
Introduction
Coronavirus mainly targets the respiratory system; however, various systemic complications are reported. In patients with moderate to severe COVID-19 infection, computed tomography (CT) of the chest can show a wide range of parenchymal changes, and, occasionally, extra-parenchymal findings such as pneumomediastinum. The authors present a case of COVID-19 infection complicated by spontaneous pneumomediastinum (SP) to highlight this rare complication.
Case presentation
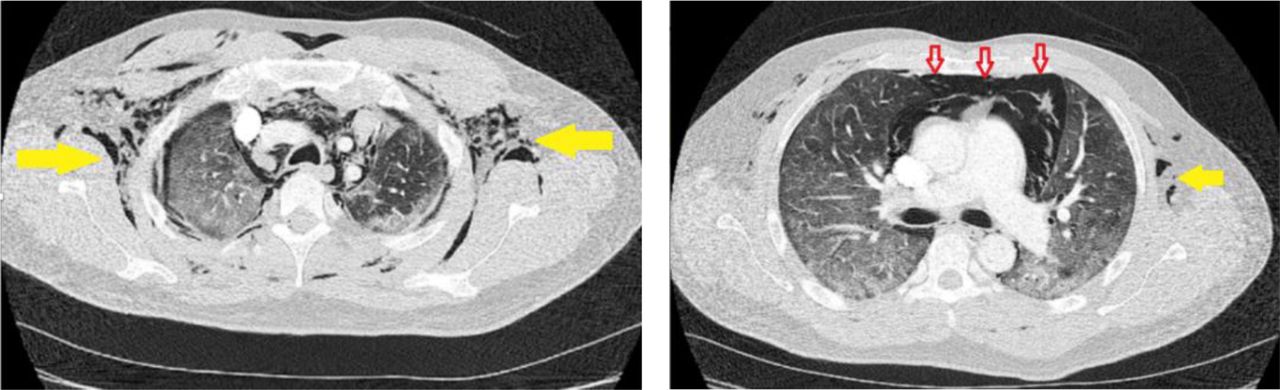
A previously healthy 42-year-old Asian man presented to the emergency department with a 10-day history of fatigue and dry cough and two days of high-grade fever along with shortness of breath. On presentation, oxygen saturation was 60% on air, heart rate was 118 beats/minute, blood pressure 130/80 mmHg, and respiratory rate 28 breaths/minute. Chest examination revealed bilateral basal fine crepitation, central trachea, and crepitus on palpation. The rest of the systemic examination was unremarkable. He denied chest pain, recent long-distance travel, leg swelling or rash. He was admitted and started on appropriate treatment. His PCR for SARS-CoV-2 was positive and remarkable bloods were a C-reactive protein 624 mg/L (0–6) and D-dimers 2,041 ng/mL (0–230). In view of the high D-dimer value, computed tomography pulmonary angiogram (CTPA) was carried out which was negative for pulmonary embolism, but revealed bilateral consolidation, extensive pneumomediastinum, surgical emphysema throughout the chest wall, and bilateral small pneumothoraces (Fig 1).

Computed tomography of the chest axial sections of pulmonary parenchymal window showing extensive ground glass opacities in both lung fields, showing extensive ground glass opacities in both lung fields, along with subcutaneous emphysema (yellow arrows) and pneumomediastinum.
A multidisciplinary team's opinion was to manage conservatively, to which he responded well with gradual reduction in oxygen requirement. He was eventually weaned off and was discharged on day 12. He was advised to follow up after 6 weeks.
Discussion
Macklin effect has been proposed as a possible aetiology for SP in non-ventilated patients.1,2 It starts with alveolar rupture secondary to direct alveolar injury, leading to air leaking and dissection along the bronchovascular sheaths and eventually spreading of air within the mediastinum.3 This can also lead to subcutaneous emphysema, as seen in our patient. The most common symptom of pneumomediastinum is acute retrosternal chest pain, which warrants early alert to rule out this dreaded complication in patients with suspected or confirmed COVID-19.2 However, our patient did not complain of retrosternal chest pain.
Although the treatment for SP is usually symptomatic and conservative, oxygen therapy could possibly lead to faster recovery.4 Loffi and colleagues consecutively studied 102 patients and found the incidence of SP to be 6%, and reported a mortality of one in six patients.1 Although isolated pneumomediastinum might be a self-limiting condition, patients with concurrent pneumopericardium, tend to have a less favourable outcomes.5–8 This could likely be due to a more severe hemodynamic risk associated with the presence of pneumopericardium. Pneumopericardium can be thought of as an extended complication of the Macklin effect.
Conclusion
Although no set guidelines have been devised, the management of SP in COVID-19 patients is largely conservative. Increased mortality is reported in patients with concurrent SP and pneumopericardium.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.