
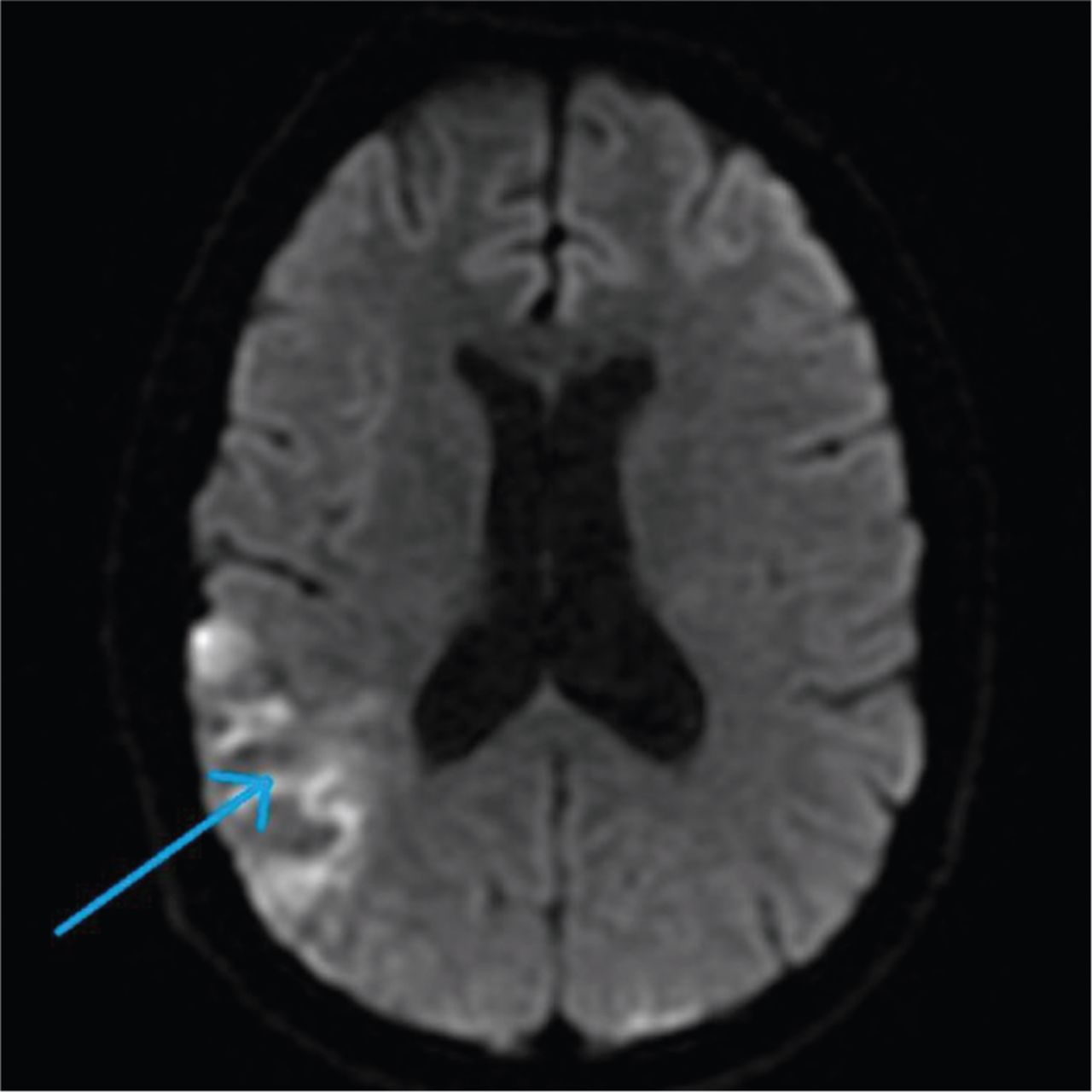
A middle-aged previously healthy and fit man presented with left sided weakness, slurred speech, left sided sensory neglect, mild headache and fever. He denied having any cough, shortness of breath, chest pain, palpitations, abdominal pain or bowel-bladder symptoms. He has smoked 5–10 cigarettes per day since adolescence and drank 1–2 cans of beer occasionally. He denied use of illicit drugs. He had two doses of COVID-19 vaccine and never had COVID-19. Repeated COVID-19 PCR swab was negative throughout the hospital stay. At admission, on systemic examination he only had left-side hemiparesis with mild left-side sensory neglect and upper motor neuron type of facial nerve palsy with no signs of meningism. Glasgow coma score was 14/15. Cardiovascular, respiratory and abdominal examinations were unremarkable. Vital signs were stable except for a mild rise of temperature of 37.8°C. Computed tomography of the head showed acute right-sided temporal ischaemic changes. He was not thrombolysed as the onset of symptoms was more than 4.5 hours. Blood tests showed high infection markers with C-reactive protein of 202 mg/L, normal haemoglobin, clotting screen and kidney function. Blood and urine cultures were negative. Electrocardiography showed sinus tachycardia and chest X-ray was unremarkable. Echocardiography showed low normal ejection fraction with mild mitral regurgitation. Transoesophageal echocardiography arranged on theatre that was documented as mitral valve vegetation. He was started on broad spectrum intravenous antibiotics for suspected infective endocarditis. He also complained of left leg pain for two months. Left leg ultrasound Doppler on this admission showed a large left leg deep vein thrombosis involving the femoral vein. Magnetic resonance imaging (MRI) of the head and magnetic resonance angiography of the carotids showed multiple cerebral and cerebellar infarcts with normal carotid arteries (Fig 1).
