
Abstract
Elderly trauma victims whose care is shared between surgeons and physicians have improved clinical outcomes and shorter hospital lengths of stay (LOS). To test whether a similar benefit can be gained for patients suffering traumatic brain injury (TBI), a quality improvement project (QIP) was run in which a neurologist was enrolled into the pre-existing neurotrauma team. Mortality rates, LOS and rates of readmission within 30 days of discharge were compared between two cohorts of TBI patients: 80 admittedly prior to the QIP and 80 admitted during the QIP. The two cohorts were well matched for age, gender, mechanism of injury, Glasgow coma score and types of injury. The QIP was not associated with a reduction in mortality but was associated with a significant reduction in mean LOS (from 25.7 days to 17.5 days; p=0.04) and a reduction in readmissions (from seven to zero patients; p=0.01).
Introduction
In the UK, adult victims of moderate and severe traumatic brain injury (TBI) are cared for through regional trauma networks, primarily under the instruction of neurosurgical departments.1 However, it is estimated that fewer than one-third of patients with TBI require a neurosurgical procedure, suggesting care could be provided by, or shared with, other specialties.2 As well as decreasing the demand on neurosurgical services, this may improve care; for example, shared care between surgeons and physicians has reduced the mortality and length of stay (LOS) of elderly patients suffering hip fractures.3,4 To explore the potential benefits of physician-shared care for TBI, our hospital employed a neurologist to join the neurosurgical team caring for patients admitted following a head injury, as part of a quality improvement project (QIP). Two cohorts of TBI patients were identified and compared: one before and one during the intervention. Primary outcome measures included death, LOS and readmission within 30 days of discharge. Secondary outcome measures included the number of patients that were followed up in the outpatient setting, time to follow-up and the number of additional diagnoses identified at follow-up.
Methods
The intervention consisted of a neurologist with an interest in TBI working alongside the pre-existing neurotrauma team, composed of neurosurgeons, a specialist nurse, therapists and a rehabilitation coordinator. The neurologist saw inpatients at least once a week, joined the neurotrauma multidisciplinary team (MDT) meeting (which oversees inpatient care and directs hospital discharges) and ran a dedicated TBI clinic to follow up discharged patients.
Patients were identified from the trauma audit and research network dataset held by the John Radcliffe Hospital, Oxford, UK. The records of 80 TBI patients consecutively admitted to the department of neurosurgery were interrogated both before (July 2019 to December 2019) and after (July 2021 to December 2021) the intervention. The intervening time was used to plan and initiate the QIP, the start of which was paused while staff and resources were redeployed as part of the hospital's COVID-19 care strategy.
The anonymised demographic data collected were age, gender and mechanism of injury (MOI). Markers of injury severity (including the Glasgow coma score (GCS) at admission), and the presence or absence of cerebral contusion, extra-axial haematoma, subarachnoid haemorrhage, skull fracture, diffuse axonal injury, seizures and/or polytrauma were also recorded. These markers were chosen based on established models of assessing TBI and overall trauma severity.5 The frequency of the following neurosurgical interventions was also recorded as a means of comparing TBI severity between the two cohorts: the insertion of either an intracranial pressure monitor (ICPm) or an extra-ventricular drain (EVD), or the requirement for craniotomy or craniectomy.
The primary outcome measures included death from all causes, total LOS (subdivided into intensive treatment unit (ITU) LOS and ward LOS) and the number of patients readmitted within 30 days of discharge.
As secondary outcome measures, we recorded if a post-traumatic amnesia (PTA) assessment was carried out. Testing for PTA allows clinicians to identify when a patient is fully oriented and can form continuous memories. Length of PTA is an important predictor of long-term recovery, especially in behavioural and memory domains, and its early identification can help patients access appropriate neurorehabilitation services.6 We also recorded if at least one family meeting was documented, the proportion of patients who were followed up in a dedicated TBI clinic, the time to follow-up, and the number of additional diagnoses identified and treated at follow-up.
To compare the cohorts, Student's t-test was used for all parametric data from the two groups (eg age), Wilcoxon rank-sum test for two-sample non-parametric data (eg LOS) and Fisher's exact test for categorical variables (eg the presence or absence of contusions). Values were considered significant where p<0.05.
We hypothesised that the addition of a neurologist with an interest in TBI to the neurotrauma team would lead to a significant improvement in those outcomes listed.
Results
Baseline features
The groups were well matched, with no significant demographic difference or injury severity (Table 1).
