
ABSTRACT
Introduction Lumbar puncture (LP) is a widely used diagnostic method in patients of all ages. Blood-contaminated cerebrospinal fluid samples are frequent and may compromise diagnostic accuracy.
Objectives We determined age-specific incidences of traumatic LPs (TLPs) in adults and examined factors that accounted for the incidence of TLPs.
Methods Erythrocyte count data from 15,812 LP procedures (2,404 were performed twice) were collected from hospital records of patients aged from 18 to 104 years. The incidence of TLPs in a patient's second LP procedure was evaluated with logistic regression analysis using the first LP, the time between the procedures and age as predictors.
Results The incidence of TLP in the second procedure was at least double that in the first procedure. If the first procedure was traumatic, the odds ratio of a TLP in the second procedure was 7–40-fold. One day between the successive procedures was associated with an over 10-fold odds ratio increase of TLP, and a week was still 4–8-fold odds ratio increase. Age was also associated with the incidence of TLP.
Conclusions Two factors (a week or less between a patient's two LP procedures or a traumatic first LP) multiply the odds of the second procedure being traumatic and contribute to whether a patient's following LP procedure is successful.
Introduction
Lumbar puncture (LP) provides a unique window to examine the state of the central nervous system through proper analyses of cerebrospinal fluid (CSF).1 With multiple indications for diagnosis, intrathecal therapy or spinal anaesthesia, the LP procedure is widely performed on patients of all ages. In adults, common diagnostic indications for LP pertain to inflammation of the central nervous system manifesting as various forms of meningitis, neurological diseases and conditions (such as Alzheimer's disease, Parkinson's disease, multiple sclerosis, autoimmune encephalitis, epileptic seizures, memory concerns and altered mental status), as well as to differentiation of subarachnoid haemorrhage (SAH).2–15 As the populations around the world are ageing, many of these diseases and conditions become more prevalent, and the clinical need for diagnostic LP is likely to increase.
For diagnostic accuracy, it would be essential that a patient's CSF is not contaminated by blood leakage from the capillaries or venules that may possibly be damaged by the spinal needle. Ideally, for minimal diagnostic uncertainty, the collected and analysed CSF samples should be free from erythrocytes but reflect the actual state of the CSF. However, in the real world, CSF samples are often blood-contaminated, defined as traumatic LPs (TLPs) according to how many red blood cells (RBC) are in the CSF sample. Based on a rough criterion of visual blood in CSF (about 300–500 erythrocytes/μL), the reported incidences of TLPs in adult patients vary between 7% and 28%.2,16–22 The incidence of TLPs is higher in infants and appears to increase also at older age indicating a U-shaped pattern.18 Common causes that may lead to TLPs include obesity of the patient, abnormal spinal anatomy, poor visibility and palpability of lumbar structures, patient agitation and anxiety during the procedure, coagulation disorders, physicians' inexperience in performing LP and multiple attempts before success in getting the CSF sample.
This retrospective study of electronic health records aimed to determine the age-specific incidences of TLPs in adults and investigate factors that account for the incidence of TLPs in a large sample of adult patients, representing a wide range of age. Depending on medical reasons or personal treatment protocols, patients may undergo several LP procedures performed at varying intervals. Repeated procedures may increase the incidence of TLPs in subsequent LPs.17,23–25 Therefore, we examined the independent contributions of a patient's first LP to the incidence of TLPs in the following LP procedure by addressing the following questions: was the first LP procedure traumatic, what was the time between the successive procedures and how old was the patient at the time of the first procedure?
Methods
Erythrocyte count data in CSF samples of adult patients were retrospectively gathered from hospital electronic health registers covering the period from 1 January 2011 to 31 May 2017. The data were obtained from LP procedures performed in Tampere University Hospital and Turku University Hospital located in southern Finland. These two hospitals provide tertiary care for about a 1.8 million population, including over 1.4 million adults. The data were eligible for the present study if the patients were at least 18 years old at their first LP. The status of being the first LP procedure was verified by checking that the patient had not undergone an LP procedure during the preceding year 2010. A time longer than 1 year between the successive LP procedures was considered a sufficient washout period.
Hospital laboratories determined routinely the erythrocyte count values from the second or third vial of the CSF sample with cytometric methods according to their standard procedures. Besides the erythrocyte count data, the dataset provided to us was quite limited containing only the date of the procedure, hospital department code and patient's age.
The present data comprised erythrocyte values from 15,812 LP procedures performed on adult patients for various clinical indications. At the time of the procedure, the patients' age ranged from 18 to 104 years. Erythrocyte data were obtained from successive procedures from 2,404 patients.
The regional Ethics Committee of the Expert Responsibility area of Tampere University Hospital approved the study. Since the study was a sole register-based study and personal identifiers were removed from the patient data before the analysis, no informed consent from individual patients was needed.
Mean, standard deviation (SD) and range are given as descriptive data for patients' age, whereas median, interquartile range (IQR) and range are given for the time between the patients' first and second LP procedures. A cumulative distribution curve is used as the main descriptive statistics for erythrocyte count data. This curve illustrates the respective proportions of CSF samples, which denote the incidence of TLPs for any given criterion of the erythrocyte count. For any chosen criterion, the incidence of TLPs is the vertical distance (in %) from the corresponding curve point up to the 100% point. For this study, we chose ≥500 and ≥10,000 erythrocytes/μL as two criteria of TLPs, corresponding to common levels of how many erythrocytes were considered acceptable in a nontraumatic CSF sample. The former criterion corresponds roughly to the lower limit of visual blood in the CSF sample, while the latter indicates a clearly blood-contaminated CSF of which approximately 0.2%–0.3% of the sample volume is occupied by blood.20
Differences in the incidence of TLPs between the first LP and second LP were described in five patient age categories (18–29 years, 30–49 years, 50–64 years, 65–74 years and ≥75 years) using the two criteria of TLPs.