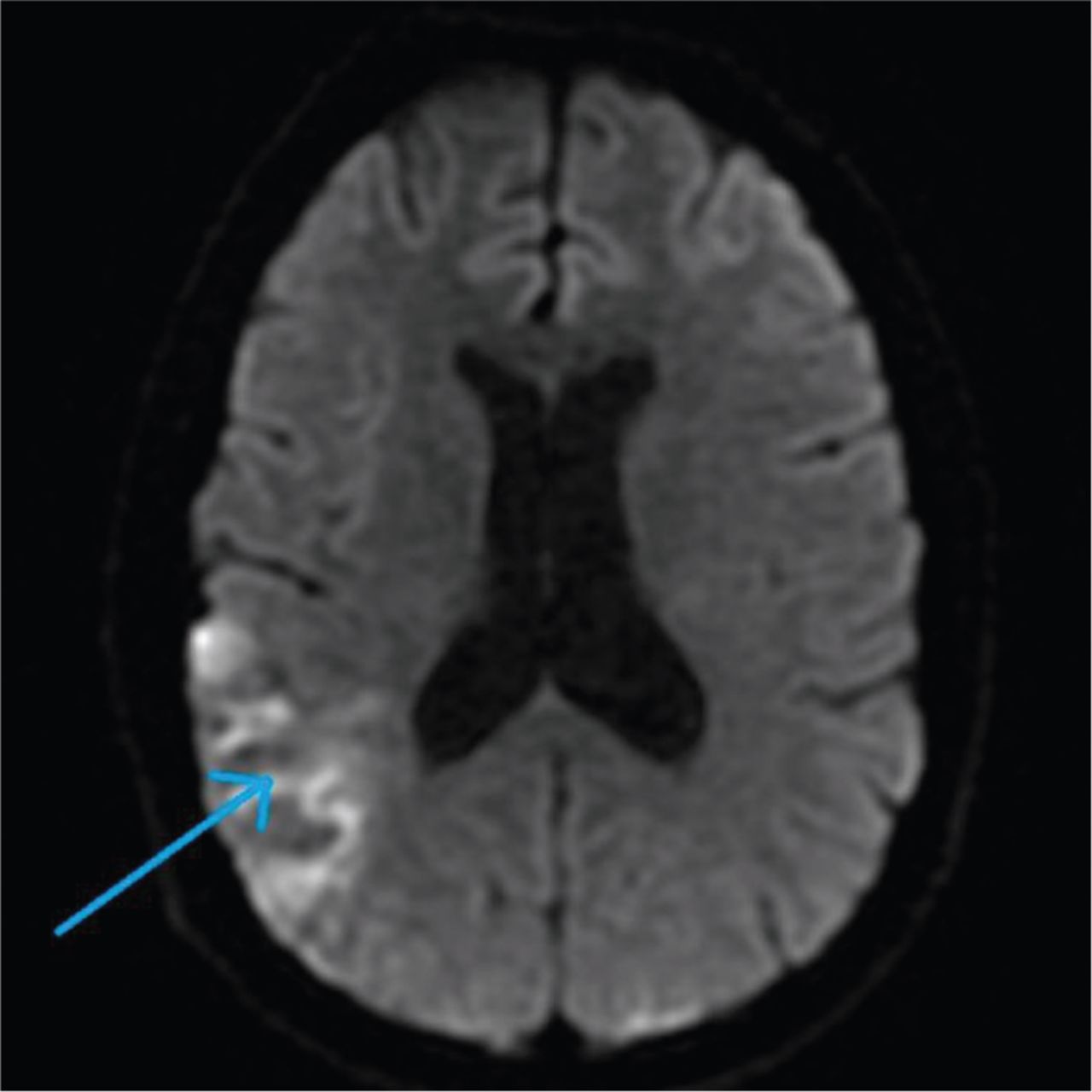
Diffusion weighted magnetic resonance imaging of the head showing multifocal cerebral and cerebellar infarcts with cytotoxic oedema.
On the 9th day of admission, the liver function test was done and came back deranged with bilirubin of 13.7 μmol/L, alanine aminotransferase of 212 U/L, alkaline phosphatase of 188 U/L, gamma-glutamyl transferase of 415 U/L, albumin of 29 g/L with normal international normalised ratio and platelets. Previous liver function tests were normal. Computed tomography of the chest, abdomen and pelvis with contrast showed bilateral pulmonary embolism, kidneys and spleen infarction, and multiple liver metastasis with unknown primary. He was started on treatment dose of low-molecular weight heparin for pulmonary embolism. Magnetic resonance imaging of the liver showed multiple liver metastasis with primary mass in the tail of the pancreas (Fig 2).
