
ABSTRACT
We present a case of a cerebral and spinal infarction caused by paradoxical embolism following traveller's thrombosis in a patient with a low activity of protein S.
Case presentation
A previously fit 47-year-old man suffered from acute quadriplegia and epileptic seizures for 1 day. He was a truck driver with no history of hypertension, diabetes, atrial fibrillation, stroke, epilepsy or tumours. He took a long-distance bus trip before the onset of the neurological symptoms.
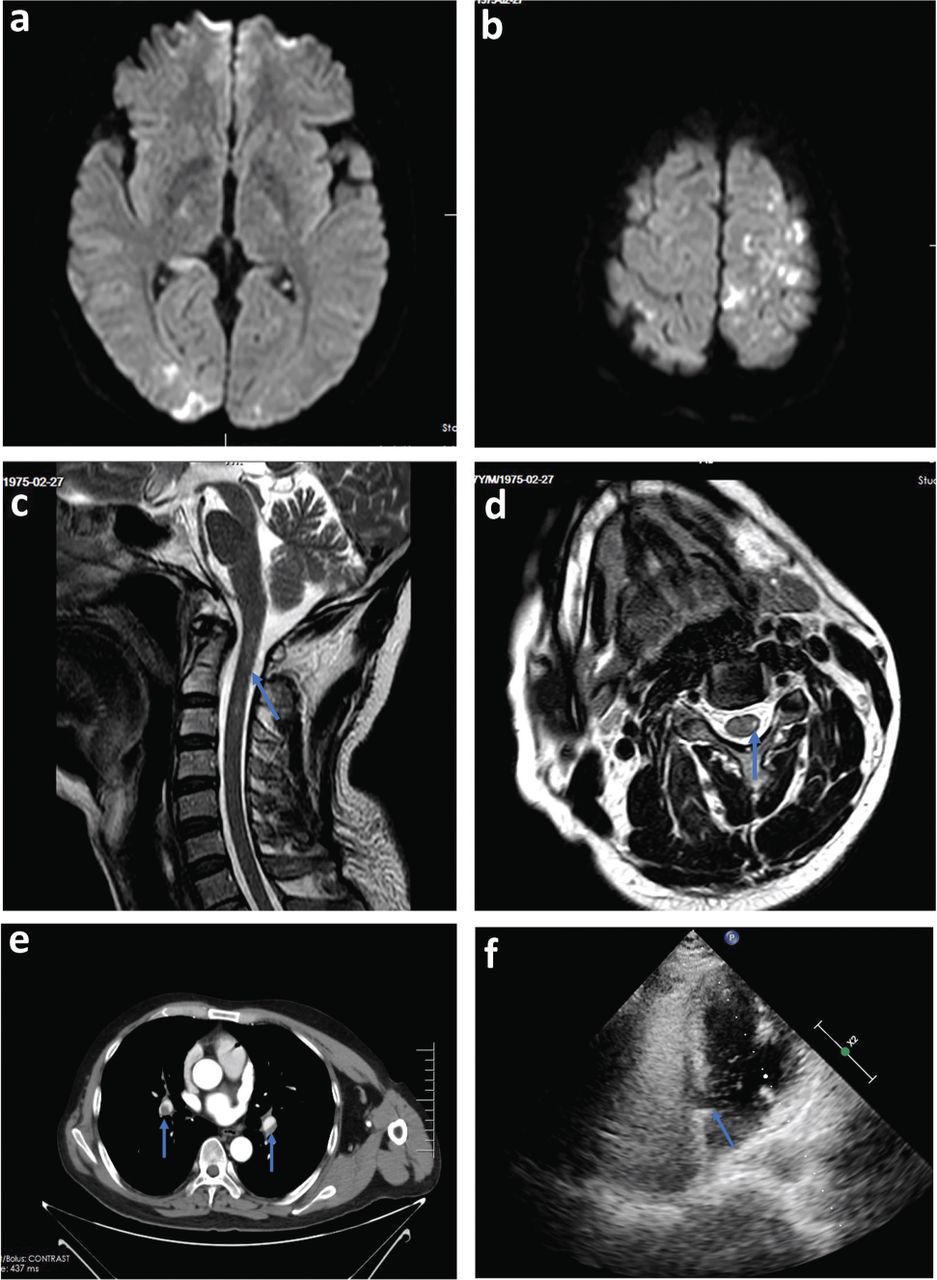
Clinical neurological examination performed at the emergency department detected left hemianopia, myasthenia of limbs (muscle strength was graded 0 or 1 for each limb), hypoalgesia below the C4 level and urine retention. Cranial magnetic resonance imaging (MRI) showed speckled diffusion weighted imaging (DWI) lesions in the cortex, including right cerebellar hemisphere, right occipital lobe and left parietal lobe without enhancement (Fig 1a and 1b). Spinal MRI showed a T2-hyperintense cervical cord lesion extending from C1 to C3 (Fig 1c and 1d). The auto-antibodies most commonly associated with autoimmune encephalitis (NMDAR, AMPA1, AMPA2, LGI1, CASPR2, GABABR, DPPX and GAD65) or central demyelinating diseases (MOG, AQP4, MBP and GFAP) were all negative in the cerebrospinal fluid and serum. Ultrasounds showed thrombosis of the left peroneal vein, while computed tomography angiography (CTA) of the chest showed low density shadow of distal pulmonary arteries on both sides (Fig 1e). Right-to-left shunt bubbles (>30/frame) were found after Valsalva manoeuvre (Fig 1f), but no left atrial thrombus was found by echocardiography. Electrocardiography (ECG) showed a sinus rhythm with T wave inversion in V2–V5 derivations, but no abnormalities were reported by coronary CTA. High-sensitivity troponin T (hsTnT) and D2 dimer increased to 0.342 μg/L and 2.52 μg/L, respectively. The activity of protein S decreased to 53% (normal range 77–143).
