
A 38-year-old man with diabetes presented with lethargy, night sweats, weight loss, right-sided pleuritic chest pain, fever and rigors, and hyperglycaemia. Chest X-ray and computed tomography (CT) of chest demonstrated multifocal inflammatory changes within the lungs.
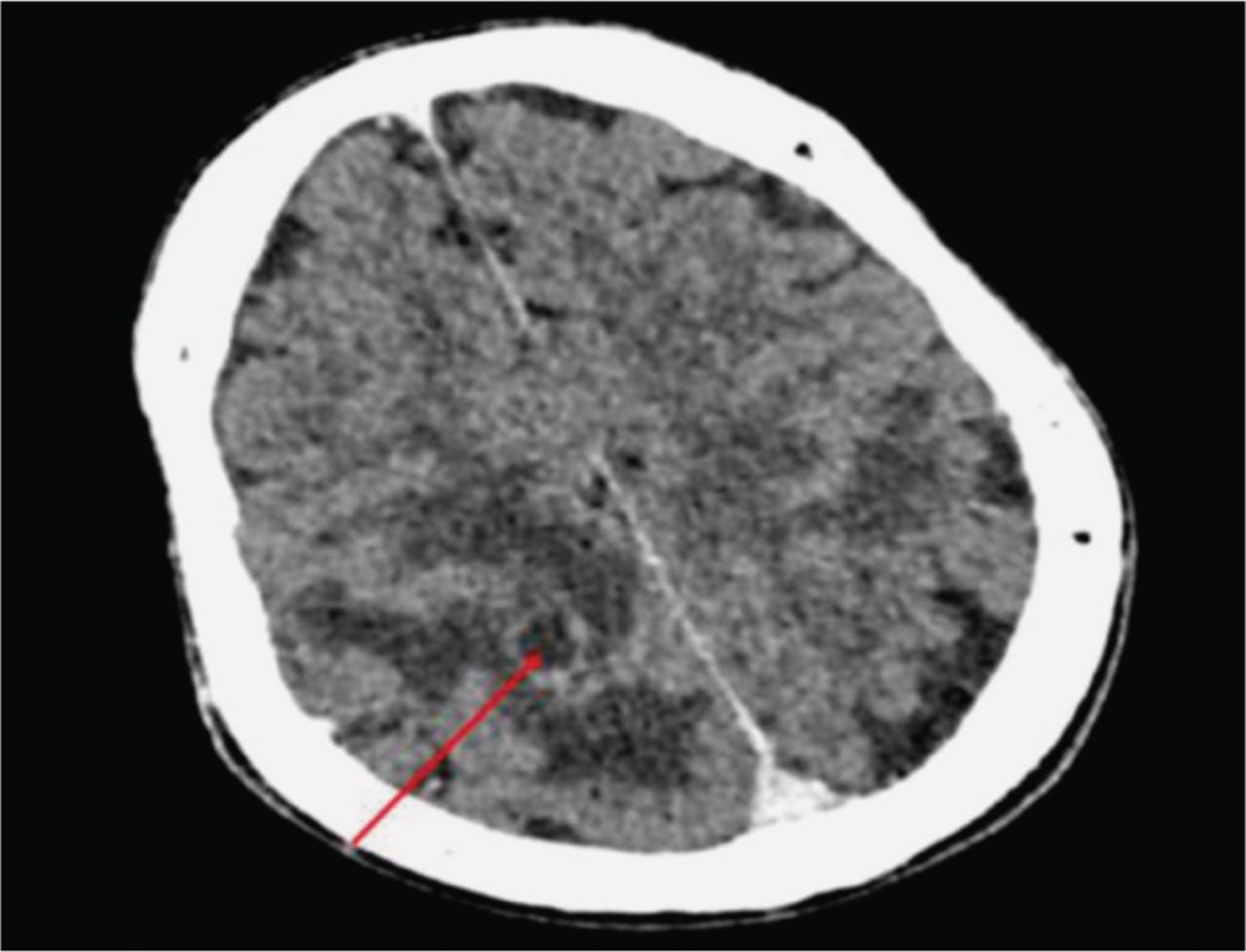
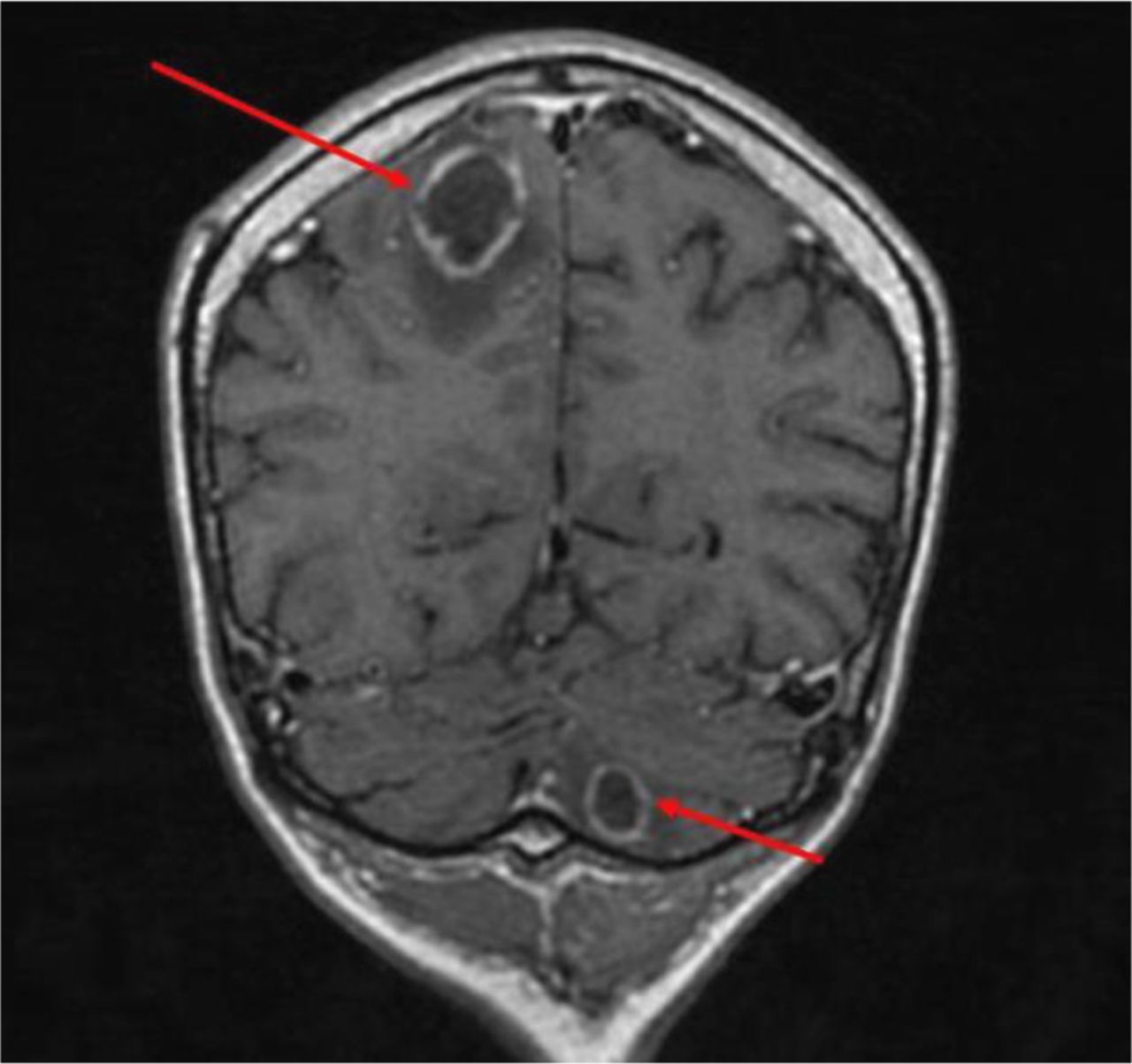
Differential diagnoses included atypical pneumonia and tuberculosis (TB). Intravenous (IV) antibiotics and insulin for uncontrolled diabetes were commenced. Bronchoscopy was requested to rule out TB. He subsequently developed left-sided weakness. An urgent CT of the head demonstrated bilateral, but more marked right-sided low-attenuation intra-cerebral lesions with vasogenic oedema. Magnetic resonance imaging of the brain confirmed ring enhancing lesions, likely tuberculomas (Fig 1). TB treatment and IV dexamethasone were initiated. He developed worsening neurology with meningism and bulbar weakness. A further CT of the head demonstrated worsening bilateral ring-enhancing lesions and vasogenic oedema (Fig 2). The neurosurgeons performed a mini-craniotomy and aspiration of the right parietal brain abscesses; polymerase chain reaction testing for TB was negative. Histology and cultures showed pauci-septate branching non-pigmented fungal hyphae and Apophysomyces variabilis. A diagnosis of central nervous system (CNS) mucormycosis was made; isavuconazole with IV liposomal amphotericin was commenced. Despite 4 weeks of treatment, deterioration continued, leading to his death.

Coronal T1 weighted magnetic resonance imaging with contrast showing multiple ring enhancing lesions (arrows) with surrounding oedema in the right parietal lobe and left cerebellum.
Axial computed tomography of the head with contrast 2 days after presentation showing worsening vasogenic oedema around the ring enhancing lesion in the right parietal lobe (arrow).
Mucormycosis is an opportunistic fungal infection. Prevalence is low in developed countries compared with developing nations, like India, where prevalence is 70 times higher.1 Common causes for CNS involvement are intravenous drug use (62%) and uncontrolled diabetes (43%).2 Mortality has been reported as 46%, with 68% in disseminated infections.3 Histology and culture are essential for diagnosis. Treatment is liposomal amphotericin and surgical debridement with the duration guided by radiological and clinical response.
The need to consider fungal infections in immunocompromised patients with worsening symptoms despite broad spectrum antibiotics is highlighted. Prompt treatment is paramount due to high mortality.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.