
ABSTRACT
A 61-year-old man with hypertension and psoriasis, which was treated with adalimumab, was admitted after a 1-month history of fever following a dental implantation. Computed tomography of the chest revealed a pseudoaneurysm in the aortic arch, and blood culture grew Salmonella enterica. A diagnosis of mycotic pseudoaneurysm of the aortic arch due to Salmonella was made, and he was treated with cefoperazone–sulbactam. During his hospital stay, he developed hoarseness followed by haemoptysis, and underwent thoracic endovascular aortic repair followed by emergency open surgical repair. However, he died 5 weeks after the surgery due to acute upper gastrointestinal bleeding, which was confirmed as an aortoesophageal fistula by oesophagogastroscopy.
Case presentation
A 61-year-old man with hypertension and psoriasis, which was treated with adalimumab, was admitted after a 1-month history of fever following dental implantation. He reported chills but no cough or chest pain. His temperature was 39.3°C, with elevated white blood cell count, neutrophil count and C-reactive protein concentration. Contrasted computed tomography of the chest showed a pseudoaneurysm in the aortic arch (Fig 1). A blood culture grew Salmonella enterica.

Contrasted computed tomography of the chest (coronal view) showing a pseudoaneurysm in the aortic arch at admission.
Diagnosis
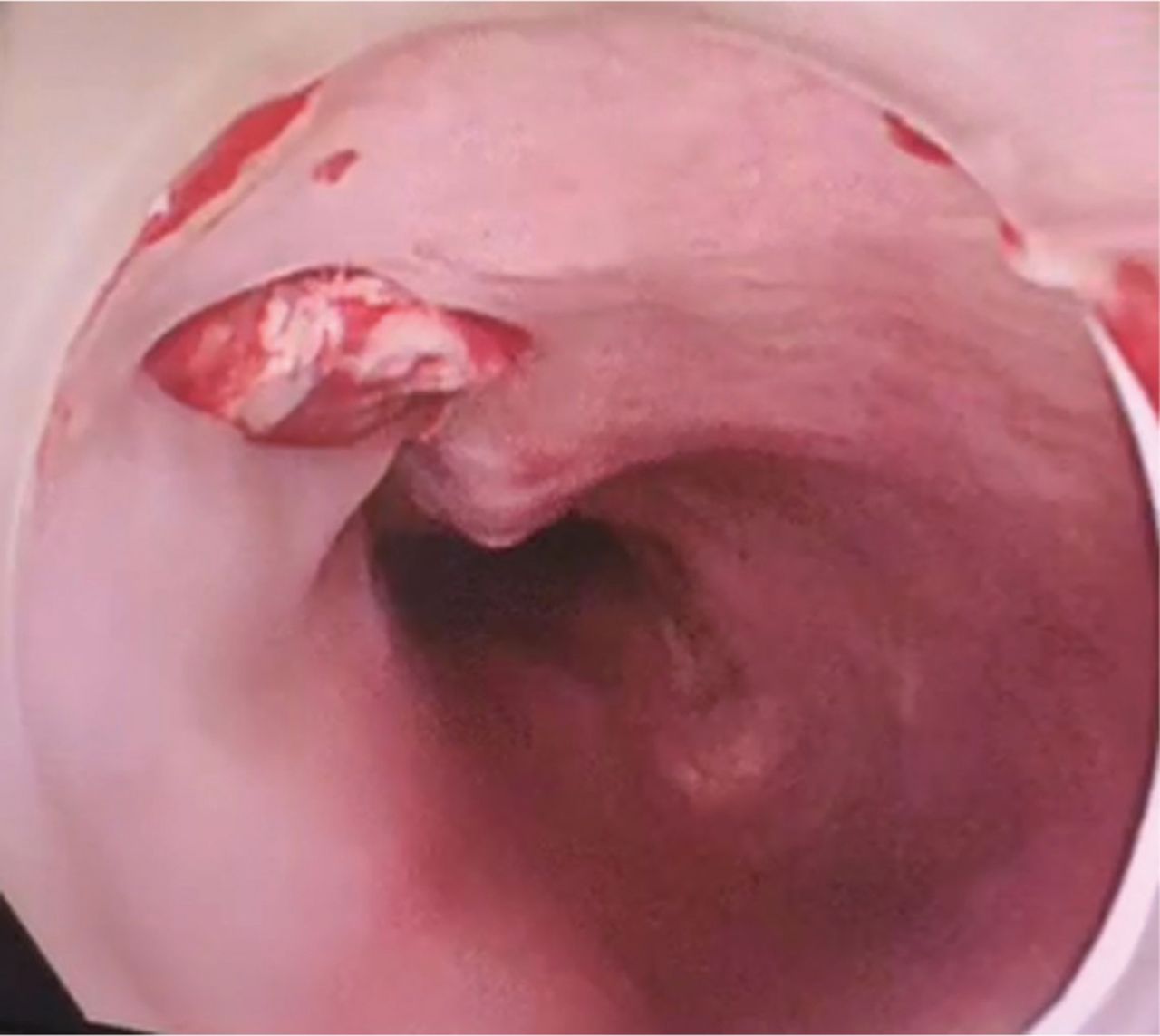
A diagnosis of mycotic aortic arch pseudoaneurysm due to Salmonella was made, and he was treated with cefoperazone–sulbactam. During his hospital stay, the patient developed hoarseness (known as Ortner's syndrome) when a progressively developed aortic arch pseudoaneurysm compresses the left recurrent laryngeal nerve between the left pulmonary artery and aorta, followed by haemoptysis.1 Because of uncontrolled infection, he underwent thoracic endovascular aortic repair (TEVAR) first. Unfortunately, the TEVAR failed in a week due to insufficient landing zone proximal to the aneurysm and he developed massive haemoptysis. An urgent open surgical repair was performed. Sadly, however, he died 5 weeks after the surgery due to acute upper gastrointestinal bleeding caused by an aortoesophageal fistula (Fig 2).