Logistic regression analysis was performed to assess factors that may account for the incidence of a TLP in a patient's second LP procedure, defined as a dichotomous variable by the criterion of ≥500 erythrocytes/μL or ≥10,000 erythrocytes/μL. The following categorical variables were entered into the model as predictors: traumatic first LP according to both criteria of TLPs (yes/no), the time category indicating the time between the second and first procedure (within 1 day (≤1 day), within a week (2–7 days), within a month (8–30 days) and within a year (31–365 days)) and the earlier-mentioned five age categories. Times longer than 365 days between the first and second LP were excluded from the analysis. Estimated odds ratios (ORs) of the entered predictors are reported with 95% confidence intervals (CIs). The robustness of predictors and related ORs was verified by performing both backward and forward regression analyses.
Statistical analyses were done with IBM SPSS statistics software (version 27.0). A p<0.05 was considered statistically significant.
Results
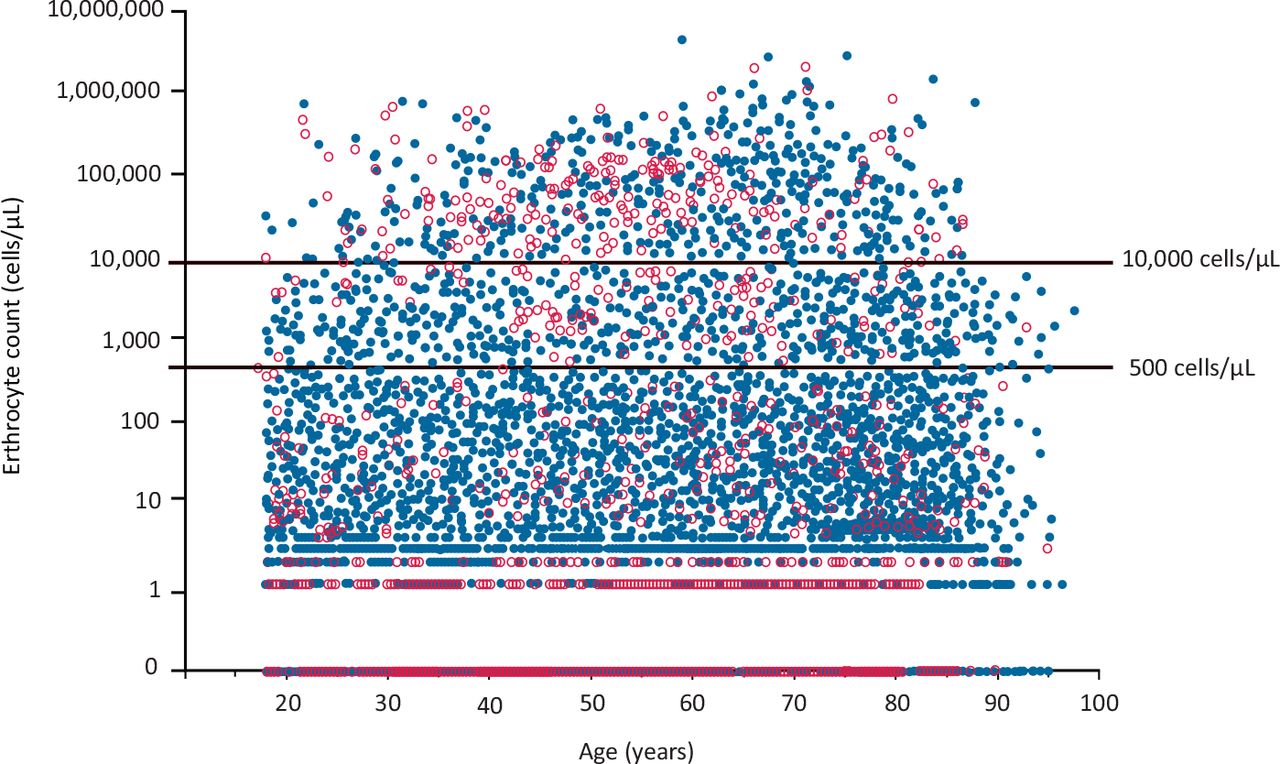
The mean age (SD) of 13,408 patients was 54.2 years (18.2) at the time of the first LP procedure. The youngest patient was 18 years old and the oldest was 104 years. A total of 2,004 first LP procedures were performed among patients aged 18–29 years old, 4,325 procedures for those aged 30–49 years old, 4,309 procedures for those aged 50–64 years old, 3,057 procedures for those aged 65–74 years old, and 2,117 procedures for those aged 75 years or more. Total numbers of the second LP procedures in these age categories were 211, 566, 747, 572 and 308, respectively. The median time (IQR) between the patients' first and second procedures was 7 days (2–82). A total of 435 procedures were repeated within 1 day, 789 within 1 week, 389 within 1 month and 518 within 1 year. The erythrocyte count values of CSF samples are plotted against the patients' age in Fig 1, the data broken down by the patients' first and second procedures.
