
ABSTRACT
Cerebral amyloid angiopathy (CAA) is a common cause of lobar cerebral haemorrhage in elderly populations, which can present as transient focal neurological episodes (TFNEs) or sometimes known as ‘amyloid spells’. CAA-TFNE poses a common diagnostic challenge to physicians as it can be difficult to distinguish from transient ischaemic attacks or other transient neurologic syndromes. Prompt recognition of CAA is crucial as it heralds a high risk of intracerebral haemorrhage and to avoid unnecessary investigation with inappropriate long-term prevention treatment.
Introduction
Cerebral amyloid angiopathy (CAA) is a cerebral small vessel disease characterised by deposition of the amyloid-beta protein, affecting the cortex and leptomeninges.1 CAA typically presents with symptomatic intracerebral haemorrhage, cognitive impairment and episodes of recurrent stereotyped limb attacks.2 Herein, we report a case of an elderly patient with CAA presenting as transient focal neurological episodes (TFNEs) mimicking transient ischaemic attack (TIA) with a capsular warning sign.
Case presentation
A 75-year-old woman with underlying hypertension presented with periodic numbness starting in her left hand, spreading to left arm and face, lasting for 10 minutes that resolved spontaneously. She had similar paraesthesia from her back migrating to the left thigh and foot occasionally. She did not have any limb weakness, facial asymmetry or transient visual loss. She experienced such an episode 5 years previously and was diagnosed with right convexal subarachnoid haemorrhage (SAH) but was lost to follow-up. Subsequently, she had multiple visits to the emergency department over the years with TFNEs but was treated as recurrent TIA and discharged with antiplatelets. She also developed a recent onset of progressive short-term memory decline. On examination, she was alert and neurological findings were unremarkable. Computed tomography (CT) of the head showed convexal SAH in the right central sulcus (Fig 1a). CT angiography and venography revealed no aneurysm or thrombosis. Magnetic resonance imaging (MRI) of the brain showed superficial haemosiderin in bilateral superior frontal sulci, with minimum cortical microbleeds (Fig 1b). These findings are consistent with the modified Boston criteria for possible CAA (Box 1).3
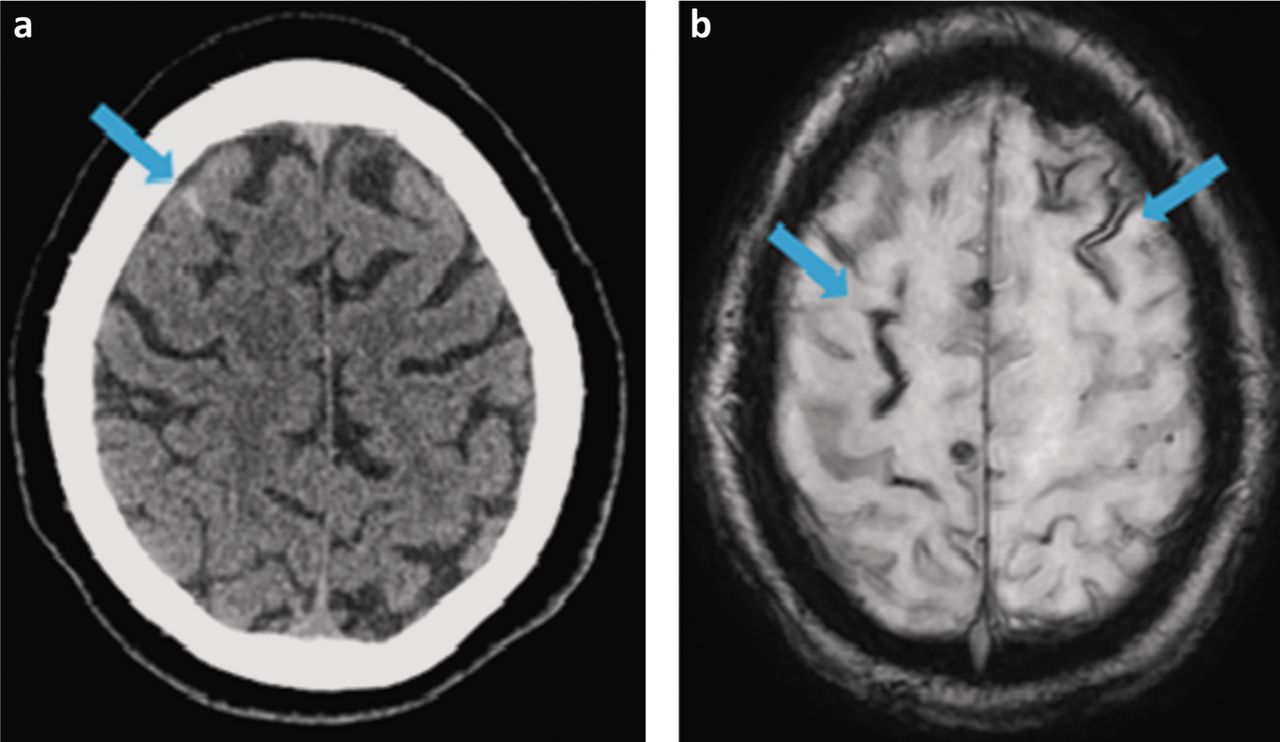
Brain imaging. a) Computed tomography showing the subtle hyperdensity within the sulcus in the right frontal lobe at the vertex. b) Magnetic resonance imaging susceptibility-weighted angiography showing superficial haemosiderin in bilateral superior frontal sulci.
