
Editor – In our 2014 article, we demonstrated that end-tidal carbon dioxide (ETCO2; the level of carbon dioxide that is released at the end of an exhaled breath) is a reliable screening test to rule out pulmonary embolism.1 There were a small number of patients (n=100), with only 38 patients with pulmonary emboli (PEs). We demonstrated then that an ETCO2 of <4.3 kPa (32.3 mmHg) had a sensitivity of 100%, specificity of 65% and negative predictive value (NPV) of 100%.1
In view of the small number, we elected to extend the study to 200 cases and repeat the analysis on 70 patients who had PEs on computed tomography (CT; Fig 1).
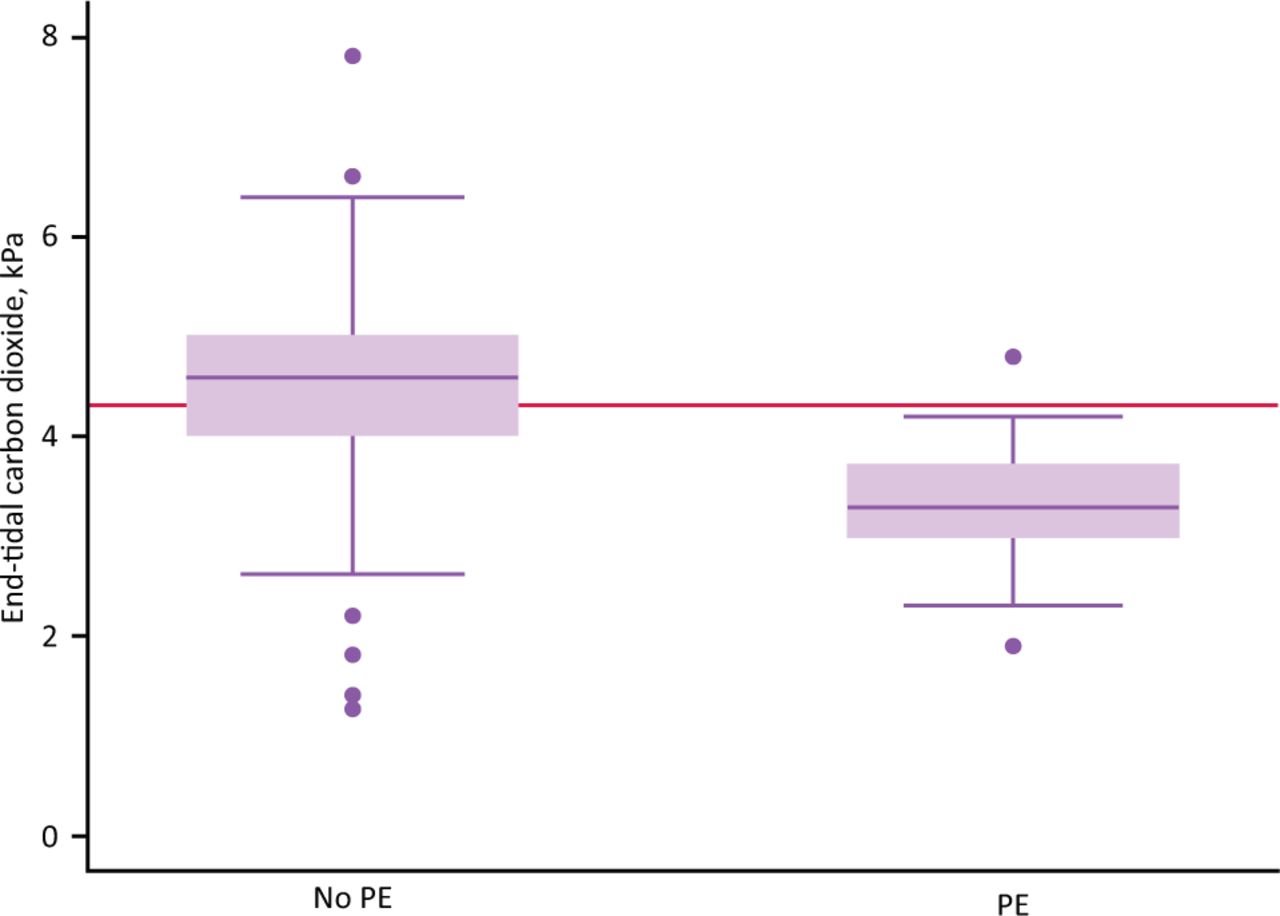
Computed tomography pulmonary angiography (CTPA) positive and CTPA negative results for end-tidal carbon dioxide (ETCO2). The red line represents threshold of 4.3 kPa (32.3 mmHg). This figure shows that no patient with a ETCO2 of >4.3 kPa had a pulmonary embolism. PE = pulmonary embolism.
