
ABSTRACT
A 26-year-old man was diagnosed with epilepsy a few months previously and admitted with status epilepticus. Computed tomography (CT) of the brain and CT venography were unremarkable. Magnetic resonance imaging (MRI) of the brain showed evidence of possible acute focal infarction in the splenium of the corpus callosum that showed a true restricted diffusion. The patient had no vascular risk factors and no focal neurological deficit on examination to explain the occurrence of an acute infarction. MRI of the brain was repeated 1 month later to assess for progression of that lesion and showed resolution of it. This case highlights the association of cytotoxic lesions of the corpus callosum that show true restricted diffusion with status epilepticus. It also emphasises the importance of medical reasoning and not being solely dependent on diagnostic investigations without reasonably linking them to the history and examination.
Introduction
The term cytotoxic lesions of the corpus callosum (CLOCCs) has been proposed recently as a more precise description of the phenomenon that has previously been known by many terms, including mild encephalopathy with reversible splenial lesions (MERS), reversible splenial lesion syndrome (RESLES), reversible/transient splenial lesions (TSL), clinically silent lesions in the splenium of the corpus callosum, transient focal lesions in the splenium of the corpus callosum and boomerang sign.1
Radiologists should be familiar with the imaging appearance of CLOCCs to avoid a misdiagnosis of ischaemia. When CLOCCs are found, the underlying cause of the lesion should be sought and addressed.1
Case presentation
A 26-year-old man was diagnosed with epilepsy a few months previously (focal onset epilepsy with unknown cause). His seizure types included focal to bilateral tonic-clonic seizures that began with a ringing sensation in his ears, hearing becoming muffled and subsequent impaired awareness. He also had brief episodes of an isolated ringing sensation in his ears that may have represented focal aware seizures, localising to cortical temporal lobes. Baseline magnetic resonance imaging (MRI) of the brain and electroencephalography (EEG) performed during diagnostic work-up had been normal. He was admitted with status epilepticus. He had no fever, headache, neck stiffness, history of recent infection, trauma, alcohol abuse, drugs abuse or any vascular risk factors. Neurologic examination revealed no focal neurological deficit.
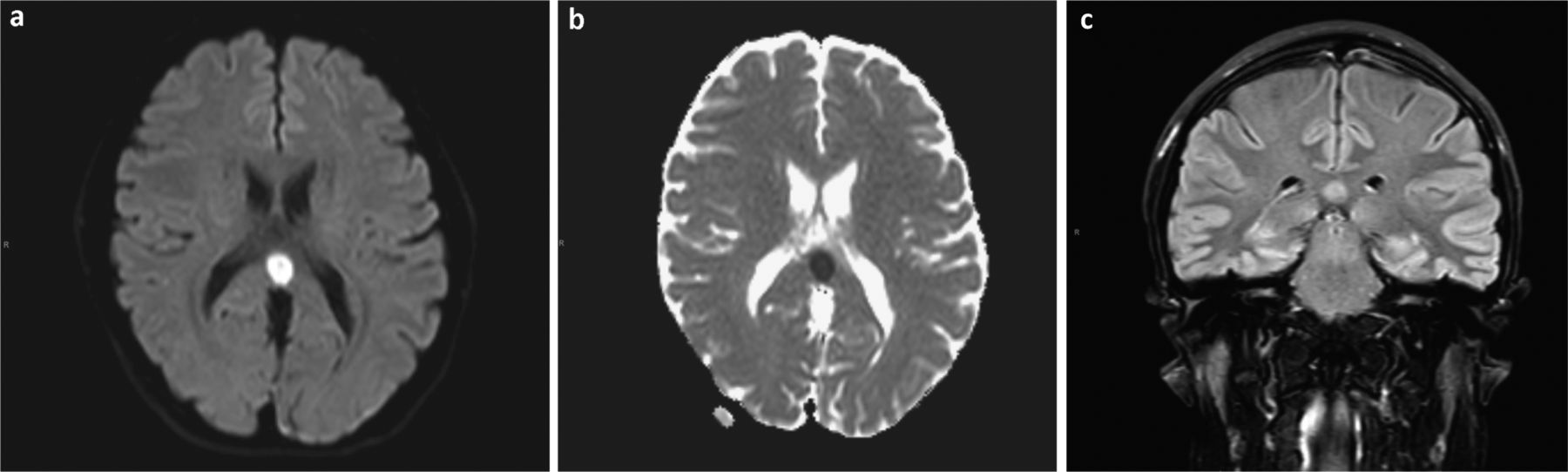
Full blood counts, blood sugar, electrolytes, kidney function test, liver function test, inflammatory markers and coagulation screen were all unremarkable (Table 1). Cerebrospinal fluid (CSF) analysis was unremarkable too (Table 2). EEG showed periods of widespread anterior dominant theta, at times sharpened, which could reflect predominantly frontal cortical dysfunction (such as due to postictal changes). Computed tomography (CT) of the brain and CT venography were unremarkable. MRI of the brain showed an isolated lesion in the splenium of the corpus callosum (CC) with restricted diffusion (Fig 1).
