
ABSTRACT
Background Serious incident (SI) investigations aim to identify factors that caused or could have caused serious patient harm. This study aimed to use the Human Factors Analysis and Classification System (HFACS) to characterise the contributory factors identified in SI investigation reports.
Methods We performed a content analysis of 126 investigation reports from a multi-site NHS trust. We used a HFACS-based framework that was modified through inductive analysis of the data.
Results Using the modified HFACS framework, ‘unsafe actions’ were the most commonly identified hierarchical level of contributory factors in investigation reports, which were identified 282 times across 99 (79%) incidents. ‘Preconditions to unsafe acts’ (identified 223 times in 91 (72%) incidents) included miscommunication and environmental factors. Supervisory factors were identified 73 times across 40 (31%) incidents, and organisational factors 115 times across 59 (47%) incidents. We identified ‘extra-organisational factors’ as a new HFACS level, though it was infrequently described.
Conclusions Analysis of SI investigation reports using a modified HFACS framework allows important insights into what investigators view as contributory factors. We found an emphasis on human error but little engagement with why it occurs. Better investigations will require independence and professionalisation of investigators, human factors expertise, and a systems approach.
Introduction
Over 1.4 million patient safety incidents (defined as events that cause or could cause harm to patients) are reported to NHS England annually.1 More than 20,000 are classed as ‘serious’ according to their level of harm or their potential to cause serious harm.2 Those adverse events classed as ‘serious incidents’ (SIs) are required to be notified to local commissioners of healthcare services and undergo a structured investigation led by the healthcare organisation where the incident occurred, with the aim of determining contributory factors (see supplementary material S1).
One commonly used approach for investigating adverse events in high-risk industries (including healthcare) is root cause analysis (RCA).1,3 RCA seeks to provide an analytical framework for investigators to construct an understanding of what happened and why, with the aim of identifying underlying causes and informing future preventive actions.1 In the English healthcare context, RCA investigations are usually undertaken by in-house investigators who gather evidence from varying sources (eg medical records, interviews and statements) and establish a timeline of key facts. An analysis of factors that appear to have contributed to the incident is then undertaken using various RCA tools (eg fishbone diagrams or five whys).4,5 Finally, recommendations are generated and an action plan formulated.6
Previous research on incident investigations has typically focused on analyses of particular classes of incident (eg adverse drug reactions or inpatient suicides) or of specific specialties (eg intensive care).7–9 These studies have produced valuable learning about what investigators identify as contributing factors for incidents in specific areas. However, study at the organisational level (agnostic to class of incident or specialty) has remained limited despite criticisms that RCAs may fail to identify and address systemic issues within organisations across multiple incidents.10,11
To understand what investigators report as factors contributing to SIs at an organisational level, a structured framework is of potential benefit. Though several options are available, an important example of such a framework is the Human Factors Analysis and Classification System (HFACS).6,12–15 HFACS builds on Reason's Swiss cheese model by providing taxonomies for active failures and latent conditions, divided into four levels: unsafe actions, preconditions for unsafe acts, unsafe supervision and organisational influences.16 Each level comprises several sub-levels corresponding to aspects of human behaviour or properties of systems that may contribute to an error.14 Originally developed for accident analysis in aviation, HFACS demonstrates good analytic properties and has been modified for use in healthcare.15,17–19 Isherwood et al are among those who propose that HFACS-based frameworks have particular value in healthcare, facilitating the identification of system-based actions that can help reduce the likelihood of future serious incidents.20
We conducted a structured analysis of investigation reports from different specialties using a modified HFACS framework in a multi-site English hospital trust to characterise the kinds of contributory factors identified by investigators in these reports.