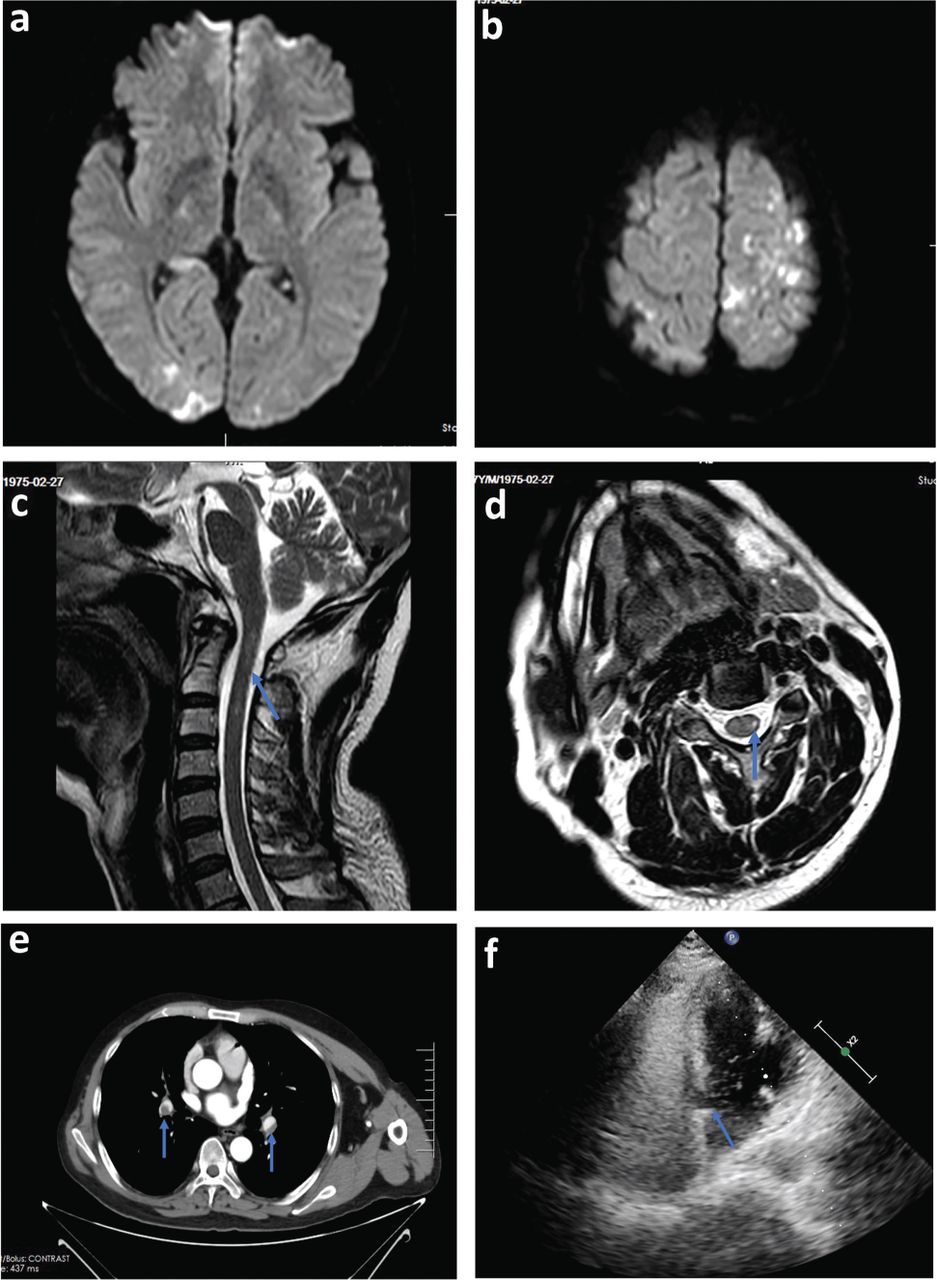
Patient imaging. a and b) Cranial magnetic resonance imaging diffusion-weighted imaging showing many speckled cortical lesions with the ‘dot sign’. c and d) T2-weighted cervical magnetic resonance imaging showing a spinal cord lesion extending from C1 to C3 with the ‘pencil sign’. e) Computed tomography of the chest showing distal pulmonary artery thrombosis on both sides. f) Echocardiography showing right-to-left shunt bubbles.
