
Introduction
Type 2 diabetes mellitus (T2DM) is a significiant risk factor for coronary artery disease (CAD). The landmark EMPA-REG trial demonstrated that SGLT2 inhibition significantly decreased the risk of all-cause mortality (number needed to treat: 39 at 3.1 years) in patients with T2DM and CAD.1
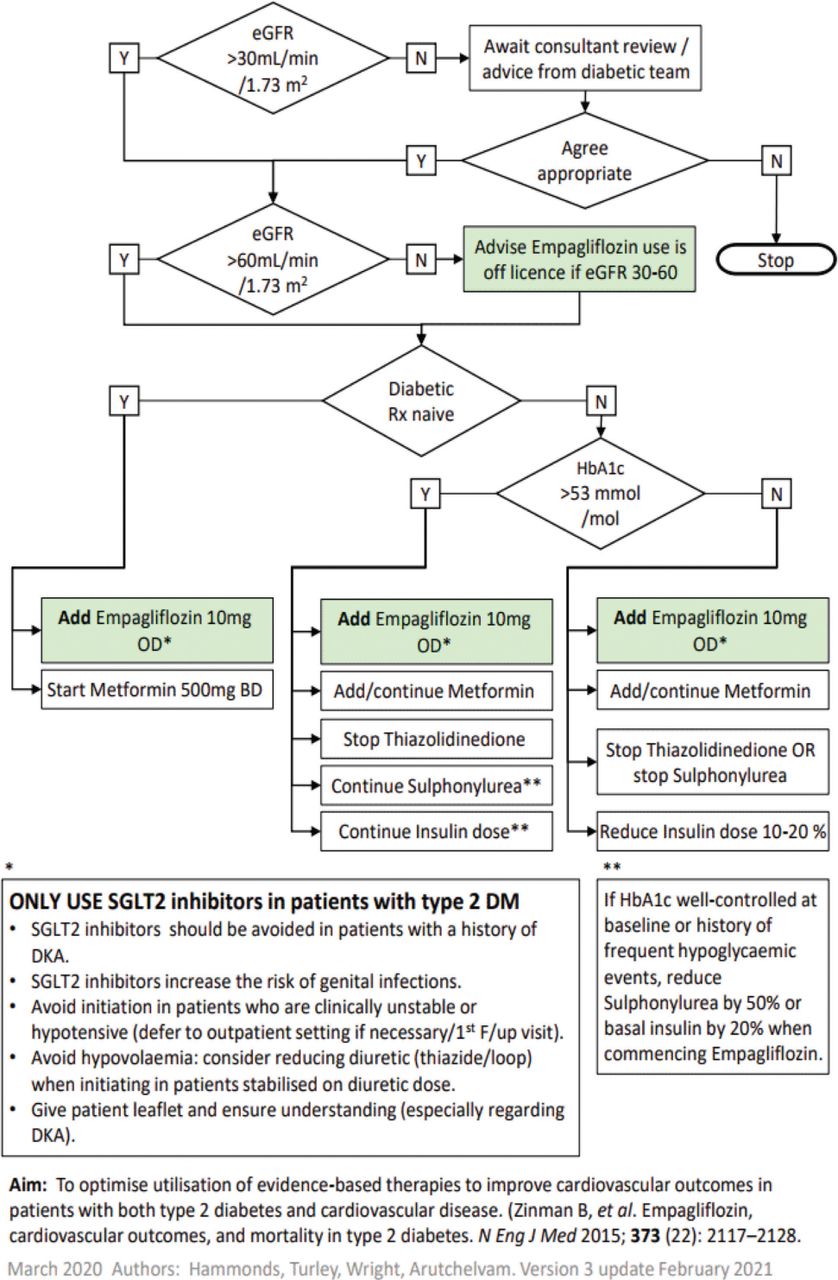
In a previous audit, we showed that six out of 259 (2.3%) diabetic patients were prescribed gliflozin on discharge. Therefore, a clinical protocol on SGLT2 inhibitor commencement (Fig 1) has been in place at James Cook University Hospital coronary care unit for all T2DM patients who present with an acute coronary syndrome (ACS; ST segment elevation myocardial infarction or non-ST segment elevation myocardial infarction). This protocol is in line with the national CaReMe intiative endorsed by the British Cardiovascular Society.