Methods
Setting
The study was located at a large teaching hospital trust with over 10,000 staff looking after over one million patients per year. It followed the SI reporting process, investigation techniques and reporting templates set out by the NHS SI framework policy.1
Data collection and sample
A search was carried out in July 2016 of the trust's risk management software (RLDatix (formerly Datix)) to identify anonymised SI investigation reports presented to local commissioners between 01 January 2013 and 31 December 2015. The sample did not include investigations that were still ongoing. It also excluded investigations into pressure ulcers and healthcare-associated infections (such as Methicillin-resistant Staphylococcus aureus bacteraemia or Clostridioides difficile) as these events were locally investigated using different processes. Each report included in the sample covers an individual incident. Each was expected to be prepared using the guidelines of the SI framework from NHS England though, in practice, the formats varied somewhat.1 Typically, each SI investigation report included a background to the incident, a chronology of key events in the care of the patient, a breakdown of service and care delivery problems as identified by investigators, the root causes, and the actions taken.1
Data analysis
Data analysis involved two stages, involving inductive and deductive approaches (Fig 1), led by two researchers with expertise in qualitative research and incident investigation.21 One researcher had additional training on use of HFACS. No researcher had been involved in any of the investigations studied.
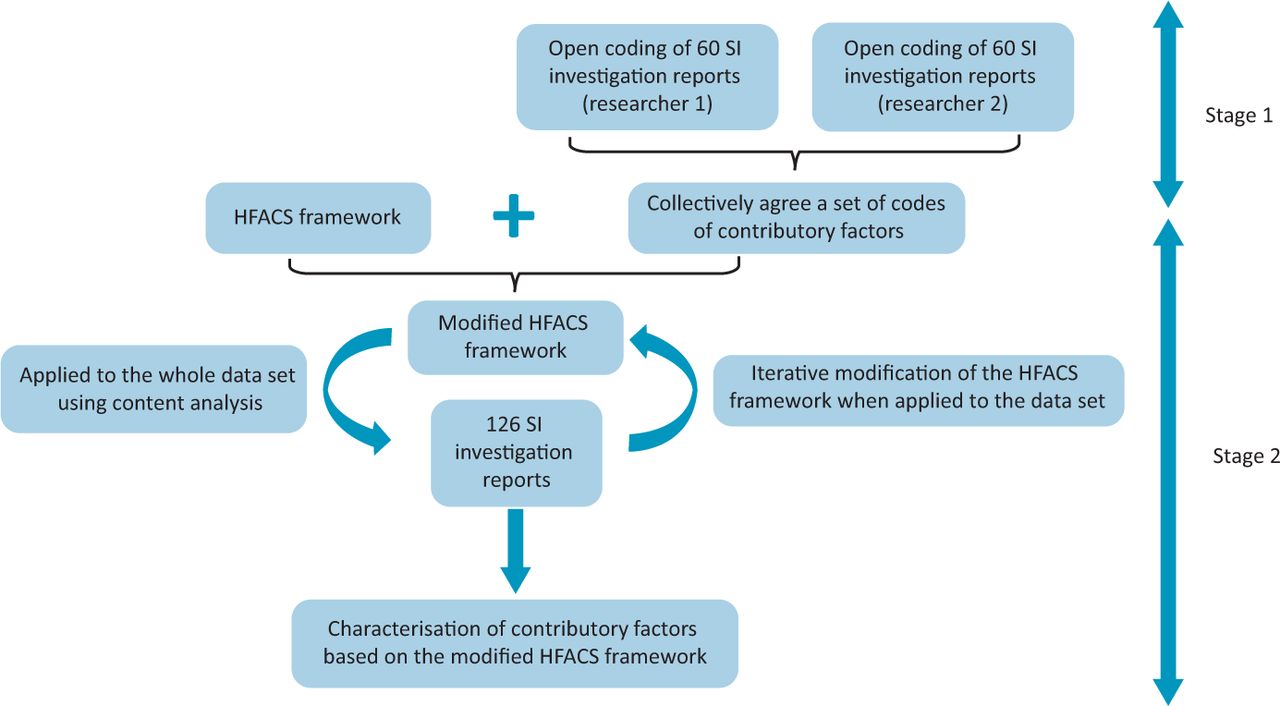
Data analysis process. HFACS = Human Factors Analysis and Classification System; SI = serious incidents.