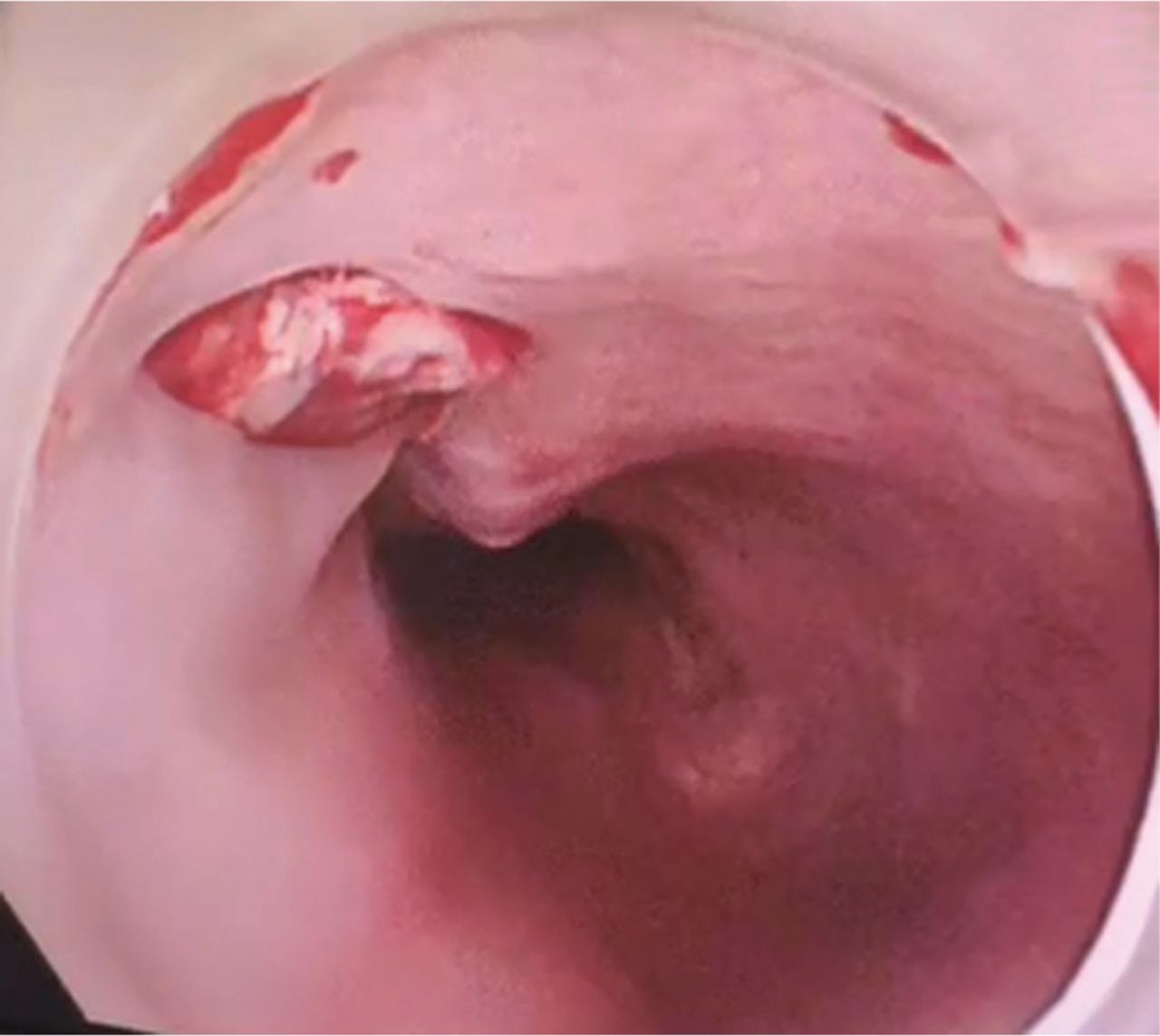
Oesophagogastroscopy revealing an aortoesophageal fistula 25 cm below the incisors.
Discussion
Mycotic aortic arch aneurysm is a rare but life-threatening pathology.2 The term ‘mycotic aneurysm’ was first used by William Osler in 1885 to describe a mushroom-shaped aneurysm in subacute bacterial endocarditis in which ulcerative endarteritis in the aortic arch produces multiple aneurysms.3 It is now known that mycotic aneurysms can arise from a wide variety of clinical causes. In our case, the risk factors of infection included the application of adalimumab, the aortic atherosclerotic lesions confirmed by the postoperative pathological examination and the damage to the oral mucosa during dental implantation. In addition to the left recurrent laryngeal nerve, the trachea is the most commonly affected structure by the aortic arch aneurysm. The treatment consists of antibiotics and surgery, either by TEVAR or open surgical repair.4,5 However, infection-related complications (sepsis, stent graft / graft infections, recurrent mycotic aortic aneurysms and aortoesophageal fistulas) pose a significant threat to patients even after surgery, as shown in our case. Resolution of infection is of key importance to improve the outcome.6
Funding
Funding support from the national key research and development programme of China (no 2021ZD0111000).
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.