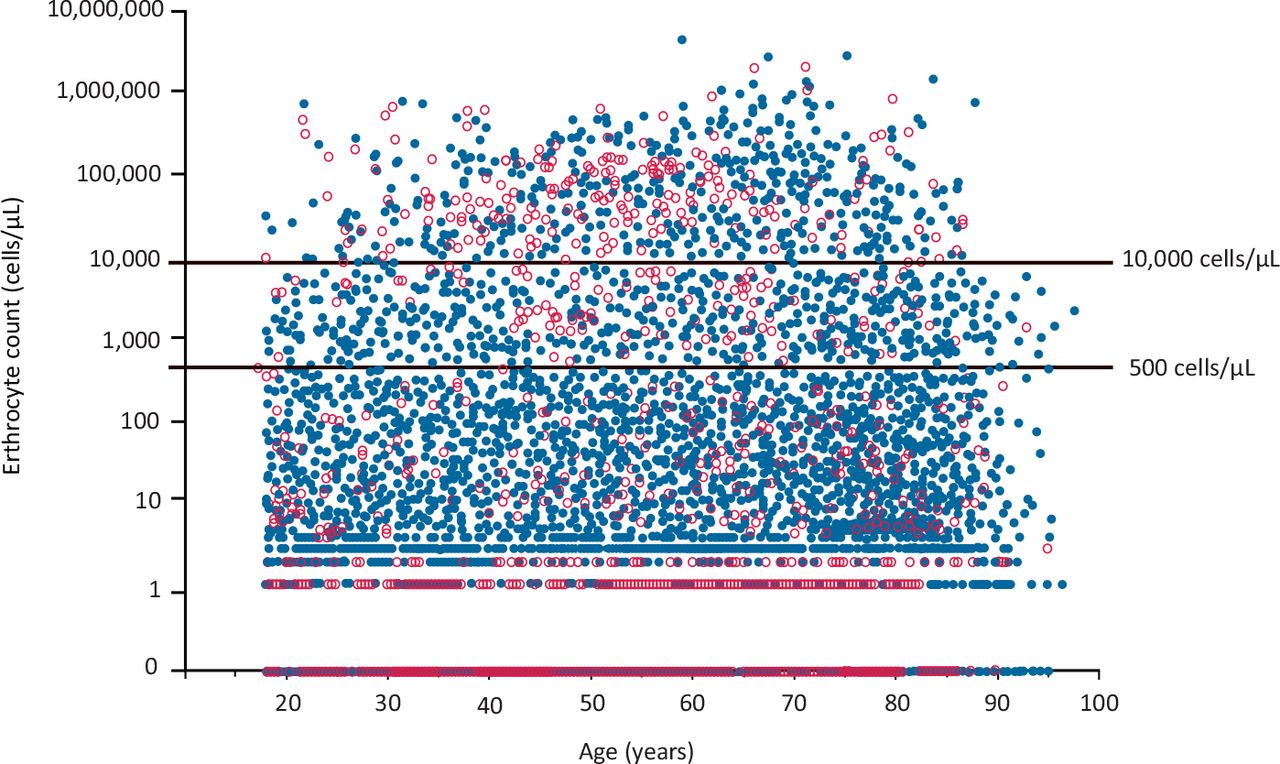
Erythrocyte count values from LP procedures of adults plotted against the patient's age. The data obtained from the first (blue dots) and second (open red dots) LP procedures is shown separately.
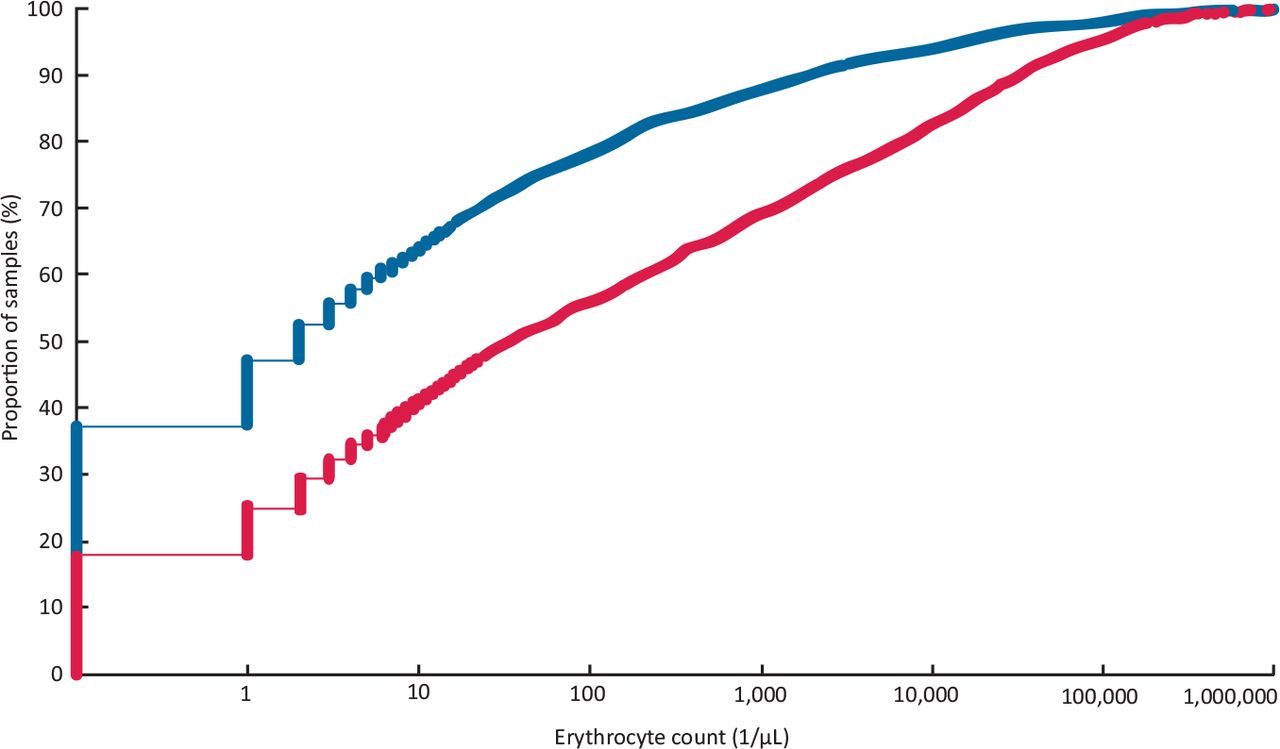
Cumulative distribution curves of erythrocyte count data in the first and second LP procedures are shown in Fig 2. In the first procedure, the incidence of erythrocyte-free CSF samples was 37.4%, while in the second procedure, it was 17.8% (p<0.0001). In the first procedure, the incidences of TLP, according to criteria of ≥500 erythrocytes/μL and ≥10,000 erythrocytes/μL, were 13.7% and 5.0%, respectively. In the second procedure, the respective incidences were 35.1% and 17.7%, which differed significantly from the first procedure (p<0.0001).