Stage 1: Open coding of SI investigation reports
Using an inductive approach, two researchers analysed a sub-sample of 60 SI investigation reports independently by reading and re-reading them to familiarise themselves with the data before performing open coding of contributory factors from the SI investigation reports.22 In keeping with qualitative research norms, they compared their coding to reach consensus.23 A third researcher was available when consensus could not be reached or where ambiguities remained.
Stage 2: Content analysis of contributory factors using a HFACS framework
We started by using a HFACS framework that was previously developed in a healthcare context and used the open codes from stage 1 to make some initial adjustments.15 This version of the framework was modified iteratively following interaction with successive SI investigation reports to produce a modified HFACS framework (Fig 2 and supplementary material S2). All included SI investigation reports were analysed using this modified HFACs framework based on the principles of content analysis.24 Data analysis was supported by NVivo (QSR International, Burlington, USA). Simple descriptive statistics were generated to report the frequencies of different types of incidents as reported in the SI investigation reports, roles of members of the investigating teams, departments and patient outcomes.

Modified Human Factors Analysis and Classification System.
Research ethics
The study was deemed not to require ethical board approval according to the decision tool from the NHS Health Research Authority website (www.hra-decisiontools.org.uk/ethics) and was registered with the trust's audit and service evaluation team (project 6545).
Results
We identified 126 investigation reports into SIs that met the inclusion criteria for the period studied: 36 in 2013, 50 in 2014 and 40 in 2015. The incidents had been investigated by teams mostly comprising representatives from the trust's patient safety team (115 (91%)), consultants (109 (87%)) and senior nurses (band 7 or above; 85 (67%)). Human factors specialists were involved in three (2%) investigations.
Characteristics of the incidents investigated
The two most frequently occurring incident types were ‘inpatient falls’ (15 (12%)) and ‘delayed or missed diagnosis of other (non-cancer) condition’ (15 (12%); Table 1). Emergency medicine (18%), and obstetrics and gynaecology (15%) were the two specialties most commonly involved based on the SI investigation reports (Table 2). Table 3 shows the patient outcomes from the SIs, with ‘death’ the most frequent outcome (37 (29%)). Twenty-seven (21%) cases resulted in no harm.
Ten most common types of serious incidents from investigation reports generated between 2013 and 2015
Five most common specialties involved in the serious incident investigation reports reviewed between 2013 and 2015
Degree of harm to patients in serious incident investigation reports reviewed that had occurred between 2013 and 2015
Content analysis of contributory factors using the modified HFACS framework
The final framework produced by our inductive and deductive analysis (modified HFACS; Fig 2) comprised five levels: extra-organisational factors, organisational factors, supervisory factors, preconditions for unsafe acts and unsafe actions. Each level was further divided into numerous sub-levels of contributory factors (supplementary material S2).
Using this framework, we identified 701 contributory factors (median per incident 4 (interquartile range 2–7)) across the 126 SI reports. Table 4 provides a breakdown of frequencies and percentages of the five different levels of contributory factors and their respective sub-levels, accompanied with illustrative excerpts from the SI investigation reports. We provide descriptions of each level in supplementary material S2.
Frequencies of different levels of the modified Human Factors Analysis and Classification System framework and corresponding textual extracts
Unsafe actions
The most commonly identified level of contributory factor in the reports was ‘unsafe actions’, comprising errors and violations. We identified that ‘unsafe actions’ were reported 282 times across 99 (79%) incidents.
We identified that errors (defined by Diller et al as mistakes, unintentional slips and lapses (action-based errors and perceptual errors) or conscious actions that proceed as intended but were inappropriate for the situation (decision-based errors)) were reported 162 times across 79 (63%) incidents.15
Decision-based errors in the reports related to inadequate clinical decision-making (eg due to poor judgement and cognitive biases; Table 4, extract 1), though deeper insights into the rationale for poor decision-making were rarely provided by investigations. Action-based errors (unintentional slips and lapses made during the execution of seemingly familiar tasks) were reported to have occurred despite controls in place to mitigate risk, such as checklists and guidelines (Table 4, extract 2). Perceptual errors, such as important clinical information being missed or misinterpreted by staff, were rarely identified in investigation reports. When described, they were found in medication prescribing and administration, and interpretation of radiological imaging (Table 4, extract 3).
