
Introduction
Granulomatosis with polyangiitis (GPA) is a rare multisystem autoimmune antineutrophil cytoplasmic antibodies (ANCA) positive vasculitis that, in rare cases, can affect the aorta causing aortitis, aneurysm and rupture.
Case presentation
A 50-year-old man presented with acute onset central chest pain, vomiting and haemoptysis with symptoms being preceded by arthritis of the right hand, ankle and knees. He was otherwise fit and well, non-smoker and without comorbidities.
Examination showed episcleritis and migratory arthritis without a rash. Electrocardiography was consistent with atrial fibrillation and serial troponins had a rising trend (42 ng/L to 376 ng/L to 1,300 ng/L). Repeated blood cultures were negative, but a vasculitic screen was positive for proteinase-3 (74 IU/mL).
An initial high-resolution computed tomography (CT) on admission was suggestive of right sided pulmonary haemorrhage (Fig 1).

Computed tomography suggestive of right sided pulmonary haemorrhage.
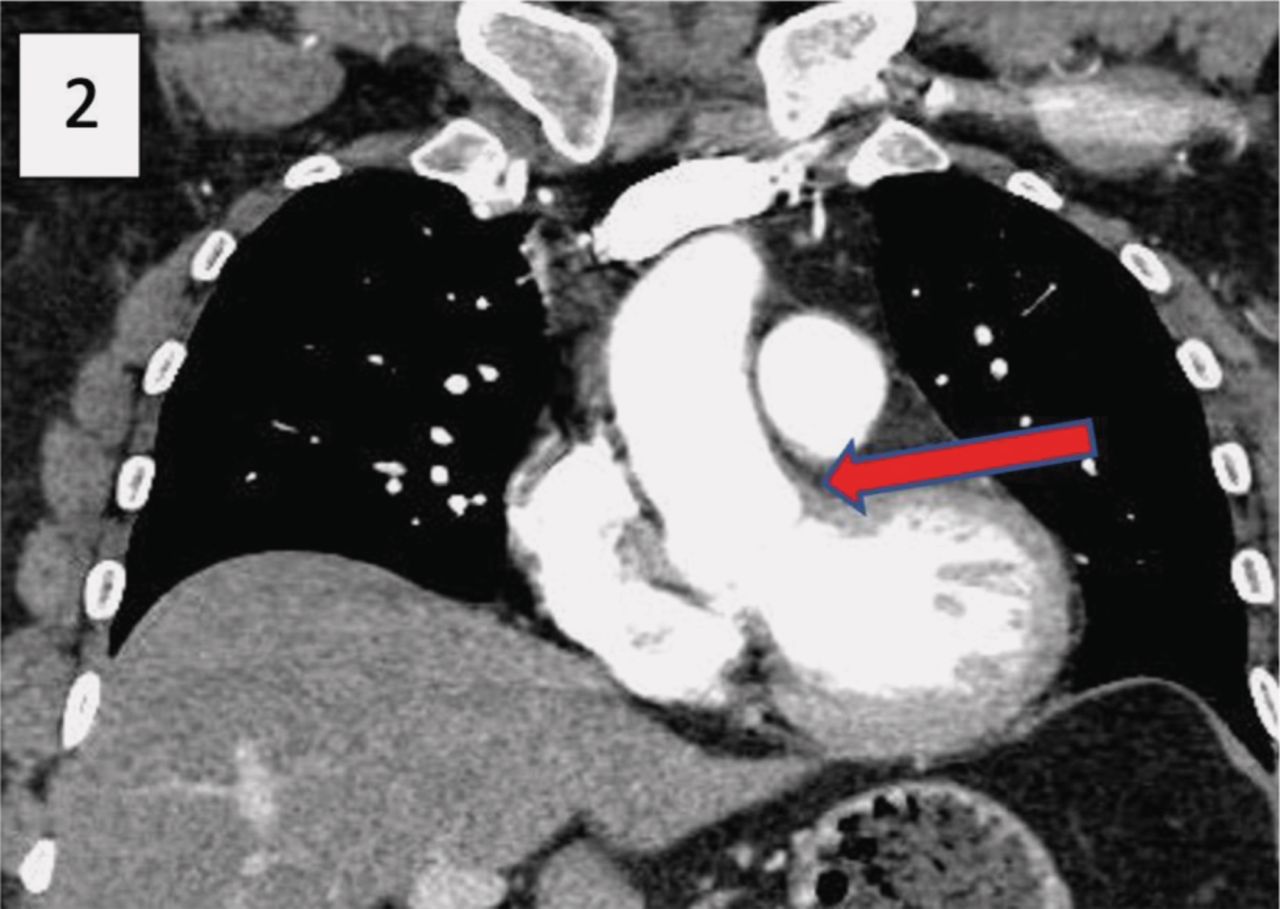
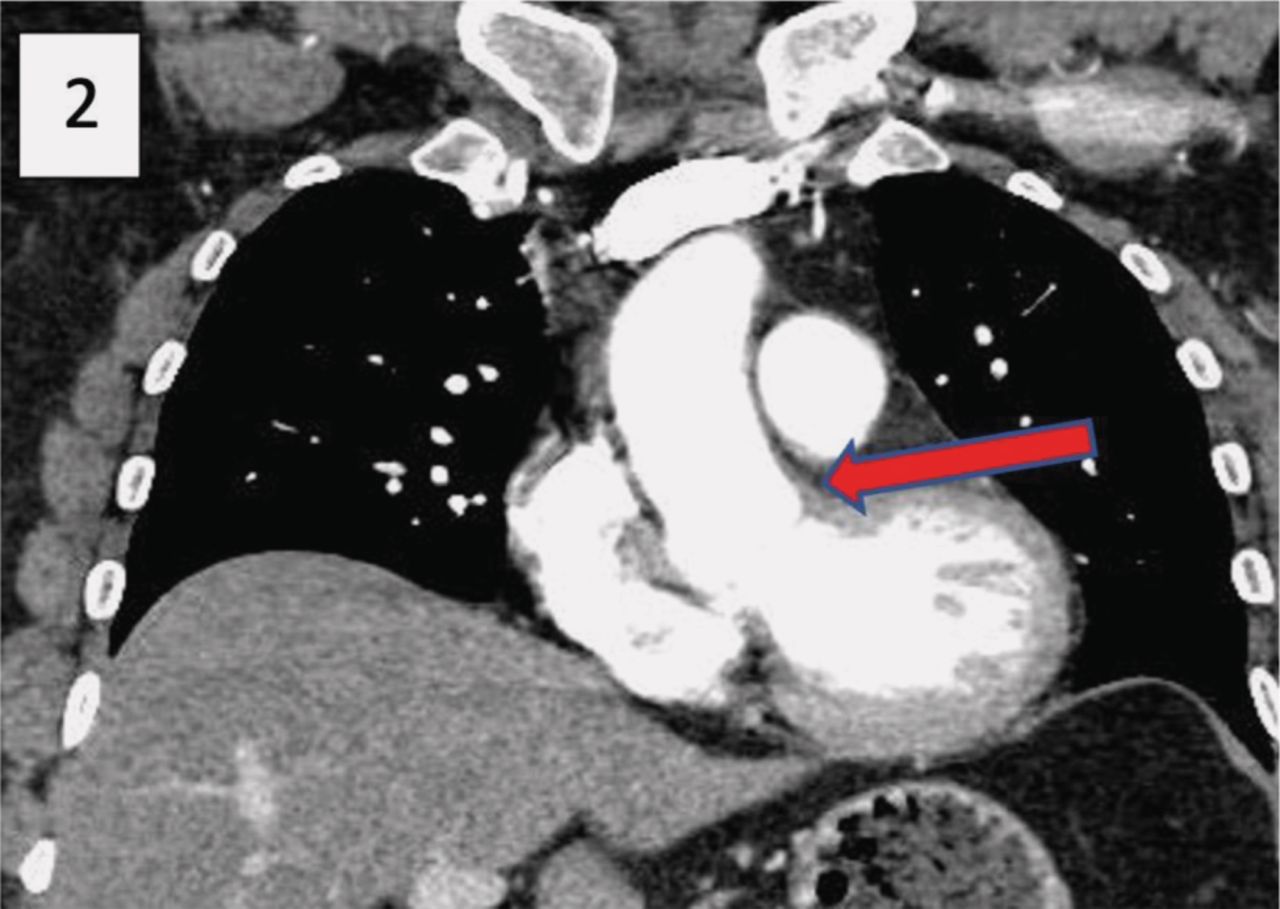
Computed tomography showing complete resolution of ascending aorta thrombus lesion.
A subsequent CT of the aorta 3 days later showed a new low-density filling defect in the aortic sinus, arising from the left/right coronary commissure and associated with minor thickening of the valve leaflets on that side. This was confirmed on echocardiography that showed a 1.79 cm × 0.64 cm lesion arising from the commissure of the left and right coronary cusps. This appeared to be attached to the aortic wall and moved independently of the valve leaflets.