Demographics and injury severity markers
Interventions
The two groups underwent a similar number of neurosurgical procedures; for example, in the pre-intervention group, nine people underwent insertion of an ICPm or EVD without recourse to more invasive surgery, compared with seven in the post-intervention group (p=0.59). Similarly, 23 people in the pre-intervention group underwent a craniotomy or craniectomy compared with 22 in the post-intervention group (p>0.99).
Outcomes
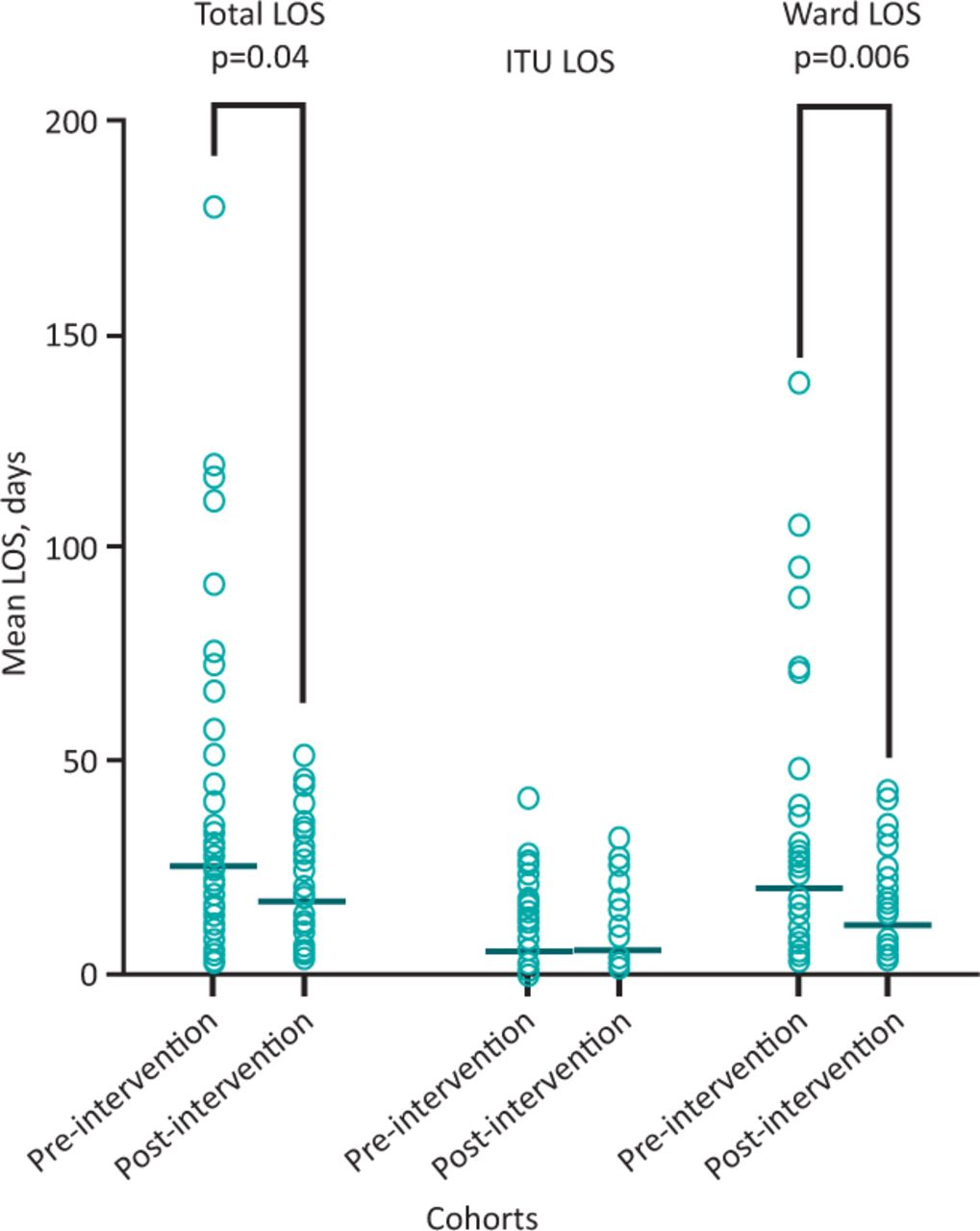
The introduction of a neurologist to the neurotrauma team was associated with a significant reduction in the mean total LOS (mean total LOS was 25.7 days versus 17.5 days (p=0.04) and median total LOS was 13.5 days versus 14.0 days). A significant reduction was seen in mean and median ward LOS (mean ward LOS was 20.1 days versus 11.8 days (p=0.006); and median ward LOS was 12.0 days versus 8.5 days) but not in ITU LOS (Fig 1).