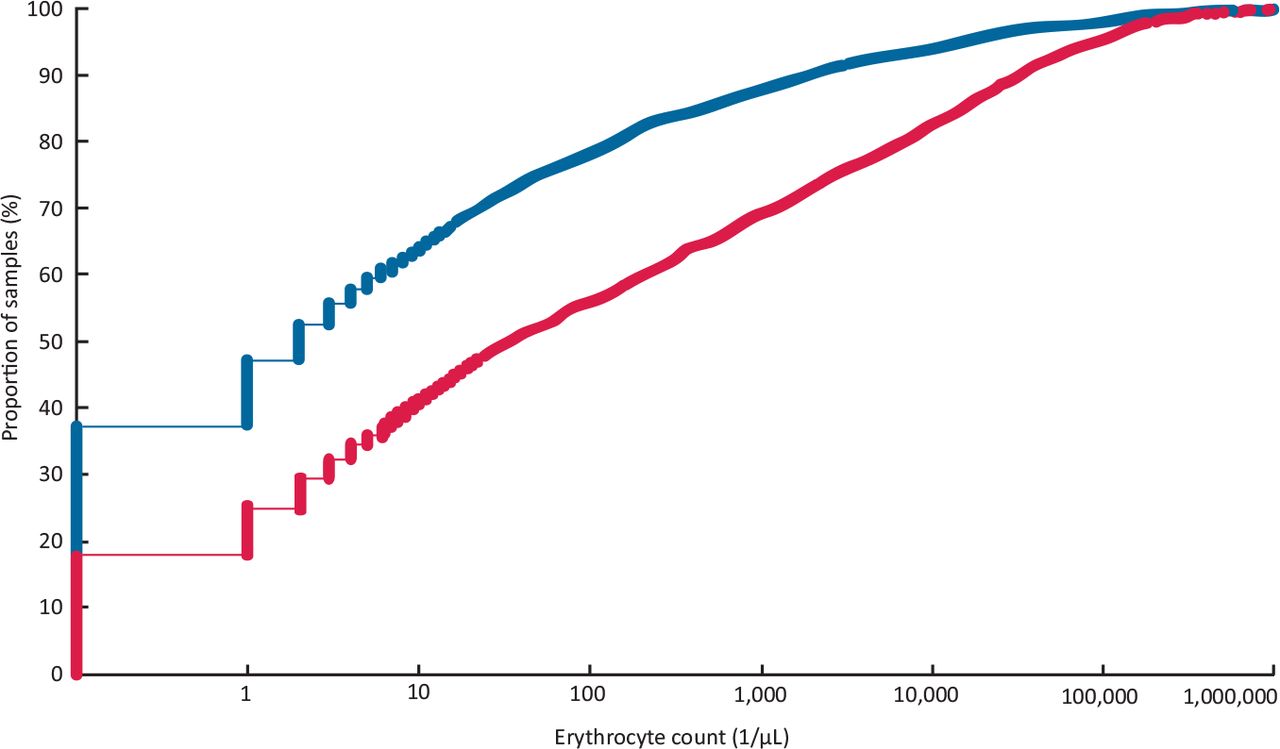
Cumulative distribution curves of the erythrocyte count data in the first LP (blue line) and second LP (red line) procedures in adult patients.