Blood test results
Cerebrospinal fluid test results
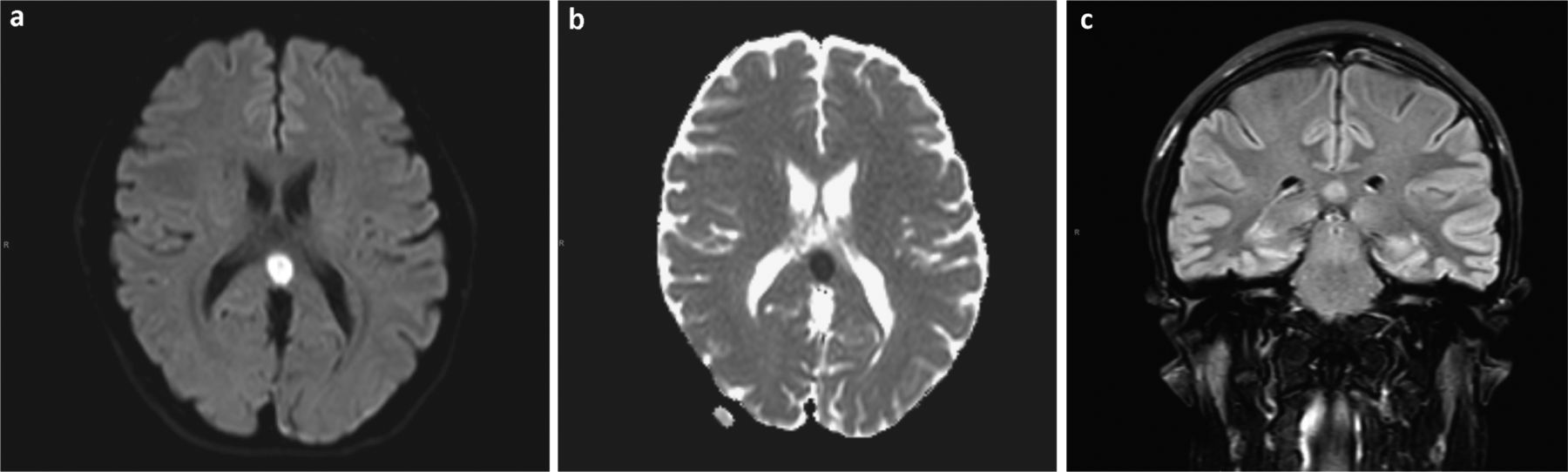
Magnetic resonance imaging of the brain on admission showing an isolated lesion in the splenium of the corpus callosum. a) Diffusion-weighted imaging showing high attenuation. b) Apparent diffusion coefficient map showing low attenuation. c) Fluid-attenuated inversion recovery imaging showing high attenuation.
Differential diagnosis in this scenario includes infection (encephalitis/meningitis), drugs (antiepileptic drugs), infarction, demyelination, metabolic conditions, epilepsy or status epilepticus. The patient had no vascular risk factors or focal neurological deficit to suggest infarction and nothing to suggest demyelination too. Investigations showed nothing to indicate metabolic issues. He had also no fever or anything to suggest infection (including normal CSF) and no history of trauma or any recent changes in medications. In light of the status epilepticus presentation and absence of other convincing diagnosis that can explain this lesion, CLOCCs associated with status epilepticus seemed to be the most reasonable diagnosis.
Before admission, the patient was on levetiracetam. On admission, he was treated successfully for status epilepticus. He was discharged on levetiracetam 1.5 g twice daily and clobazam 10 mg twice daily. A follow-up imaging to monitor the lesion progression after 1 month was planned.
MRI of the brain was done after a month of being discharged and showed a resolution of the lesion in the splenium of the CC (Fig 2). The patient has not had any further episodes of status epilepticus since then but he still has uncontrolled seizures. Sodium valproate and midazolam were added accordingly. The patient was still experiencing intermittent seizures while using the antiepileptic medications yet his imaging showed a resolution of the lesion, which gives us a more convincing evidence that the lesion is mainly due to status epilepticus rather than being medication induced.