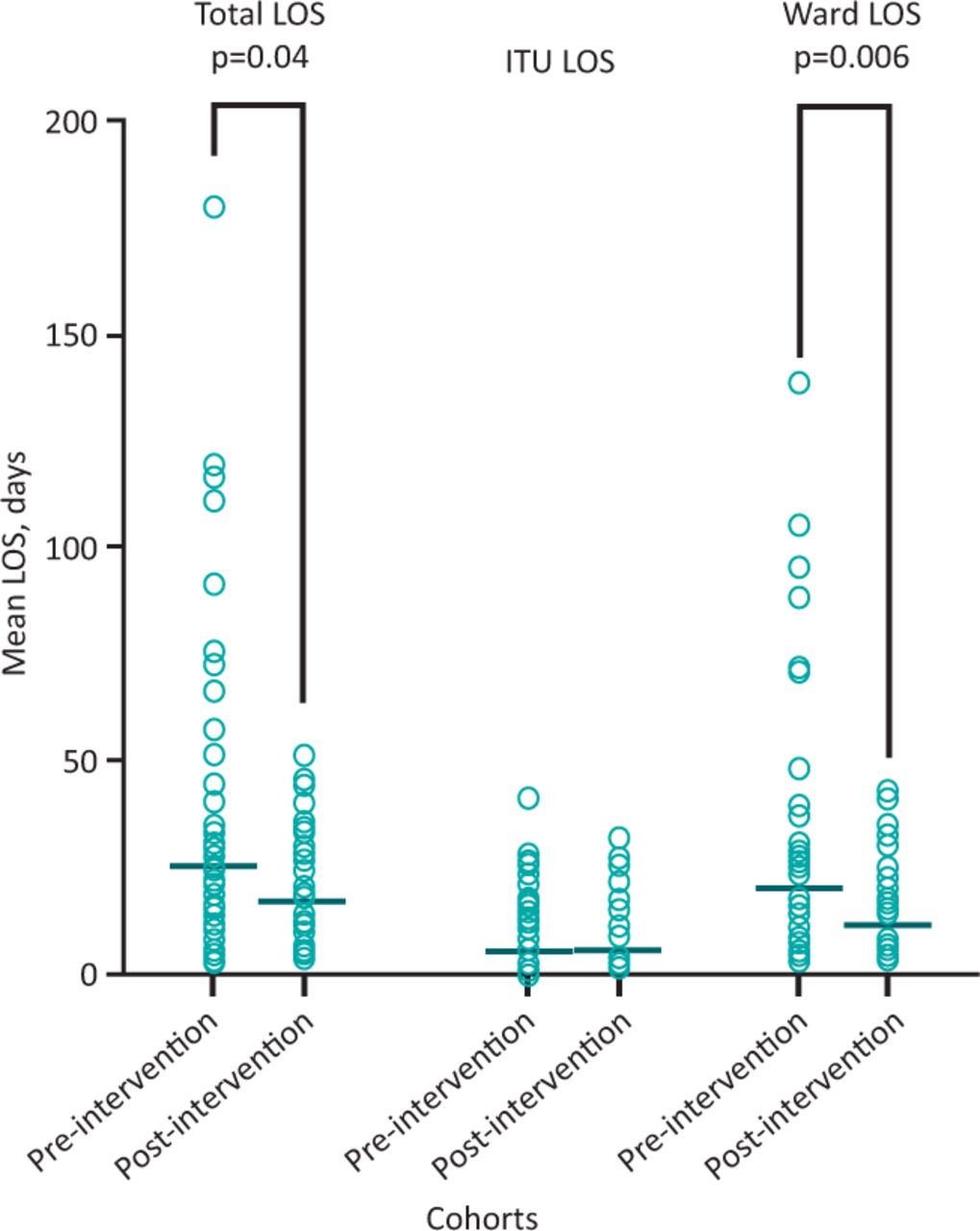
Mean length of stay pre- and post-intervention. ITU = intensive treatment unit; LOS = length of stay.
There was a significant reduction in the number of cases requiring readmission within 30 days of discharge (number of patients readmitted before and after the intervention were seven versus zero, respectively; p=0.01) but no reduction was seen in the number of deaths (number of deaths before and after the intervention was three versus three, respectively; p>0.99).