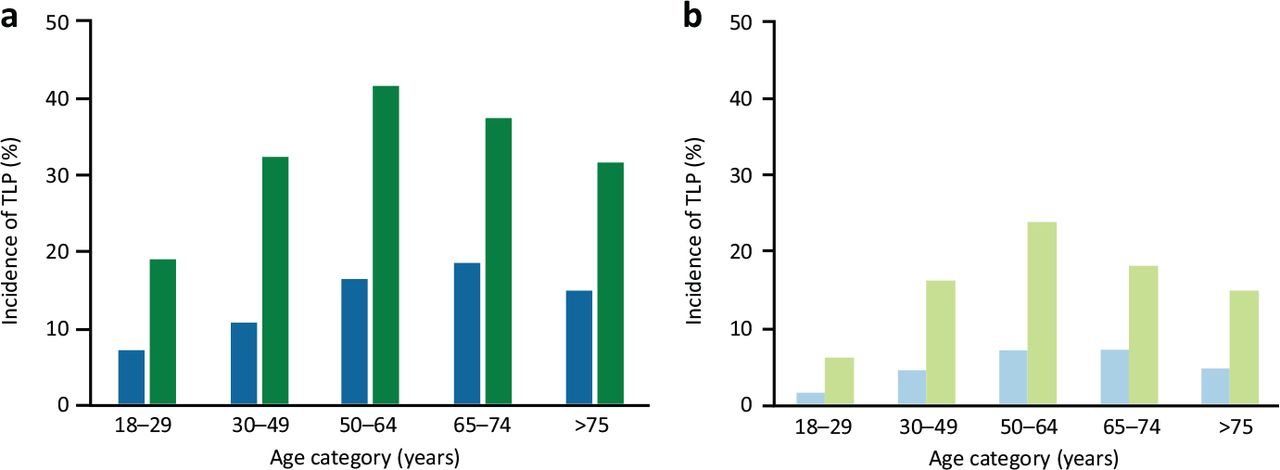
The incidences of TLPs in the first and second LP procedures, broken down by the age categories, are shown in Fig 3 for both TLP criteria. In all age categories and for both criteria, the incidence of TLPs in the second procedure was consistently significantly higher than in the first procedure (chi-squared test, p<0.0001), being at least twice as high.
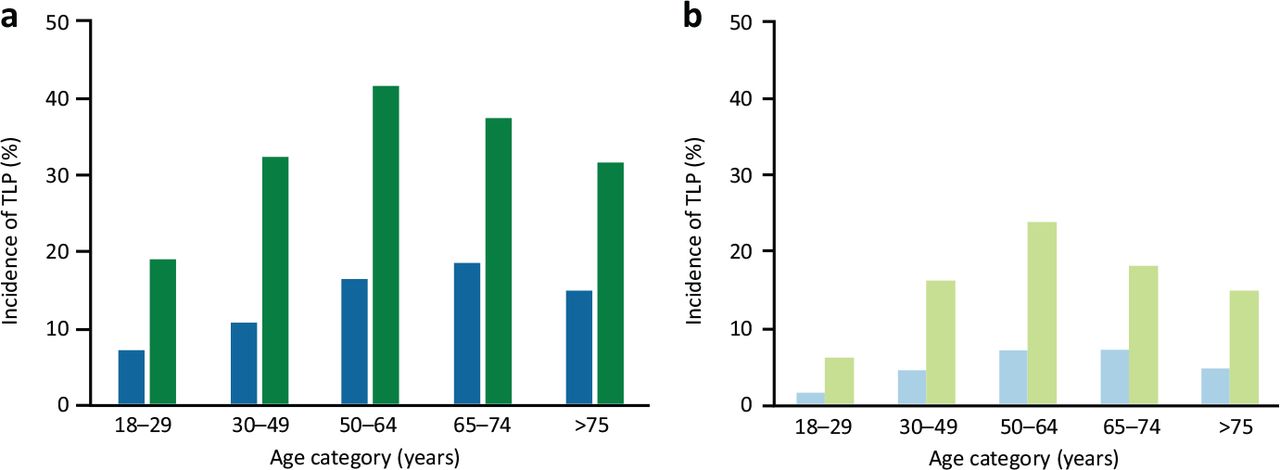
Incidence of TLP in the five age categories of adults in the first LP (blue) and second LP procedure (green) according to criterion of a) 500 erythrocytes/μL and b) 10,000 erythrocytes/ μL.
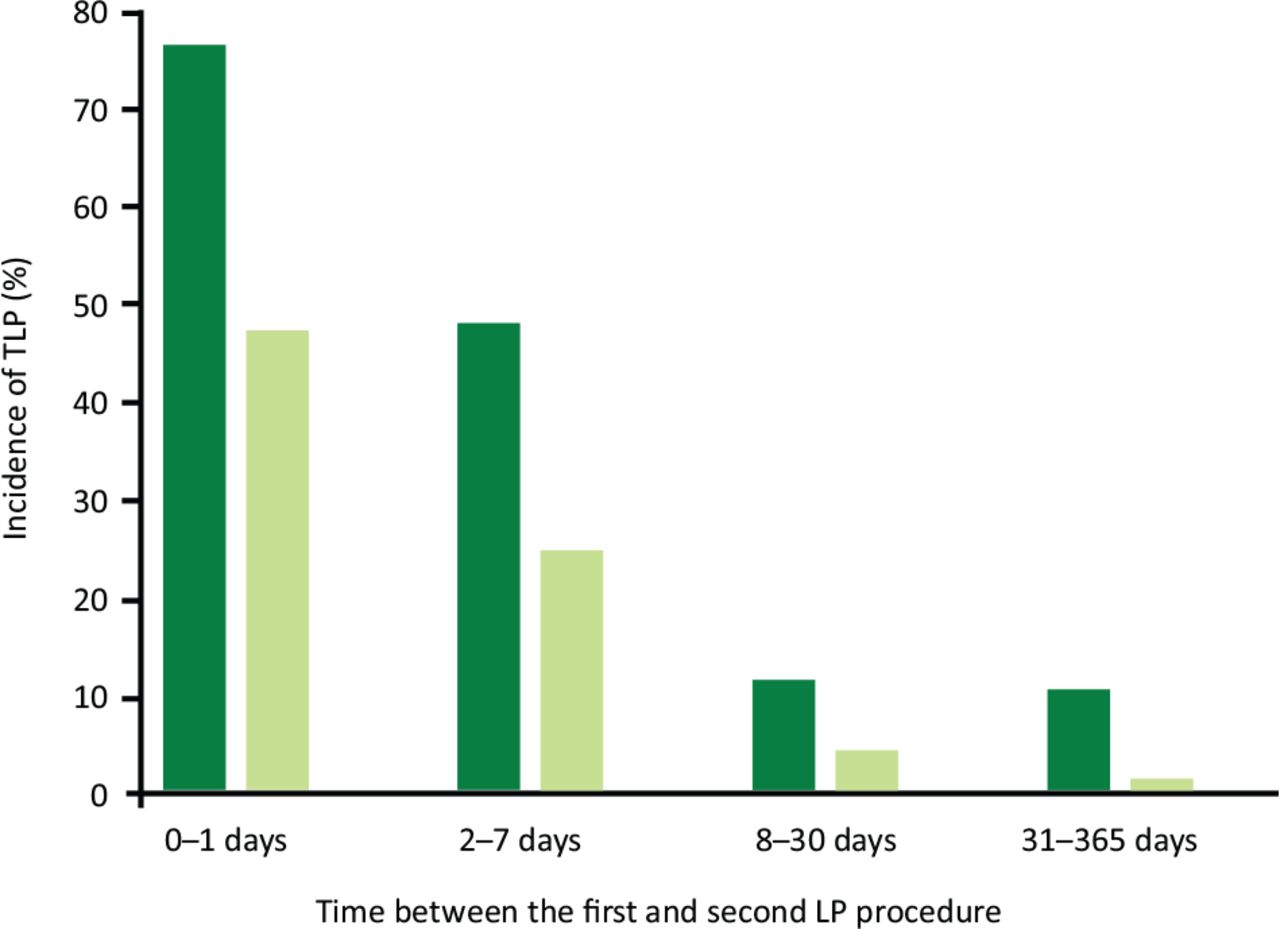
The incidence of TLPs in the second LP procedure broken down by the time category since the preceding first procedure is