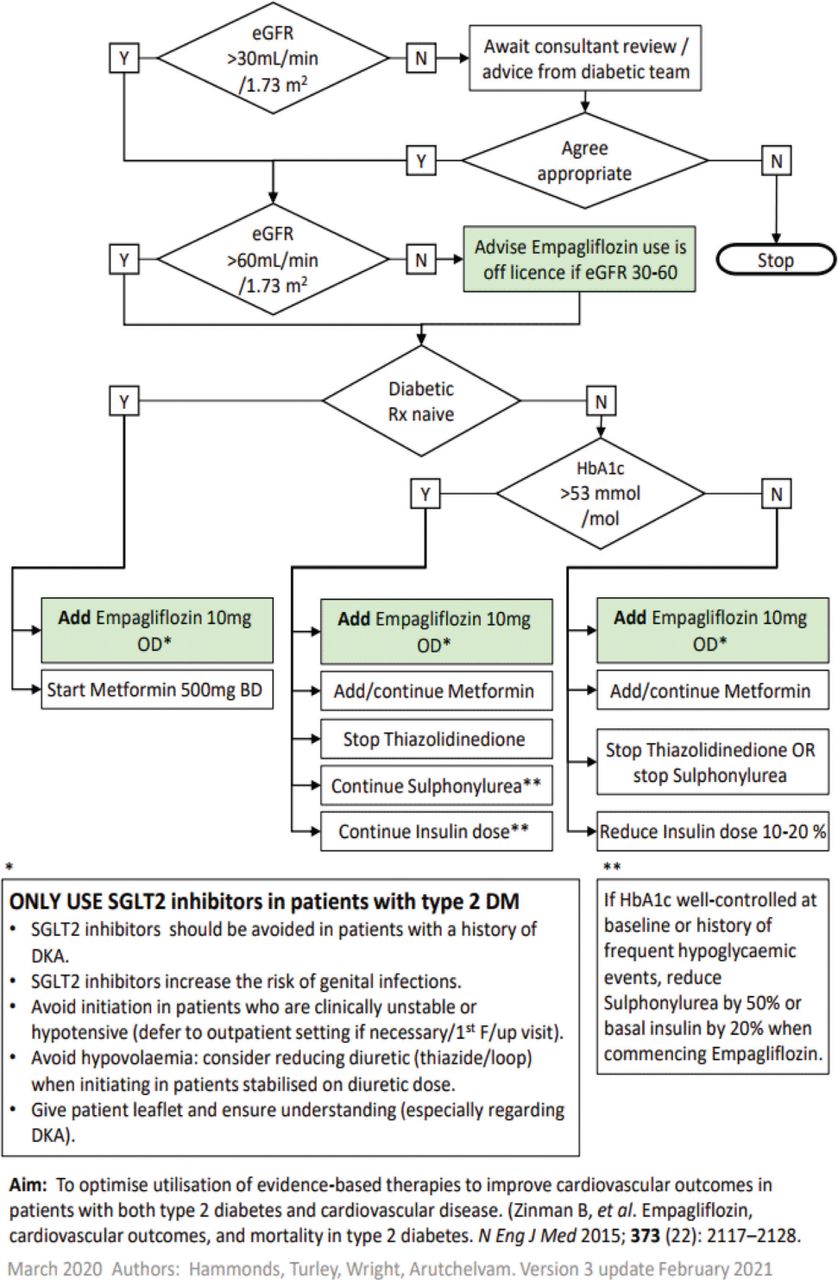
Protocol for commencing empagliflozin (SGLT2 inhibitor) in patients with type 2 diabetes mellitus and confirmed voronary artery disease.
Objective
To evaluate whether T2DM patients admitted with ACS are commenced on SGLT2 inhibitor prior to hospital discharge.
Methods
Data were collected retrospectively from the validated Myocardial Ischaemia National Audit Project (MINAP) database for the months of August and September 2020. HbA1c and eGFR results were gathered from the hospital electronic biochemistry database while diabetic medication was recorded from the British Cardiovascular Interventional Society (BCIS) discharge letter.
Results
Forty-two patients with T2DM admitted between August and September 2020 with ACS and subsequently discharged were audited. In this reaudit, 11 out of 42 (26%) T2DM patients were prescribed gliflozin on discharge. Prescribing of an SGLT2 inhibitor in T2DM patients with CAD has risen.
Patients were divided between ward areas: coronary care unit (CCU) versus cardiology ward admission (Table 1). The CCU group had a higher percentage of patients, 37%, prescribed an SGLT2 inhibitor compared with 17% of patients in the cardiology ward category.
Data for patients in our cohort
The main reason for this difference is that all CCU patients are reviewed daily by cardiology consultants, while ward patients are generally looked after by junior doctors and specialty interventional nurses. Although a clinical protocol is available, junior doctors and specialty interventional nurses were cautious in integrating SGLT2 inhibitor into take-home medication.
Conclusion
SGLT2 inhibitor is proven to have mortality benefits in patients with CAD and T2DM. Our clinical protocol was effective in increasing numbers of patients discharged on an SGLT2 inhibitor. To improve this further, we have instigated cardiologist specialist nurse prescribing of SGLT2 inhibitor into daily practice. In addition, we enforced the SGLT2 inhibitor pathway during the junior doctors' and CCU nurses' meeting. We aim to reaudit after 1 year.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.