Prior to the intervention, 30% of TBI patients were followed up in clinic compared with 90% after the intervention (p<0.0001). There was no difference in the time from discharge to follow-up: 3.0 months in the pre-intervention group versus 2.9 months in the post-intervention group (p=0.64). However, significantly more patients followed up in the post-intervention group were found to have additional diagnoses (51% versus 7%; p<0.0001). A list of additional diagnoses is provided in Table 2.
Additional diagnoses identified at follow-up
The number of cases in which family meetings took place differed significantly, with meetings occurring in 10% of pre-intervention cases and 46% of post-intervention cases (p<0.0001). Finally, PTA testing occurred more frequently following the intervention (percentage of patients undergoing PTA assessment pre- vs post-intervention was 19% vs 46%, respectively; p=0.04).
Discussion
In many countries, the care of elderly trauma patients is shared between surgeons and physicians as standard. Benefits include reduced inpatient mortality, decreased LOS and an increased likelihood of being discharged to home.7 Whether or not a similar benefit might accrue to patients with head injuries is unknown. Herein, we report that shared care between physicians and surgeons is associated with a reduction in LOS and hospital readmission for patients with a head injury. Broadening the neurotrauma team skill set also increased the number of patients offered outpatient follow-up, and led to increased identification and treatment of neurological conditions associated with TBI.
The addition of a neurologist to the care team appears to be most effective in reducing long admissions; for example, the reduction in mean ward LOS was 8.3 days while the reduction in median ward LOS was 3.5 days. The reduction may stem from the earlier identification and treatment of conditions (such as headache, seizures and post-traumatic amnesia) that otherwise delay safe discharge. Earlier engagement with neurorehabilitation centres is also likely to have reduced LOS, while the involvement and education of family members in patient care, which increased following our intervention, may have improved discharge planning and reduced readmission.8
Although the QIP was not set up to explore the health economics of TBI care, a reduction in median ward LOS of 3.5 days for approximately 200 TBI patients per year, with a predicted ward cost per bed day equal to £586.59, would amount to a cost saving of £410,613 per year for our NHS trust alone.9 This is a conservative estimate based on the 2016 cost of a general ward bed, whereas specialist neuroscience beds at 2022 values could be expected to make greater financial gains. Furthermore, the saving far outstrips the cost of the two programmed activities (PAs) required for a physician to provide this service. Taking the British Medical Association's calculated cost per PA as £422, the annual cost of adding a physician to the neurotrauma team equates to £43,888 (giving a predicted cost saving of £366,725 per year).10 Replicated across the NHS, this amounts to an enormous potential cost saving.
Future studies would do well to gather information on patient and family satisfaction with TBI services, as this will highlight areas for growth and continued good practice. Colleague feedback would also be useful, helping show the broader value of such services.
Our work also highlights the value to TBI patients of follow up with a neuroscience specialist. Head injury gives rise to a number of additional, common conditions (such as benign paroxysmal positional vertigo, headache and seizures) but also to less common or more difficult to manage conditions (such as superior semi-circular canal dehiscence, movement disorders and behaviour disturbance). Such problems are best identified and managed by those with routine clinical exposure to them. Future physician trainees could be skilled in this area, with fellowships designed to provide the required education and exposure.
Overall, our work lends support to the growing call for a broader skill set in teams caring for patients with TBI.11 This is especially relevant in the acute hospital setting, where LOS can be positively impacted by the early recognition and treatment of the neurological sequelae to head injury. A similar effect can be seen in the outpatient setting, where physician input leads to better recognition of secondary conditions triggered by trauma. Of note, our work focused solely on the care of TBI patients admitted under the care of neurosurgery: it is possible that a similar benefit might accrue in expanding this service to the care of TBI patients admitted under trauma or general medical teams.
The outbreak of the COVID-19 pandemic brought significant changes to inpatient services. As the QIP took place either side of the initial outbreak, our data must be interpreted with caution. However, we believe that our findings are robust and reflect a true improvement in TBI care, as we alone report a reduction in LOS while others saw both an increase in head injury severity and an increase in LOS during the pandemic.12,13 Furthermore, the QIP was paused during staff redeployment.
Conclusion
Our work demonstrates a significant reduction in total hospital LOS, an increase in the identification and management of TBI sequelae, and a reduction in early readmissions following the introduction of a neurologist to the neurotrauma team.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.