Routine violations in the reports characteristically involved poor documentation practices (Table 4, extract 4) and non-compliance with written policies and guidelines. Exceptional violations (failures to perform critical job activities) included delays in responding to emergencies or acting upon results (Table 4, extract 5).15 Investigation reports did not probe into the rationales for either type of violation.
Preconditions for unsafe acts
We identified ‘preconditions for unsafe acts’ reported 223 times across 91 (72%) incidents, comprising five sub-levels: environmental factors, communication factors, patient factors, factors relating to staff wellbeing and issues with team dynamics.
We deemed environmental factors to be physical, technological and cultural (based on local context) in nature. Physical environmental factors included those relating to the settings within which patient care was delivered, eg high levels of activity in clinical areas leading to overstretched resources (Table 4, extract 6). Technological factors concerned issues with the design and usability of IT systems and equipment, lack of inter-operability between software solutions (Table 4, extract 7) and poorly designed hardware, including some hazards that had already been identified nationally (Table 4, extract 8). Local cultural factors included the normalisation of potentially unsafe practices, such as workarounds when completing checklists (Table 4 extract 9).
We identified communication factors as contributory factors in the incident investigation reports at all organisational levels (micro-level (between members of the same team such as at shift handovers), meso-level (between departments) and macro-level (between organisations)). Poor communication was reported to result in lack of shared mental models of evolving clinical situations (Table 4, extract 10). When investigators did probe the rationales for communication failures, a recurring finding was lack of training among staff members on how to use clinical and administrative systems in place. Such training deficiencies were identified in relation to some widely used tools in healthcare, such as the World Health Organization (WHO) surgical safety checklist (Table 4, extract 11).
Supervisory factors
‘Supervisory factors’ in the reports comprised those decisions and actions made by staff in positions of authority at a departmental level that adversely affected performance in the organisation and delivery of healthcare.14,15 Of the five broad levels of contributory factors, supervisory factors were reported least frequently (73 instances across 40 (31%) incidents). We deemed unsafe supervision to be due to inappropriate planning, poor oversight, failures to address known problems and supervisory violations (Table 4, extracts 16 to 19). The most frequently identified ‘supervisory factor’ was inappropriate planning, present in 19% of incidents. These instances led to patient-facing staff being overloaded with work and created unbalanced teams, ultimately leading to hazard-prone situations, sometimes despite prior warnings from patient-facing staff (Table 4, extract 16).
Organisational factors
‘Organisational factors’, which we identified in reports 115 times across 59 (47%) incidents, included actions and decisions made at the blunt end of the organisation that negatively impacted on patient safety. These factors affected operational choices made in individual departments and impacted on staff performance at the sharp end.14,15 We further distinguished them into three sub-levels, pertaining to issues with operational processes, resource management and organisational culture.
Poor operational processes included instances where decisions and rules (or lack thereof) from senior management ultimately undermined how the organisation functioned, frustrating its ability to deliver on goals for direct patient care. Examples included the absence or impracticality of guidelines and standard operating procedures, generating confusion among staff (Table 4, extract 20). Some organisational rules and practices had been in operation for some time, despite their apparent lack of effectiveness and, occasionally, deficient logic (Table 4, extract 21).
Issues relating to resource management consisted of inappropriate handling of organisational assets, leading to unsafe working conditions. A recurring issue was inadequate staffing leading to poor continuity of care, reduced supervision of junior staff and high caseloads (Table 4, extract 22).
As shown in Table 4, we rarely identified factors in the reports relating to organisational culture (ie shared ways of thinking, feeling and behaving across different departments in the trust). When organisation culture factors were reported, they included practices perpetuating hierarchical barriers that had remained unquestioned (Table 4, extract 23).
Extra-organisational factors
We identified a limited number of factors from the SI investigation reports that lay beyond the remit of the trust (eight references across seven (6%) incidents). This level was not previously described in the HFACS framework used by Diller et al.15 Though rarely explored by investigators, we identified examples of ‘extra-organisational factors’, including system-wide lack of resources (such as a lack of particular skills and limitations of national guidance; Table 4, extract 24).
