
Introduction
A 47-year-old man presented to the emergency department with atraumatic acute onset lumbar back pain while attending a surfing lesson at an artificial wave lake. It occurred when transitioning from a prone position, with a hyperextended back, to standing on the surfboard, a manoeuvre known as ‘popping up’. Upon exiting the water, his pain worsened with acute lower limb weakness and a deep cold sensation in both feet. Weakness progressed to a nadir 1 hour from onset. He subsequently went into urinary retention several hours later requiring catheterisation.
There were no preceding back issues or discrete neurological episodes. He had no medical history and took no regular medications. He had no vascular risk factors and denied recreational drug use.
Examination revealed trepidation during gait inspection without the ability to walk on his heels or toes. Romberg's test was negative. Lower limb tone was normal, with a mild bilateral pyramidal weakness at hip flexion (4+/5), knee flexion (4+/5) and ankle dorsiflexion (4+/5). Plantars were flexor and reflexes were symmetrically brisk on admission. The right plantar became extensor on day 2 without clinical progression of symptoms. Pinprick, light touch and temperature sensations were diminished in the right leg to the tibial tuberosity and the left to the mid-shin. Posterior column sensory modalities were preserved. Upper limb and cranial nerve examinations were normal. Vital signs were stable and lower limb pulses were present.
Spinal magnetic resonance imaging (MRI) revealed a long ‘pencil-like’ T2 hyperintense signal within the anterior and central grey matter from T9/T10 to the conus consistent with anterior spinal cord ischaemia (Fig 1). There was an additional tear in the annulus fibrosus at L5/S1 with a non-compressive paracentral disc herniation raising the possibility for a fibrocartilaginous embolism. There was no evidence of vascular malformation. Routine admission blood tests were normal.
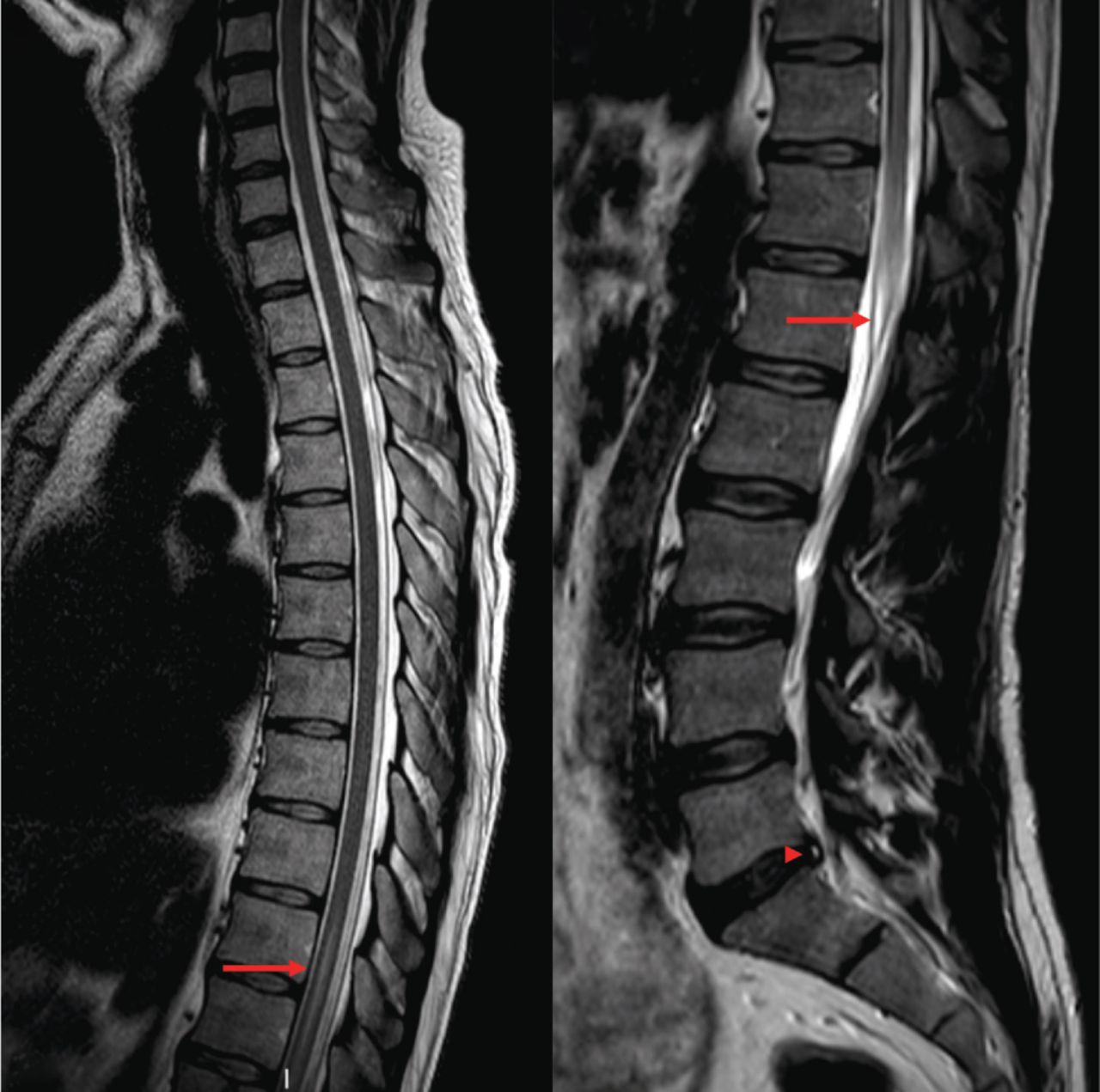
Spinal magnetic resonance imaging showing anterior spinal cord ischaemia following surfing.