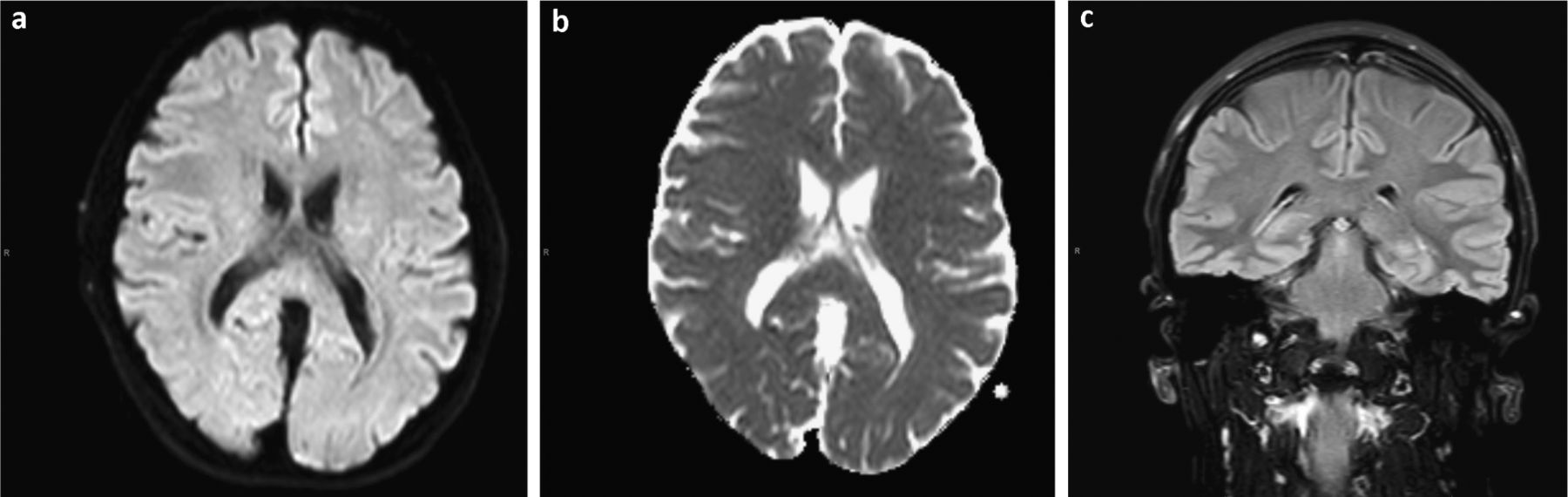
Magnetic resonance imaging of the brain after a month of being discharged and showing a resolution of the lesion in the splenium of the corpus callosum. a) Diffusion-weighted imaging. b) Apparent diffusion coefficient map. c) Fluid-attenuated inversion recovery imaging.
Discussion
The CC forms the bridge between the cerebral hemispheres, containing crossing axonal fibres from both hemispheres.2 Up to 1940, the neurological function of the CC was not understood. Callosotomy, used in the treatment of epilepsy, first reported in 1940, has allowed a better understanding of its function. It has led to the view that the CC is involved in transferring information between the cerebral hemispheres.3
CLOCCs is an imaging finding that usually resolves within the first month of the neurological symptoms, and develops from a variety of medical conditions including viral infections, epileptic seizures, metabolic disorders, drug toxicity, malignancies, status migrainosus, cerebrovascular disease and other conditions.4
The involvement of the CC typically shows one of three patterns: a small round or oval lesion located in the centre of the splenium, a lesion centred in the splenium but extending through the callosal fibres laterally into the adjacent white matter or a lesion centred posteriorly but extending into the anterior portion of the CC.1
With trauma, infection and inflammation, macrophages become active and release inflammatory cytokines. The net result of this cytokinopathy is massively increased amounts of glutamate in the extracellular space at levels 100 times the normal level or more.1
There is a strong association between the CC and seizures. Seizures are observed in up to two-thirds of people with developmental CC anomalies.5 Transient lesions of the CC were first reported by Kim et al in 1999 who noted the disappearance of focal lesions in the splenium of the CC of two patients after withdrawing antiepileptic drugs (AEDs).6
In cases of epilepsy, there are two possible mechanisms for the development of such lesions: the lesion can occur due to transient oedema resulting from the effect on the fluid-balance system by arginine vasopressin (AVP) levels; and a few AEDs can influence the fluid-balance system and cause oedema; also, AEDs can interact with AVP, causing such a brain oedema.7
Theories like anatomical uniqueness of the splenium of the CC, development of cytotoxic oedema, cytokines release and the role of AVP levels have described the predilection of the splenium of the CC for development of such lesions. Without follow-up imaging, such lesions cannot be termed as CLOCCs.8
Infarctions can be one of the causes of such lesions, but infarctions restricted to the CC are rare because of its rich blood supply from the different arteries bilaterally. Furthermore, the perpendicular orientation of the callosal branches may prevent embolisation.9 Another possible reason is that CC is a dense white matter tract that is slightly less sensitive to hypoxia or transient ischaemia than grey matter.10
Conclusion
This case emphasises the importance of medical reasoning and reasonably interpreting investigations and imaging according to the clinical scenario. It also encourages the concept of interval imaging, highlighting the importance of follow-up imaging in specific clinical scenarios. An awareness among physicians about approaching such lesions is paramount to avoid rushing into a diagnosis of stroke that can, consequently, lead to unnecessary investigations and treatment.
Key points
CLOCCs can develop in different medical conditions including infections, seizures, metabolic disorders, drug toxicity, malignancies, headache, cerebrovascular disease and other conditions.
CLOCCs is an imaging finding that usually resolves with time (mostly reversible).
Imaging should be interpreted in the context of the clinical scenario.
Follow-up imaging is needed to confirm the diagnosis.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.