Modified Boston criteria for possible cerebral amyloid angiopathy
Discussion
Among patients with acute non-traumatic convexal SAH, CAA was identified as the main cause in a quarter to a third of patients of all ages, including 76% of people aged 60 years or older.4 More than 75% of patients with convexal SAH presented with TFNEs, whereas TIA is often labelled as a mimic of ‘amyloid spells’ or CAA-TFNE.4,5 The cardinal features of CAA-TFNE are stereotyped, recurrent, transient neurological episodes of paraesthesia, and numbness or weakness of spreading onset over seconds to minutes with subsequent complete resolution caused by cortical spreading depression (CSD), as seen in our case, whereby the clinical features of such episodes correlated anatomically with superficial cortical siderosis in MRI of the brain. Cortical superficial siderosis (cSS) results in cortical spreading depolarisation that is secondary to irritative blood products trapped within the cerebral sulcus.4 The depolarisation of CSD propagates gradually across contiguous cortical regions, which explains the slow, smooth and somatotopic spread of neurological deficits that is pathognomonic for CSD.4 A systematic review highlighted that CAA patients with TFNE often had cSS or convexal SAH as compared with those without TFNE. TFNE predicts a substantial risk of lobar haemorrhage.5 Another recent meta-analysis confirms that cSS is a risk factor for future intracerebral haemorrhage (ICH), independent of the number of microbleeds, in patients with CAA with or without prior history of ICH.1 Hence, antiplatelets or antithrombotic drugs should generally be avoided.4
MRI of the brain is imperative to establish the diagnosis of CAA as it has high sensitivity for the characteristic haemorrhagic lesions that are not reliably seen on conventional scans.5 MRI of the brain should be performed to investigate suspected TIAs, especially in elderly patients with atypical symptoms.5 Currently, there are no proven interventions in CAA-TFNE to prevent future ICH, including ICH or convexal SAH.3 However, it is recommended to follow ICH guidelines among the high-risk patients for prevention, including for optimal blood pressure control of less than 130/80 mmHg.3
Conclusion
Identification of CAA, especially among the elderly patients as the underlying aetiology of transient neurological symptoms mimicking TIA is vital to avoid antiplatelets and anticoagulants, and to rationalise the right treatment and long-term plan.
Acknowledgements
We would like to thank the patient for allowing us to present her case.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.