Given the rapid clinical presentation and classical radiological features, precipitated during a novice surfing lesson, a diagnosis of surfer's myelopathy was established. Alongside early neurorehabilitation, he was managed with aspirin 300 mg for 2 weeks followed by 75 mg lifelong. His lower limb symptoms resolved on day 2 with full ambulation and he was discharged with a flip-flow catheter and urological follow-up.
What is the mechanism of spinal injury in surfer's myelopathy?
Acute disc herniation.
Myelitis (spinal inflammation).
Spinal cord ischaemia.
In view of the symmetrical lower limb pyramidal findings (ie brisk reflexes, extensor plantar and lower limb flexion weakness), together with spinothalamic sensory involvement, back pain and urinary retention, an upper motor neuron pathology localising to the anterior spinal cord should be suspected. An acute anterior spinal cord syndrome would be most in keeping with a vascular event, such as spinal cord ischaemia.
Prolonged prone spinal hyperextension on the surfboard (Fig 2) is thought to compress the artery of Adamkiewicz, or its radicular arteries, supplying the anterior portion of the spinal cord. The artery of Adamkiewicz typically arises from the left side of the aorta between T8 and L2. It is the only major arterial supply to the anterior spinal artery along the lower thoracic, lumbar and sacral segments of the spinal cord. In the lower thoracic region, the anterior spinal cord is most susceptible to an ischaemic event due to the inadequate collateral vascular supply. Spinal arteries lie on mobile structures that make them prone to mechanical damage.1 Injury to the artery of Adamkiewicz is well described and can cause neurologic damage with sphincter involvement, impaired motor function, and loss of pain and temperature sensation one level below the lesion.2

Prone hyperextension of the spine while surfing. This image illustrates the angle closure of the back during hyperextension that is thought to contribute to vascular compromise of the anterior spinal cord.
Alternative theories have been proposed, which may or may not occur concomitantly, including impaired venous return through compression of the inferior vena cava and fibrocartilaginous embolism (FCE). FCE is thought to occur in the context of Valsalva manoeuvres or increased axial loads that facilitate avulsion of the fibrocartilaginous nucleus pulposus and subsequent embolisation into the local spinal vasculature generating ischaemia.1
Myelitis (spinal inflammation) is an incorrect term for patients presenting with a rapid-onset symmetric cord syndrome in the context of novice surfing and without evolution of symptoms. Inflammatory processes present with progression of symptoms over many hours to 2 weeks and typically do not reach neurological nadir within 1 hour.
What principle diagnostic test is most helpful?
Lumbar puncture.
Spinal angiography.
Spinal MRI.
A spinal MRI is the immediate necessary investigation, given the hyperacute presentation, to assess for an anterior spinal cord infarct and exclude structural pathologies such as acute disc herniation or spinal cord haematoma. With specific reference to an acute myelopathy while surfing, studies have suggested likely unyielding investigatory results from inflammatory bloods and lumbar punctures with spinal MRI being the principle diagnostic test.3,4 A long ‘pencil-like’ T2-weighted hyperintensity in the anterior spinal cord is typically seen in surfer's myelopathy. Diffusion-weighted MRI sequences can be used to corroborate spinal cord ischaemia; however, this can be marred by physiological cerebrospinal fluid flow-induced artefact.5
What is the management of surfer's myelopathy?
Conservative management.
Steroids.
Surgical management.
Conservative management in the form of neurorehabilitation is the core treatment for surfer's myelopathy. Steroids, mean arterial pressure maintenance to >85 mmHg for ≥24 hours, and angiography with the prospect for tissue plasminogen activator or nicardipine (for thrombosis in situ and vasospasm, respectively) have been tried with mixed results.6,7 Prognosis is largely dependent on the degree of the spinal cord injury and neurological deficit at its nadir.7 In essence, surfer's myelopathy presents similarly to an acute spinal stroke and, given the vascular theory in addition to neurorehabilitation, our patient received aspirin 300 mg daily for 2 weeks followed by regular aspirin 75 mg.
Discussion
Surfer's myelopathy was first coined by Thompson et al in 2004, where a case series of nine first-time surfers, with no past medical history and structurally normal spines, presented with an acute spinal syndrome.3 In all patients, clinical features included non-traumatic back pain with varying degrees of progressive paraesthesias and paraparesis/-plegia, reaching its nadir within 1 hour. Urinary retention was a common feature. A spinal MRI typically shows anterior ‘pencil-like’ signal change from the lower thoracic region to the conus.
The pathophysiology is thought to be related to spinal cord ischaemia secondary to prolonged prone hyperextension of the spine that occurs while surfing and exacerbated by Valsalva when ‘popping up’ on the surfboard. Indeed, novice surfers are more likely to spend time in hyperlordosis without sitting on their surfboard between waves.1 This mechanical phenomenon has also been documented in other sports including gymnastics, yoga or pilates.6
Although rare and poorly recognised, surfer's myelopathy is a more frequent complication of the sport than being attacked by a shark or struck by lightning.6 The most effective management may be education in the novice surfing community to avoid excessive prone hyperextension and modification of training (such as comprehensive warm-up strategies). Further studies are necessary in clarifying the pathophysiology to assist in optimising management strategies.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.