shown in Fig 4 for both TLP criteria. The longer the time since the first procedure, the lower the incidence of TLPs in the second procedure. With the criterion of ≥500 erythrocytes/μL, the incidence of TLP was 76.1% if the successive LPs were performed within a day and plateaued to about the 10% level within a month. With the criterion of ≥10,000 erythrocytes/μL, the pattern was similar except that the incidence of TLPs was halved compared with the low criterion and virtually vanished with time.
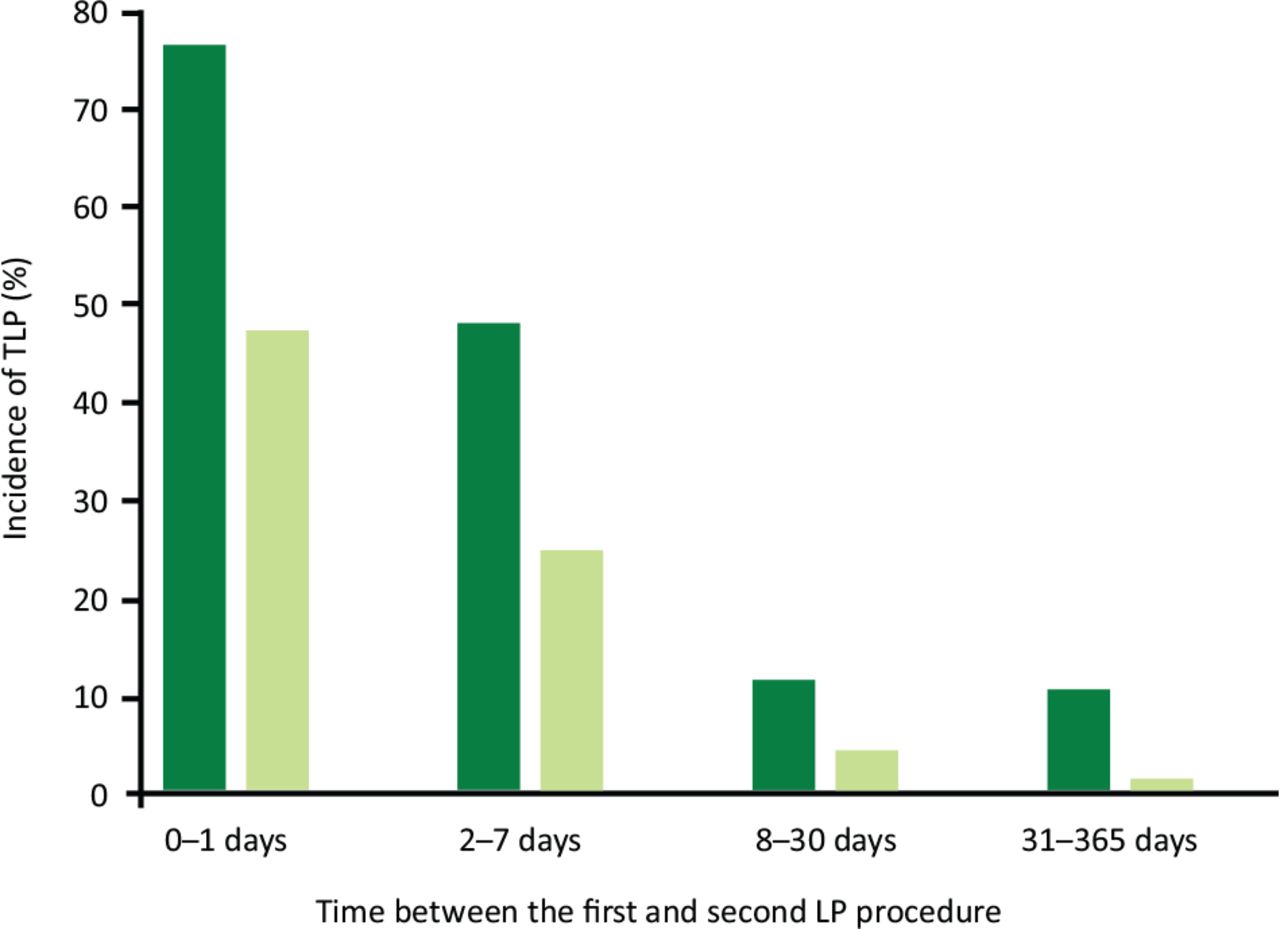
Incidence of TLP in the patient's second lumbar puncture according to criterion of ≥500 erythrocytes/μL (dark green bar) and ≥10,000 erythrocytes/ μL (light green bar) broken down by the time category between the first and second LP procedures.
