
Introduction
Computed tomography pulmonary angiography (CTPA) has become a quick and readily accessible test. As a result, clinicians frequently come across incidental findings such as a rare case of pulmonary vein thrombosis (PVT) as presented here.
Case presentation
A 66-year-old man with known squamous-cell lung cancer presented with worsening breathlessness. He had been diagnosed in 2016, for which he underwent a right middle and lower lobectomy. In 2020, he had recurrence of lung cancer with CT showing an extensive right hilar mass invading the mediastinum. He received palliative radiotherapy and subsequently was started on immunotherapy. Two weeks after undergoing radiotherapy, he presented with worsening breathlessness and a cough productive of greenish sputum. His exercise tolerance had reduced from 100 yards to just a few steps. Apart from his oxygen saturation being 94% on room air, his physical examination was unremarkable. His blood tests showed raised inflammatory markers. He was started on oral doxycycline for a possible respiratory infection. A CTPA was performed that was negative for a pulmonary embolism but showed a PVT (Fig 1). Anticoagulation was initiated after reaching a shared decision.
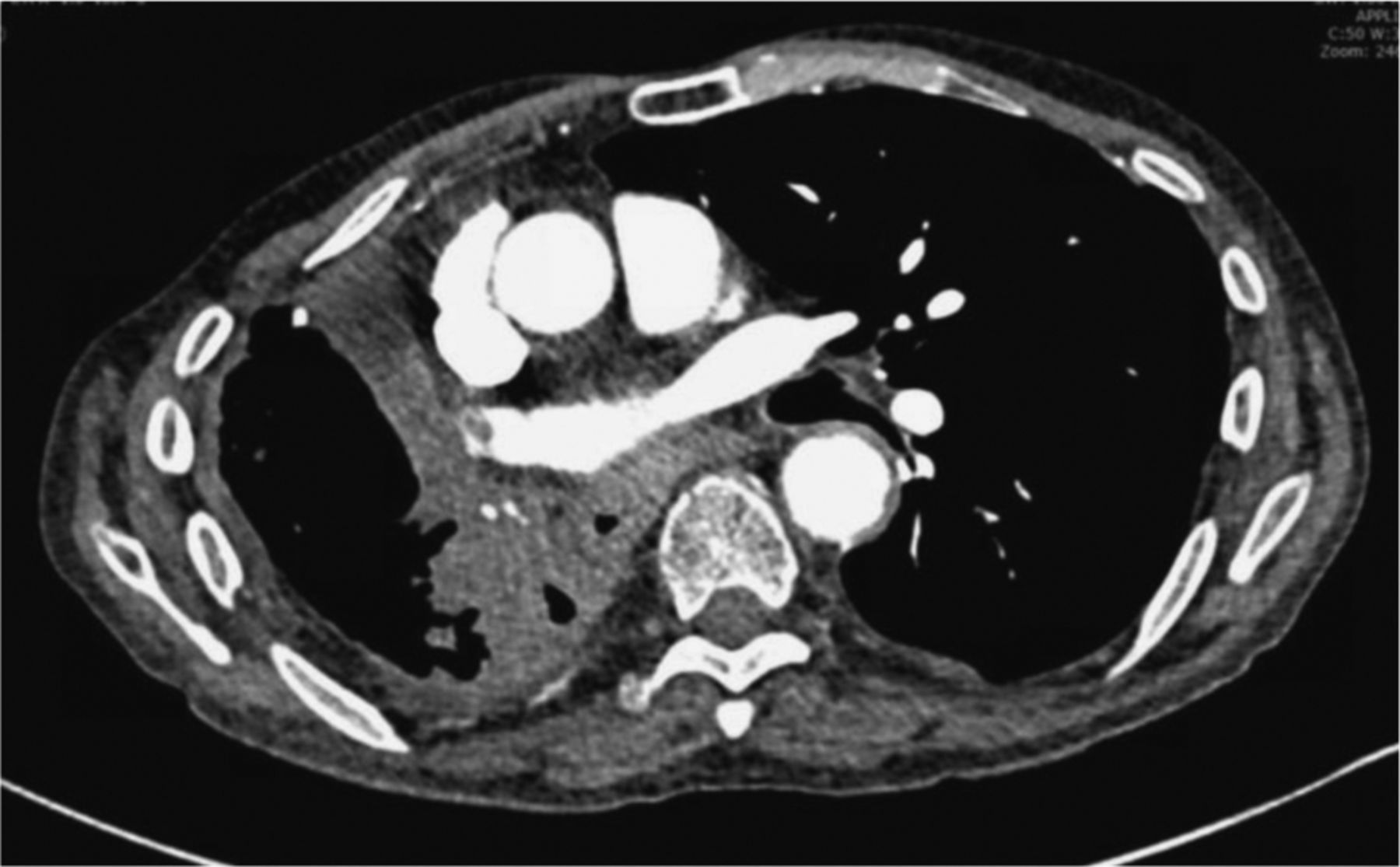
Computed tomography pulmonary angiography showing a thrombus in the right pulmonary vein, hilar soft tissue mass extending into the mediastinum.
Discussion
PVT can occur after surgical procedures involving manipulation of the pulmonary vessels, for example, lung transplant and lobectomy.1 Thrombosis in post-lung transplant patients can mimic acute graft dysfunction and incidence is as high as 15%.2 Rarely, radiofrequency ablation for atrial fibrillation can cause a clot. Non iatrogenic causes include malignancy, atrial fibrillation, left atrial thrombus, mediastinitis, sickle cell crises and trauma. Recently COVID-19 infection has also been associated with it.3 PVT can be completely asymptomatic and only picked up incidentally on imaging. However, if it is large enough to obstruct the pulmonary flow, it can lead to acute symptoms and even haemodynamic instability. Pulmonary oedema or an infarct can lead to symptoms like dyspnoea, haemoptysis or cough. Superadded bacterial infections can occur especially in the postoperative state. Long-term complications include heart failure and pulmonary fibrosis.4 Systemic embolisation to almost all major sites including the brain, kidneys and limbs have been reported.5,6 CTPA is the cornerstone investigation, which helps to diagnose the thrombus and also rules out certain aetiologies. Echocardiography is used to ascertain presence of left atrial thrombus and differentiate a true thrombus from tumour invasion. Treatment is to start anticoagulation in order to prevent embolism. Case reports in post-surgical patients have shown a role for antibiotics in that scenario. In acutely unstable patients with haemodynamic compromise and a large obstructive clot, thrombolysis can be considered. Another alternative in these circumstances, especially in post-surgical patients, would be thrombectomy, however, availability to this service is limited.7
Conclusion
PVT is an entity that we are likely to see more of due to an increase in frequency of radiological investigations. However, having an awareness of PVT as a cause of such complications may help to reduce the delay in diagnosis and treatment. It is essential that the risk of systemic embolisation be addressed with anticoagulation where appropriate.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.