Discussion
Our analysis, using a modified HFACS framework, characterised the contributory factors identified in 126 SI investigation reports over a 3-year period in an NHS trust. The findings should not be understood as providing an objective account of the true causes of incidents or their relative frequencies. Instead, the distinctive achievement of this analysis is to offer significant insight into what investigators see as contributory factors to incidents that they describe in investigation reports. Our findings raise questions about why investigation teams identify certain contributory factors more than others, about the absences or silences in the reports as well as what is made prominent, and about the potential biases that may influence investigators’ analysis. As Nicolini reminds us, cultural and organisational priorities are likely to colour the analytic lens that investigators apply.10
Notably, our analysis shows that there is an emphasis in investigation reports on problems occurring at the sharp end of care relating to, for example, clinical decision-making but little engagement with why they might occur. This may suggest an undue preoccupation with active errors and individual, rather than systemic, causes of incidents. Similarly, we identified reported instances of routine violations (such as poor documentation practices and non-compliance with written policies) in more than a third of SI investigation reports. However, the rationales for these violations and instances of normalisation of deviance (such as the influence of managerial decisions) were rarely explored in the investigation reports. Issues with supervision and organisational culture were identified much more rarely (making up 10% and 1% of all contributory factors, respectively) mirroring findings from other studies.15,18 Focusing on the more easily visible slips, lapses, mistakes and violations neglects the systemic origins of behaviours at the blunt end of care, may promote a blame culture and thwart learning.15,25
Another important emphasis in the reports was on environmental factors (identified in 44% of all SI investigation reports), such as poorly designed clinical spaces and technological problems. At the same time, silence largely prevails regarding the ‘extra-organisational factors’ (such as procurement practices or national standards) that might be implicated. In fact, previous iterations of the HFACS framework applied to healthcare data did not include a distinct level of contributory factors beyond the remit of organisations.15,18,19 Identification of such factors is of crucial importance in appropriate allocation of responsibility across the system and, in particular, avoiding assigning individual organisations the responsibility of solving such issues when they may not possess the power and resources to do so successfully.26
Implications for practice and policy
These findings have important implications for practice and policy. First, this study adds to the body of evidence for the utility of HFACS as a tool to provide insights into the levels of contributory factors identified from healthcare incident investigations.15,18,19 HFACS complements other frameworks, such as the Yorkshire contributory factors framework and the London protocol, offering an additional level of granularity and specificity.6,12 HFACS-based analysis may have a valuable role in sensitising investigators in understanding how factors at the blunt end of care influence those at the sharp end. A particular advantage demonstrated by our study is that HFACS analyses can be conducted at multiple levels (within specific specialties or organisations, and across a whole healthcare system) to prioritise targets for interventions.
We suggest that more attention should be paid in SI investigations to understanding how the physical, technological and cultural environment contributes to unsafe actions. This may mean more routinely involving human factors specialists in healthcare investigations. The limited availability of such expertise (one qualified human factors specialist for every 300,000 staff in the NHS in contrast to a ratio of one in 100 in the National Air Traffic Service) highlights the scale of work ahead.27 More broadly, these findings suggest that a move from individualisation of contributory factors to a more system-level understanding of causes of incidents is likely to be of benefit.