Table 1 shows ORs for whether the second LP procedure was traumatic according to the criteria of ≥500 erythrocytes/μL and ≥10,000 erythrocytes/μL. The overall association of the first traumatic LP procedure with the incidence of TLP in the second procedure was significant (p<0.0001 for both criteria). If the first procedure was traumatic, the odds ratio of a TLP in the second procedure was multifold compared with a situation where the first procedure was not traumatic. A clearly blood-contaminated CSF sample in the first procedure indicated very high odds ratio of a TLP in the second procedure. The overall association of the time category with the incidence of a TLP in the second procedure was significant as well (p<0.0001 for both criteria). In concordance with Fig 4, the odds ratio of a TLP in the second procedure was at least 10-fold if the second LP procedure was performed within a day. If the successive procedure was repeated within a week, the odds ratio of a TLP was still four- or 10-fold depending on the criterion. Longer times were not significantly associated with a higher odds ratio of a TLP. The overall association of the age category with the incidence of TLPs in the second procedure did not reach statistical significance (p=0.07 for ≥500 erythrocytes/μL; p=0.12 for ≥10,000 erythrocytes/μL), but some age categories suggested twice higher odds ratios of TLPs, in line with Fig 3. Both the backward and forward logistic regression analyses confirmed the predictors and the magnitudes of their ORs and the omission of age as an independent predictor of a TLP in a patient's second procedure.
Odds ratios for predictors of traumatic second lumbar puncture procedure according to 500 red blood cells/μL and 10,000 red blood cells/μL criteria of traumatic lumbar puncture
Discussion
Besides presenting age-specific incidences of TLPs in adult LP procedures, this large retrospective study based on electronic health records examined factors that accounted for the incidence of a TLP in the second LP procedure using a pseudoprospective approach. Based on 15,800 adult LP procedures, including 2,400 successive procedures, we consistently found an at least doubled incidence of TLPs in the patients' second LP procedure compared with the first, through young adults to the oldest. Two factors accounted substantially for the higher incidence of TLPs: whether the preceding LP procedure was traumatic and whether the time between the successive procedures was short. The more blood-contaminated the preceding CSF sample, and the sooner the successive LP procedure, the more multiplied the odds of TLP. In haemato-oncology, a short time (ie a week or less) between successive LP procedures is a known risk factor of TLPs, but longer times (about 2 weeks or more) seem not to increase the risk.23–26 However, this evidence comes from haematology patients, mostly paediatric ones. Root causes of a higher odds ratio of TLP in the second procedure await further investigations but may speculatively pertain to a persistent (not fully recovered) trauma of the dura mater at the puncture site, coagulation disorders preventing or postponing proper healing of the site, or local inflammation that compromises the composition and structure of the dura mater at the time of the successive procedure.
While the young adults showed the lowest incidence of TLPs, a patient's age appeared not to be a significant independent predictor of TLPs in the second puncture. However, a consistent trend for about double odds of TLPs was seen in all age categories compared with young adults. In contrast to a higher incidence of TLPs in the oldest people reported earlier, we found an inverted U-shaped curve for the association between age and incidence of TLP.18 Especially in a patient's second LP procedure, the peak incidence took place at age around 50 to 64 years followed by a declining incidence, while in the patient's first procedure, the curve appeared flattened and reached the peak around 65 to 74 years of age. These age-related incidence patterns were similar for both criteria of TLPs, indicating robustness for the observed associations.
Based on the visual threshold of blood in CSF (≥500 erythrocytes/μL), the present 17% overall incidence of TLPs is in the middle within the reported incidences of TLPs (7%–28%) in adults.2,16–22 However, when the LP procedures were divided into a patient's first and second procedures, the respective incidences are about 14% and 35%, respectively, the latter being higher than reported in the literature. To our knowledge, this is a novel observation in adult lumbar punctures in general, other than observed in paediatric haemato-oncology.23,25 According to a similar criterion of TLP, the respective incidences in the first and second LP procedures are as low as 5% and 13% in paediatric haemato-oncology, which is most likely explained by the criticality of the LP procedure in these patients' treatment and the consequent focus on overall procedural success at the first attempt.25 Furthermore, deep sedation or general anaesthesia is generally applied, and experienced providers perform the LP procedures, especially the first diagnostic LP. In adult patients with acute leukaemia, the incidence of TLPs based on the visual threshold is about 7%.27 In routine LP procedures of adults, deep sedation and a highly experienced provider are seldom arguable alternatives, but there is much more cross-specialty variation in clinical practices and success rates, as the wide range of reported incidences of TLPs in different clinical settings indicates.2,16–22
A successful first attempt would be crucial since performing LP properly with a single skin penetration contributes to the lower incidence of TLPs in adults.16,17,26,28 A preceding TLP increases not only the probability of a TLP in the successive LP procedure but also the risk of post-dural puncture headache (PDPH).16 PDPH is among the most common complications of the LP procedure, which causes notable, post-procedural discomfort to the patient for several days, affecting from 3.5% to 33% of patients of all ages.29 Performing a successful LP procedure can be particularly challenging in patients who are substantially overweight, have spinal abnormalities or have had spinal surgery.21,26,30 While the mechanical properties of the dura mater may vary much between individuals, these properties can also alter with age and modify the haptic feedback from the tip of the spinal needle, and eventually account for the incidence of TLPs.31 For the patients' safety and comfort, one should attempt to keep the rate of complications and possible adverse events as low as possible. The smooth performance of an LP procedure may also reduce the patients' concerns about this invasive procedure and facilitate its overall performance. Success in a patient's first LP procedure strongly determines the odds ratio of a TLP in the successive procedure. If a patient's treatment or diagnostics are known to require multiple LP procedures separated by short intervals, a successful first procedure should be pursued to reduce the likelihood of a TLP in the successive procedure.