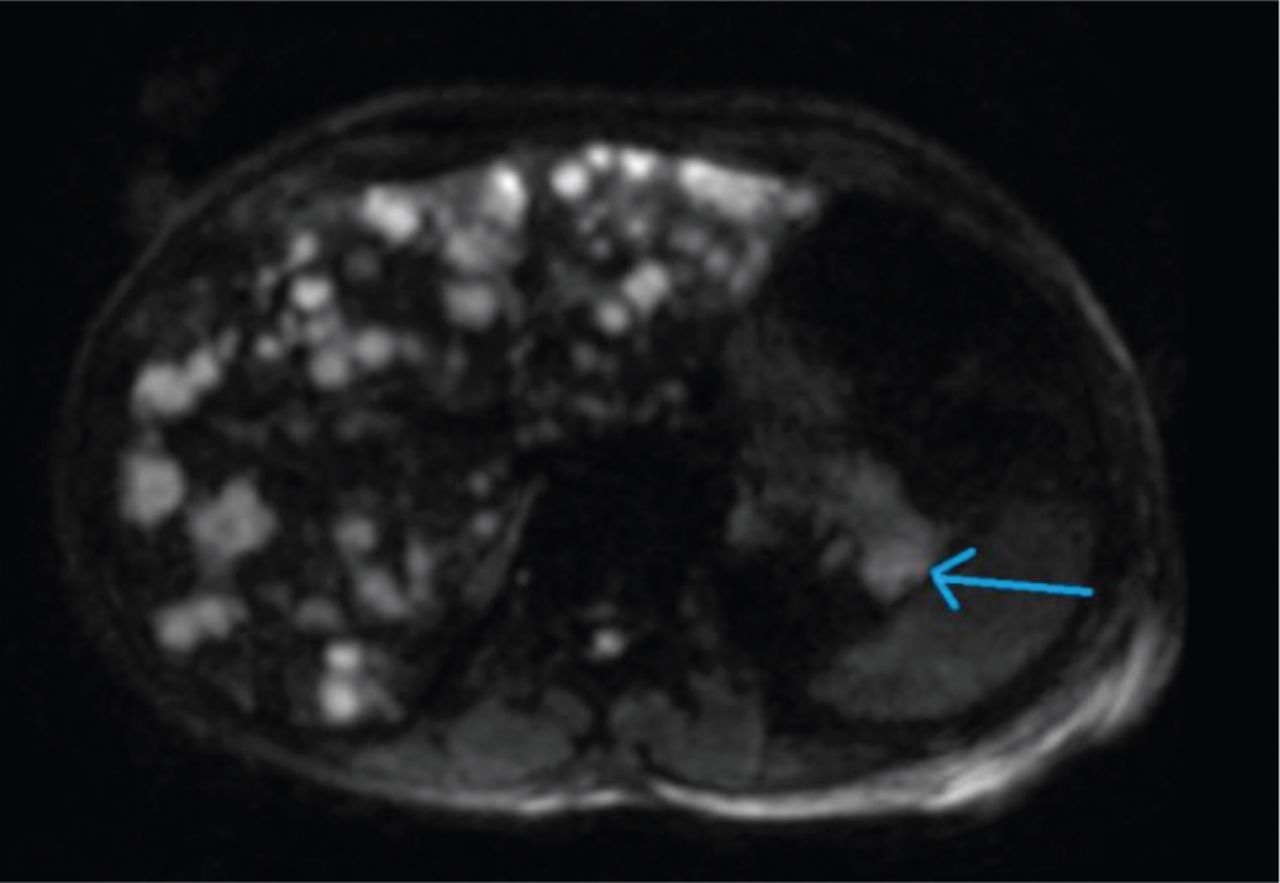
Magnetic resonance imaging of the liver showing primary malignancy in the tail of the pancreas (35 × 20 mm) with hypovascular liver metastasis; the scan was limited due to motion artefacts.
Antiphospholipid antibodies, HIV, hepatitis and vasculitis screening were negative, and non-invasive liver tests (autoimmune liver antibodies, alpha-1 antitrypsin, serum ceruloplasmin and iron studies) were normal. Cancer screening showed high carbohydrate antigen 19-9, >10,000 U/mL, normal alpha-fetoprotein and prostate specific antigen levels. The patient's mother mentioned that he had attended the general practitioner surgery 3 months previously for right leg sprain and the acute emergency care (AEC) unit in hospital 2 months previously for left leg cellulitis. D-dimer in AEC unit was very high, 6,500 ng/mL. The clinical events explained that he most likely developed Trousseau's syndrome 3 months previously and the embolic phenomena were due to rare marantic endocarditis (non-bacterial thrombotic endocarditis) secondary to pancreatic cancer. The multidisciplinary team advised for ultrasound-guided biopsy of liver metastasis, but sadly the patient passed away the next day.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.