Linked to this, our findings indicate that investigations need to focus more on identifying ‘organisational’ and ‘supervisory’ factors, as well as those at the ‘extra-organisational’ level; a domain missing from previous HFACS frameworks. Many of those factors may not be easily addressed within departments and local healthcare organisations, and may require referral to national professional, regulatory or improvement bodies. We suggest that systems theory has much to offer to understand the interdependency of contributory factors arising across the whole healthcare ecology. Systems theory suggests that safety can only be appreciated when all the interactions between different components of a system are studied together.28 Examples of systems approaches used when investigating causes of incidents include Leveson's safety control structure, Rasmussen's AcciMap and hierarchical risk management.28,29
We also suggest that local investigators in NHS organisations should be independent of the department where the adverse events occurred. Such independence may allow investigators to question more ‘thorny’ issues (such as organisational culture and poor supervision) creating a more factual representation of ‘work-as-done’ in organisations, especially when things go wrong.30 A previous qualitative study of railway investigators highlights the value of independent investigators, empowering them to give a critical view of operations and provide recommendations without undue influence from organisation management.31
Lastly, we propose that SI investigations should be conducted by professionals whose expertise lie primarily in safety investigation and who also maintain a working knowledge of healthcare systems.32 This is in contrast to the current reality in healthcare where most investigators are healthcare workers with expertise in clinical and nursing domains with a secondary interest, and perhaps limited expertise, in safety. In England, the conduct of national safety investigations through the Healthcare Safety Investigation Branch (staffed with experts in different safety sciences), the creation of a national patient safety curriculum and the appointment of patient safety specialists in individual healthcare organisations with the role of overseeing safety related work are steps in the right direction.33,34 To improve individual healthcare organisations’ capacity and capability in investigating incidents robustly, we propose that local healthcare safety investigators need to have dedicated time in their job plans to conduct robust investigations and be supported to develop the skills required to do so.
Limitations
This study has some limitations. First, the results of the study may not represent a complete overview of all the contributory factors to SIs, as we applied a HFACS-based framework retrospectively to SI investigation reports that had themselves been produced using RCA findings of investigators. Next, our sample was limited to a single organisation between 2013 and 2015. Nevertheless, the commonality in results with other studies using HFACS-based frameworks suggests that the wider reproducibility of similar findings.15,18,19 Only 20% of the included SI investigation reports were from incidents involving no harm, highlighting a potential under-representation of near misses. Inclusion of more near misses in reports might have allowed a more transparent discussion of contributory factors. Relatedly, new guidance on patient safety investigations in England has been published since we conducted this analysis, prioritising the conduct of investigations based on the level of risk as opposed to the level of harm to patients.35
Conclusion
This content analysis of 126 SI investigation reports over a 3-year period from different specialties in a multi-site organisation using a modified HFACS framework provides important insights into the nature of contributory factors identified in reports, but also indicates that ‘extra-organisational factors’ should be included as a distinct level in the HFACS framework. There are indications from our analysis of excessive focus on individual behaviours and actions, to the neglect of systemic and organisational contributions to serious incidents. To improve the strength of SI investigations, we suggest the need for increased independence and professionalisation of investigators, wider involvement of human factors specialists and the use of systems theory during the conduct of investigations.
Summary box
What is known?
Previous qualitative analyses of incident investigations have looked at particular types of incidents and within specific specialties.
Research looking at identifying influences on incidents across different types of incidents and specialties is scarce, despite concerns regarding the strength of current methods (such as root cause analysis) used to investigate incidents.
What is the question?
Using the principles of content analysis, what are the contributory factors to serious incidents in healthcare, based on a modified Human Factors Analysis and Classification System (HFACS) framework?
What was found?
The most commonly identified level of contributory factors found from a content analysis of serious incident investigation reports, based on a HFACS framework, were at the sharp end of care, focusing on individual behaviours and actions, to the neglect of systemic and organisational contributions to serious incidents.
Through inductive analysis, we identified ‘extra-organisational factors' as a new level to the modified HFACS framework, though it was rarely detected by serious incident investigators.
What is the implication for practice now?
HFACS is a useful tool that provides deeper insights into commonly identified contributory factors to incidents and important factors missing from serious incident investigations.
Increased attention needs to be paid during the conduct of serious incident investigations to the role of environmental, organisational and extra-organisational factors on incidents.
More robust investigations will require independence and professionalisation of investigators, increased involvement of human factors experts and wider use of systems theory
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/clinmedicine:
S1 – Definition of serious incidents.
S2 – HFACS levels and modifications.
Funding
This study was funded by The Health Foundation's Improvement Science Fellowship. Mary Dixon-Woods and Graham Martin's contributions were funded by The Health Foundation's grant to THIS Institute (grant number RG88620). Mary Dixon-Woods is a National Institute for Health and Care Research (NIHR) senior investigator (NF-SI-0617-10026).
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}