
Introduction
Cardiac resynchronisation therapy (CRT) is recommended for suitable patients with heart failure (HF) who continue to be symptomatic despite optimal medical therapy (OMT).1 In reality, only a minority of patients are able to tolerate target dosages of guideline-directed medical therapy (GDMT) prior to receiving CRT.2 Common reasons for the same include low blood pressure, bradycardia, pauses, kidney injury or a combination of these factors.2 The aim was to assess whether a review by the heart failure team (HFT) post-CRT resulted in further optimisation of medical therapy for HF. The effect of this intervention on hospitalisation for HF, incidence of ventricular arrhythmias and mortality was also assessed.
Materials and methods
Retrospective analysis of records of consecutive patients undergoing CRT implantation (n=83; CRT defibrillator 70/83 (84.3%); CRT pacemaker 13/83 (15.7%)) between March 2017 and February 2019. Follow-up duration was 12 months. Baseline medical therapy prior to CRT was assessed. Patients reviewed by the HFT within six months of receiving CRT were compared with those who were not. Optimisation was defined as upward adjustment of dosages of GDMT or introduction of a new disease-modifying drug that the patient was not initially suitable for pre-CRT.
Results and discussion
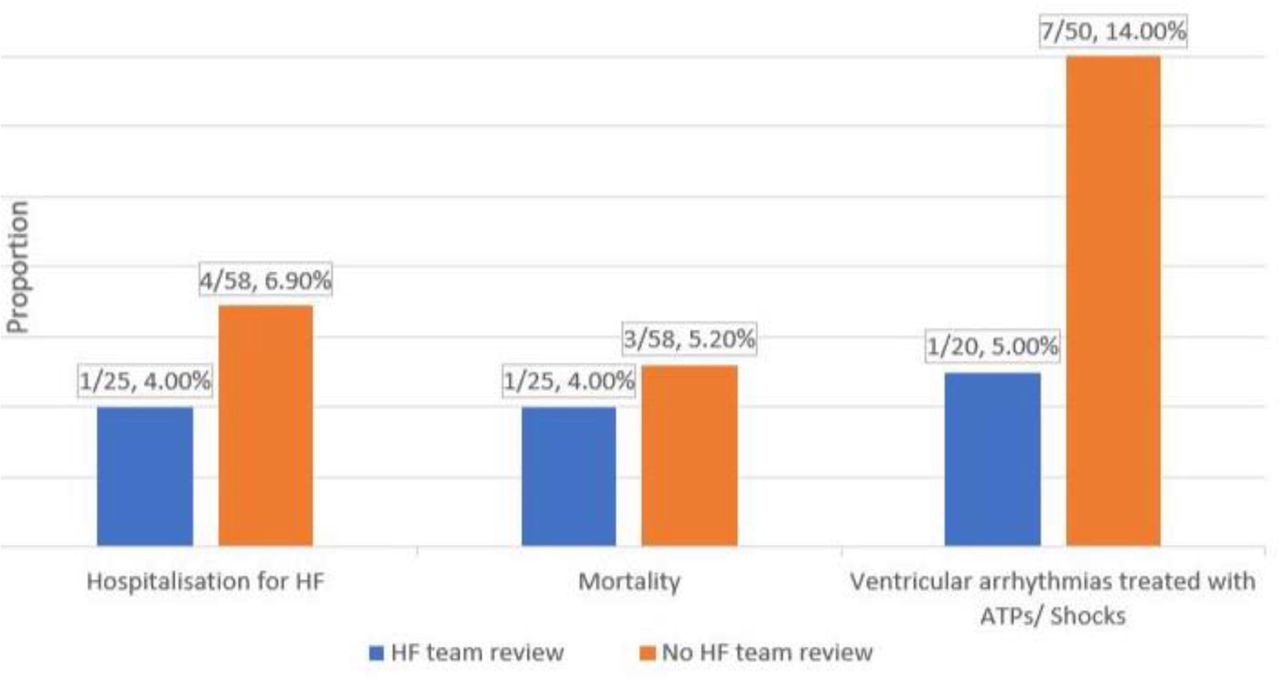
Mean age was 71.1±11.1 years and there were 58/83 (70%) men. Prior to CRT, the proportion of those on target dosages of angiotensin inhibitors, betablockers, mineralocorticoid receptor antagonist and sacubitril–valsartan was 27.7% (23/83), 24.0% (20/83), 8.4% (7/83) and 6.0% (5/83), respectively. Twenty-five (72%) patients reviewed by the HFT post-CRT had their medications optimised. Of the remainder (58/83; 69.9%), only 5.2% had their medications optimised. Beta-blockers were the most optimised medication. The proportion of patients experiencing ventricular arrhythmias (VTs) treated by the device, hospitalisation for HF and mortality was higher among those not reviewed by the HFT (Fig 1).