Differentiation of the life-threatening SAH would essentially benefit from CSF samples that are not misleadingly confounded by TLPs. High erythrocyte counts (>10,000 erythrocytes/μL) in CSF are associated with six-fold increase in odds ratio of SAH.15 Raised erythrocyte counts (1,000–10,000 erythrocytes/μL) in the last (3rd or 4th) vial or xanthochromia are typically considered indicators of SAH, whereas lower erythrocyte counts without xanthochromia indicate TLPs.14 Reducing erythrocyte counts in the sequence of CSF samples indicate TLPs, and a certain percentage change between the first and last sample is suggestive of a TLP.15 However, the specificity or sensitivity of this approach may not always be sufficient for diagnostic certainty, and computed tomography of the head, possibly complemented by angiographic examination, is needed.14
The main strength of this study is the large sample size comprising almost 16,000 LP procedures that were performed in two Finnish university hospitals in unselected adult patients. The dataset is, thus, considered to well-represent the general adult population undergoing LP procedures due to various clinical reasons, making the observed age-specific incidences of TLP robust and unbiased. This allowed us to establish the actual distributions of erythrocyte counts in the CSF samples collected from adults of all ages. These cumulative distribution curves comprehensively illustrate the distributions of erythrocyte counts in the CSF samples and allowed us to estimate the incidence of TLPs for any criteria of TLPs. This novel visualisation method is also a strength of this study. Another strength and novelty are the pseudoprospective analysis of relevant factors that accounted for the incidence of TLPs in successive LP procedures of the same patient. The benefit of the pseudoprospective approach over the conventional association analysis based on cross-sectional data is that virtually all patient characteristics contributing to the incidence of TLP in the first procedure are inherently regarded in the second procedure. Our data describe the whole spectrum of LP procedures performed in adults for various clinical indications.
The main limitation of this study is related to potential factors that we could not consider in statistical modelling because of the minimised, pseudonymised dataset collected retrospectively from the electronic health records for us. Potentially relevant factors include the specific indication of LP; practices concerning general anaesthesia, sedation or topical analgesics; the patients' position during the procedure; the patients' obesity / body mass index, anatomic abnormalities and consequent challenges; specific puncture site; number of attempts during the LP procedure; blood properties (eg low platelet count or coagulation pathologies); physicians' specialty and personnel's experience in performing LPs; use of image guidance; or the spinal needle type and its gauge.18–24,26,32 This specific information on patient-, physician- and procedure-related factors might have revealed some new relationships and shed further light on age-specific aetiologies of TLPs in adults. On the other hand, analysing statistically numerous explanatory variables may also reveal sporadic and relatively weak associations that may fail under scrutiny. In contrast, our study focused on a few predetermined factors (traumatic preceding procedure, time between the successive procedures and patients' age category) that could arguably be causally linked to the incidence of TLPs.
Conclusion
This retrospective study based on electronic health records yielded evidence in a large population of unselected adult patients having undergone LP procedures that the incidence of a TLP in a patient's first LP procedure was associated with age showing the lowest incidence in young adults but doubled independently of age in the subsequent procedure. Two factors, a week or shorter time between a patient's two LP procedures or a traumatic first LP, multiplied the odds ratio of a traumatic second puncture. A nontraumatic first LP procedure likely reduces diagnostic uncertainty in a patient's successive procedure. Thus, irrespective of the primary indication of LP, success in the first procedure should be pursued. If a patient's clinical situation permits and the presence of erythrocytes in the CSF sample can confound the interpretation, postponing the successive LP procedure by at least a week may be appropriate.
Summary
What is known?
Traumatic lumbar punctures, defined as blood-contaminated cerebrospinal fluid samples, are common in clinical practice.
What is the question?
Blood-contaminated cerebrospinal fluid samples can mislead a patient's diagnosis or its verification.
What was found?
Traumatic puncture is twice as frequent if the procedure is repeated.
Both a traumatic first procedure and a short time between the successive procedures multiply the odds ratio of a traumatic lumbar puncture in the latter procedure.
What is the implication for practice now?
If a patient's clinical situation permits and a high-quality sample is required, postponing the next procedure by at least a week is advised.
Conflicts of interest
Harri Sievänen and Juho Kari hold shares and are employees of Injeq Oy. This study was funded by Injeq Oy, a Finnish start-up company that manufactures bioimpedance spinal needle systems for lumbar punctures.
- © Royal College of Physicians 2023. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
{kind=link}