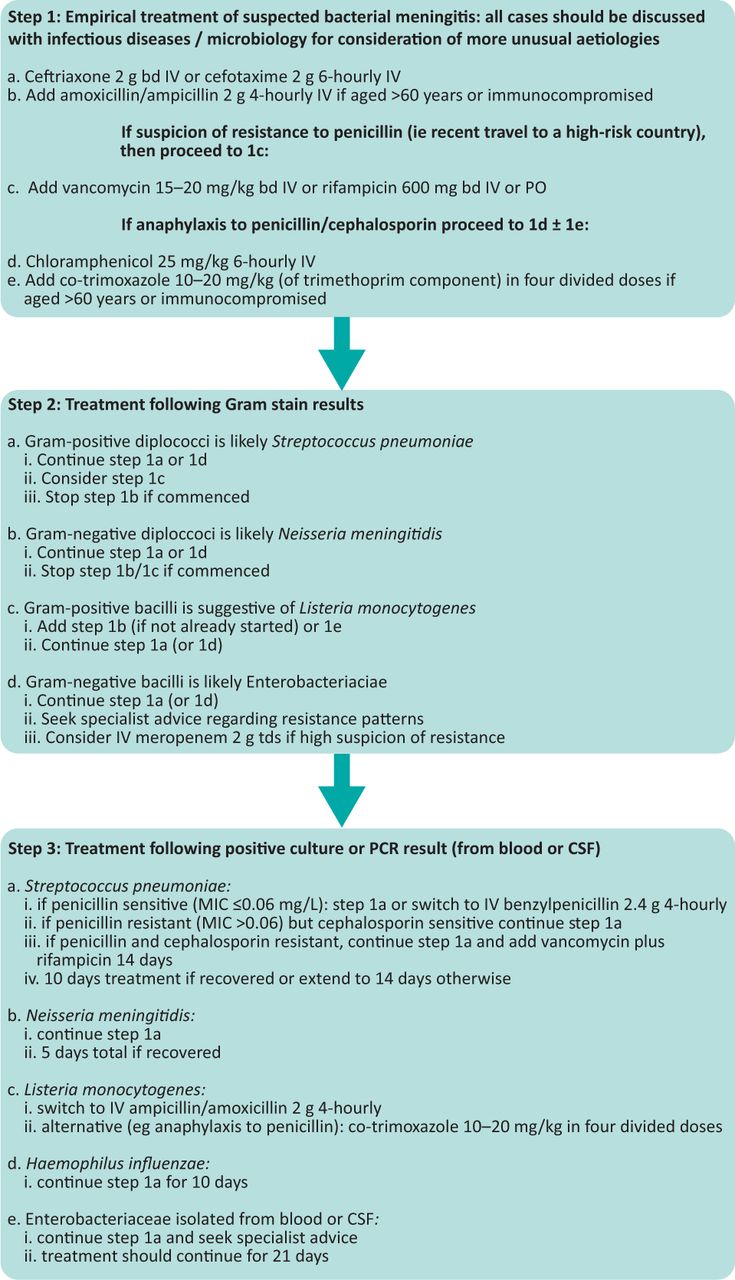
Antimicrobial treatment algorithm. aSerum vancomycin trough concentrations of 15–20 μg/mL should be aimed for. bd = twice a day; IV = intravenous; MIC = minimal inhibitory concentration; PO = per oral; tds = three times a day.
In patients with predominantly sepsis or a rapidly evolving rash, antibiotics should be given immediately after blood cultures have been taken. The surviving sepsis guidelines should be followed in patients with sepsis.22 A recent meta-analysis has shown that delays of over 2 hours in antibiotic administration in bacterial meningitis are associated with a doubling in mortality.21 Therefore, antibiotics should be administered as soon as possible and certainly within 2 hours in suspected meningitis without sepsis.
Steroids
A Cochrane review found that steroids led to a small reduction in mortality in pneumococcal meningitis and reduced hearing loss and neurological sequelae for all causes.23 They concluded that current data supports their use in high-income settings in acute meningitis but not in low-income settings.23
Current UK guidance recommends that intravenous dexamethasone 10 mg 6 hourly should be commenced on admission shortly before or simultaneously with antibiotics and up to 12 hours after for patients with suspected meningitis.1 Compliance with this recommendation in the UK is poor, with only 20% of patients given steroids.3 If pneumococcal meningitis is confirmed, dexamethasone should be continued for 4 days.
Antibiotic choice
Consideration should be given to patient risk factors. In those with relative or overt immunocompromise (see details earlier), amoxicillin/ampicillin should be added to cover Listeria. A recent UK study showed that only 28% of patients aged >60 years and 31% of those immunocompromised received anti-listerial antibiotics.3 In those with a travel history to an area with a high prevalence of penicillin-resistant pneumococci, then vancomycin or rifampicin should be added.1
Viral meningitis
There is no specific treatment for viral meningitis, but clinical trials are lacking. Treatment with aciclovir is of proven benefit in herpes encephalitis, therefore, if the patient has encephalitic features, aciclovir should be given. A prospective observational study in the UK showed that 43% of patients with HSV/VZV meningitis received ≥5 days of antivirals despite no evidence showing benefit.2
New treatments
The mortality associated with meningitis is still 10%–20%, much of this is due to associated inflammation. Current trials are aimed at reducing inflammation. An ongoing randomised trial is assessing whether the addition of daptomycin to standard treatment improves outcomes.24 Daptomycin is primarily being used for its anti-inflammatory properties in this context rather than its antimicrobial ones.25 Pre-clinical studies have shown that adjuvant treatment with C5 inhibitors dampen down complement-associated damage and improve outcomes in an experimental model of pneumococcal meningitis.26
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}