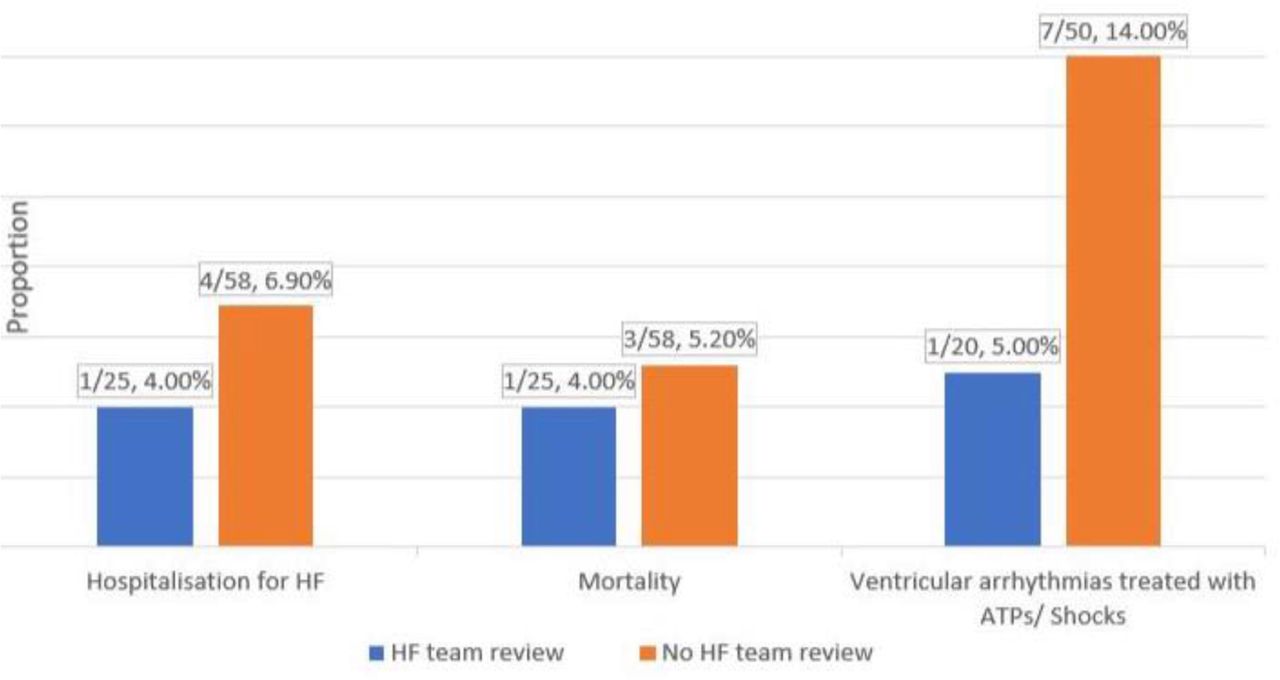
The 12-month outcomes for those reviewed and not reviewed by the heart failure team. ATP = anti-tachycardia pacing; GDMT = guideline-directed medical therapy; HF = heart failure.
The low proportion of patients on target dosages of GDMT is a reflection of the difficulty attaining the optimal recommended dosages prior to CRT.3 Our findings show that, in a vast majority of patients, there is room for optimisation of GDMT post-CRT. This may be because of an improvement in blood pressure following CRT as found in the COMPANION and CARE-HF trials.4,5 It may also be from protection against bradycardia, sinoatrial nodal pauses and slowing of atrio-ventricular conduction offered by CRT.2 The difference in VTs between the two study groups may have resulted from the higher proportion of beta blocker optimisation among those reviewed by the HFT. Background severity of HF, response to CRT, short duration of follow-up and other comorbid conditions may have contributed to the attenuation of differences in other clinical outcomes observed between the study groups.
Conclusion
We strongly recommend that all patients receiving CRT should have their medications optimised post-implant. In view of their expertise, this is best done by the HFT as attaining target dosages of GDMT remains a cornerstone of heart failure treatment, favourably influencing symptoms as well as possible prognosis.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.