The impression was that the mass was likely to represent a thrombus rather than an infective vegetation considering its position and time of appearance. The patient was commenced on intravenous (IV) heparin infusion with target activated partial thromboplastin time ratio (APTR) of 2 and IV methylprednisolone. Repeat CT of the aorta 3 days later showed reduction in volume of the low attenuation material. Overall, the appearances favoured thrombus that may had formed at a point of intimal inflammation or injury secondary to an underlying aortitis.
The patient was then switched to warfarin to achieve target international normalised ratio (INR) of 2 and was discharged with a reducing regimen of prednisolone. He also received a 6-dose course of cyclophosphamide as an outpatient. A repeat CT, 10 weeks later, showed complete resolution of ascending aorta thrombus lesion (Fig 2).
Discussion
GPA is a small vessel vasculitis most commonly associated with PR-3 antibodies. In one-fifth of cases, myeloperoxidase antibodies can also be present. PR-3 antibody positivity provides aid to the diagnosis and is also a marker of disease activity.1 The disease is characterised by granulomatous inflammation and necrosis of small and medium vessels, and most commonly affects the ears, nose, throat, respiratory tract and kidneys.2 Cardiac manifestations of GPA are rare and can include pericarditis, cardiomyopathy, coronary arteritis, valvular lesions and conduction abnormalities.3 Large vessels may also be affected, despite it being classified as a small vessel vasculitis. Specifically for the aorta, which was affected in our case, this can present with aneurysmal formation, dissection, rupture, regurgitation or death. In those cases, a possible overlap between ANCA-associated vasculitis and large vessel vasculitis has been suggested.4
Conclusion
We have presented a rare case of GPA presenting with thrombus of the ascending aorta that resolved following effective anticoagulation and immunosuppressive treatment.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.