Discussion
We reported a case of a cerebral and spinal infarction caused by paradoxical embolism following traveller's thrombosis in a patient with a low activity of protein S. At present, few reports describing concomitant cerebral and spinal embolism infarctions have been published. The diagnosis of cerebral and spinal embolic infarction was corroborated by the sudden onset of acute symptoms (quadriplegia and seizures), physical signs and MRI manifestations (‘dot sign’ in the cerebral cortex and ‘pencil sign’ in spinal cord).1,2 The patient was characterised by the patent foramen ovale (PFO) and suffered from traveller's thrombosis, which caused a paradoxical embolism of cerebral and spinal arteries. The T wave inversion on ECG, the significant increase of hsTnT and the absence of coronary stenosis further suggested the possibility of a paradoxical embolisation of the systemic circulation. No history of fever or vaccination before the onset of symptoms, lesions in the cerebral cortex rather than white matter, and the ‘pencil sign’ in the spinal cord were all helpful to exclude acute disseminated encephalomyelitis. Neuromyelitis optica spectrum disorders were excluded because the auto-antibodies were all negative. Autoimmune encephalitis was excluded because lesions were not located in the limbic system and the auto-antibodies involved in autoimmune encephalitis were all negative. No history of tumours and no signal-intensified lesions on cranial MRI were helpful to exclude metastatic tumours of the brain or the spinal cord. Acute altitude sickness was ruled out because there was no obvious brain oedema on cranial MRI and no pulmonary oedema on the CT of the chest.
Paradoxical embolism is one of the causes for embolic stroke of undetermined source in the young population.3 The risk of paradoxical embolism (RoPE) score (total score: 10 points) is used to evaluate paradoxical embolism risk in patients with a PFO.4 Thaler et al defined a stroke related to a PFO when the RoPE score >6.5 Our patient scored 8 points, suggesting the presence of a paradoxical embolic cerebral infarction caused by a PFO. Paradoxical embolisation of spinal arteries is rare and potentially associated with an anterior spinal artery syndrome (ASAS). On MRI, the main lesions were located in the ‘watershed’ or ‘marginal zone’ (C2–C3, T3–T5 and L1–L2 segments), which exhibited T1-weighted iso- or hypointense signals, and T2-weighted hyperintense ‘pencil signs’ and ‘owl signs’.
Traveller's thrombosis is a travel-related deep vein thrombosis that can occur as a result of prolonged immobility during long-distance travel.6 Thrombophilic patients have a higher risk of developing traveller's thrombosis due to an abnormal hypercoagulability caused by the deficiency of protein S, protein C or antithrombin III. In our case, the patient was a truck driver with a decreased activity of protein S. Although he had no serious dyspnoea or hypoxaemia after sitting for a long time, his imaging examination showed deep peroneal vein thrombosis with bilateral pulmonary artery thrombosis. Therefore, we considered the patient suffered from a traveller's thrombosis. Due to the presence of a PFO, he developed cerebral and spinal infarctions because of a paradoxical embolism.
After 25 days of anticoagulation therapy with enoxaparin, the patient reported no further seizure. The muscle strength of both upper limbs reached grade V, while the muscle strength of the right and left lower limb reached grade IV and grade III, respectively. The hypoalgesia dropped to the T6 level, and the visual field and urinary function returned to normal. The patient was advised to take oral anticoagulation and to perform PFO closure after 2 months.
We report this case of cerebral and spinal embolism event to remind clinicians to be alert to the possibility of paradoxical embolism in patients with traveller's thrombosis, and improve the aetiological diagnosis of diseases involving both the brain and spinal cord.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
Related Articles
Cited By...
- No citing articles found.