Our updated results show similar statistics with an excellent NPV in ruling out PEs (Table 1). Our institution administers over 1,000 CT pulmonary angiographies (CTPAs) per year, reducing these can have a huge financial saving locally and to the NHS at large, as well as reducing the number of complications from procedures due to allergies or kidney problems relating to the dye used for CTPAs. ETCO2 can be applied in the emergency rooms and medical assessment wards. This helps with the flow of cases as well without the need for venipuncture.
End-tidal carbon dioxide classification table over a range of cut-off thresholds
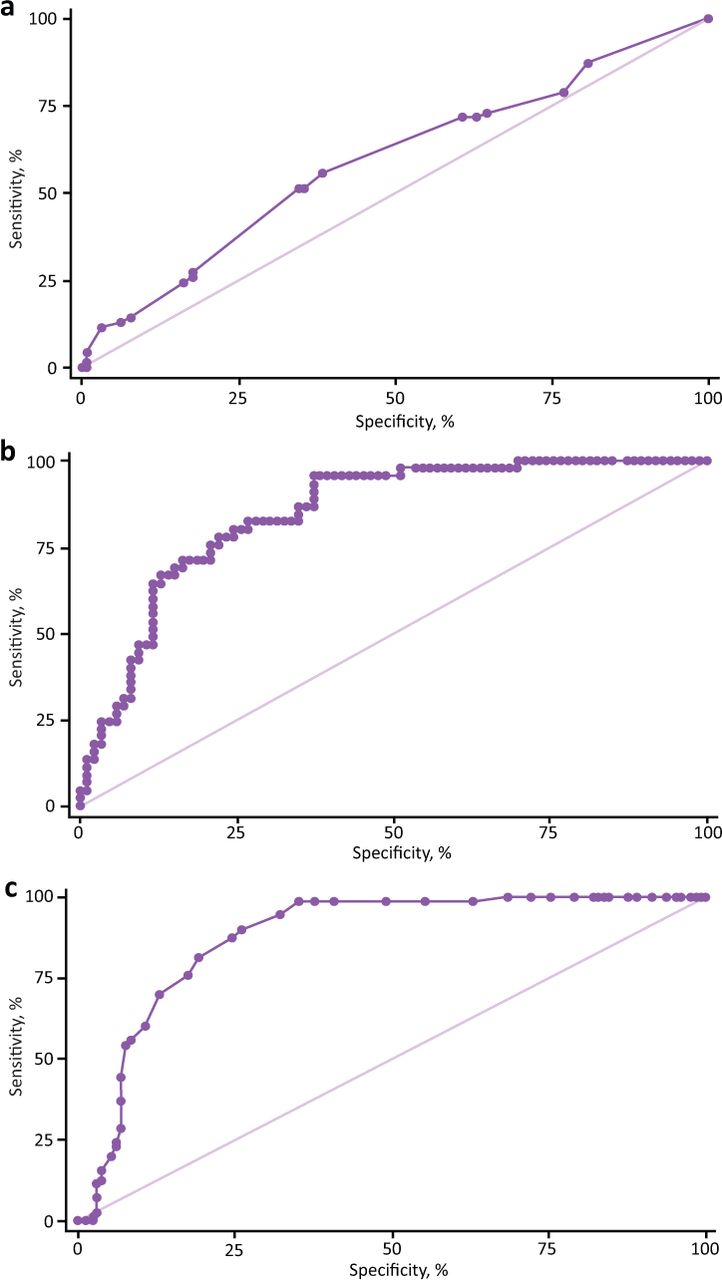
This is the only study to compare ETCO2 with D-dimer; D-dimer is the gold standard to rule out PE at present (Fig 2).

Area under receiver operator characteristic curves (AUROCCs) for the true positive rate against the false positive rate for different possible cut-off points. a) Wells score, AUROCC = 0.5891. b) D-dimer, AUROCC = 0.8468. c) End-tidal carbon dioxide, AUROCC = 0.8768.
Both parameters look at similar tests but from different perspectives. D-dimer measures the clot lysis (fibrinolysis) and ETCO2 looks at the physiological consequences of the clot, ie dead space ventilation caused by the clot in the pulmonary circulation.
We will probably require a larger sample size for more definitive conclusions, but this is a promising step in the right direction.
- © Royal College of Physicians 2022. All rights reserved.
Reference








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.