
ABSTRACT
‘Stage shift’ has been proposed as a marker of impact of Coronavirus 2019 (COVID-19) in lung cancer services; however, there are no data available specifically from income-deprived areas. Thus, this study evaluated the impact of the COVID-19 pandemic on lung cancer care in our area (Corby; among the most income deprived in England) and identified focus recovery areas. The study was a retrospective observational study of 668 consecutive patients with lung cancer at a district general hospital, pre-, during and after the COVID peak. Outcomes were the overall number of cases, presenting staging and treatment pathway. Overall, 32 fewer patients were diagnosed during the pandemic, with more inpatient diagnoses (p=0.01) and fewer primary care referrals (p<0.0001). There were no differences observed in treatment intent or ‘stage shift’. Our results suggest that COVID-19 negatively affected the whole lung cancer pathway in our area. However, ‘stage shift’ might not be ideal to assess the impact of COVID-19 in income-deprived areas. Further studies will help the strategic rollout of a screening programme to identify patients with lung cancer earlier on in such areas.
Introduction
In January 2020, the World Health Organization (WHO) recognised the outbreak of Coronavirus disease (COVID-19) secondary to the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) as a Public Health Emergency of International Concern. By March 2020, the outbreak of COVID-19 was recognised as a pandemic, with the first cases in the UK confirmed in the week beginning 27 January 2020.
The UK Government launched a coronavirus action plan in March 2020, with a view toward protecting the NHS from being inundated by the exponential trajectory of COVID-19 cases requiring hospital admission. Services were reallocated to maximise inpatient and intensive care capacity for COVID-19 management. Furthermore, the NHS encountered a significant crisis in staffing levels because of infection and the need for staff to self-isolate. As a result, oncological services, among others, were significantly impacted. There was reduced patient contact and an eightfold increase in the number of telephone consultations.1 Clinicians have expressed their anxieties over the negative outcomes that this might have resulted in.1 It is also estimated that ‘2-week wait’ (2WW) referrals from primary care have reduced by 80% nationwide.2
Lung cancer remains the cancer with the highest morbidity and has a significant global disease burden. Lung cancer exudes a profound impact in the UK, with national cancer registries noting an incidence of 47,838 cases diagnosed and 35,137 deaths recorded in 2018.3 Prognosis is frequently poor, which is mainly associated with late presentation.4 Therefore, early recognition is integral to more treatment options and better outcomes. Potential malignancy can be diagnosed initially following a patient's concern over their physical symptoms; this leads to further investigations and referral to specialised centres5 or via targeted screening programmes. For lung cancer, National Institute for Health and Care Excellence (NICE) guidelines advise that those with two or more unexplained symptoms (ie cough, weight loss, fatigue, breathlessness, unexplained haemoptysis and over 40 years of age) must be referred to the ‘suspected lung cancer pathway’. A chest X-ray must be carried out within 2 weeks via the 2WW system6 and patients are subsequently stratified into an urgent or non-urgent pathway. Additionally, pilot targeted lung cancer screening programmes have been launched so far in 23 income-deprived areas in England known to have poor lung cancer outcomes and late presentations, with the aim to diagnose more lung cancers early and at a curable stage, with one of those programmes being in our operational catchment area of Corby.7
The past decade saw lung cancer age-standardised incidence rates increase by 1% overall, with a 15% increase and 11% decrease in the female and male population, respectively.3 Although lung cancer age-standardised mortality rates decreased by 14% lung cancer continues to have the highest cancer-related mortality in the UK. In 2018, the 1-year survival was 83% for patients presenting with stage I disease but 17% for patients with stage IV disease. Although these statistics reflect a robust and productive national strategy, the COVID-19 pandemic has impacted facilitation of the lung cancer programme, which has inevitably paused its diagnosis of patients.
In the context of the COVID-19 pandemic, the management of lung cancer has proved arduous for several reasons. Given infection transmission fears, patients have been reluctant to present to, and convey their concerns in, a healthcare setting. Symptom similarities between the presentation of COVID-19 pneumonia and lung cancer further compound the diagnostic process. In individuals with confirmed lung cancer, the need for frequent access to healthcare facilities is common, thus exposing an at-risk population to COVID-19 infection, with previously published data showing that patients with lung cancer have poorer outcomes when infected compared with other patients.8 Oncological therapeutics further increase the susceptibility to, and severity of, COVID-19 infection. Studies have hypothesised and predicted an increase in cancer-related mortality because of obstructions caused by the COVID-19 pandemic.9 Maringe et al estimated an ∼1,235–1,372 additional deaths from lung cancer because of the pandemic.2 Furthermore, a UK Lung Cancer Coalition report recently estimated a drop of up to 5.3% in 5-year survival rates in England for patients diagnosed with lung cancer during the pandemic.10
Essential and urgent cancer services have continued through the pandemic and have had to adapt, with reallocation of resources to maintain patient safety and quality of care despite the inevitable restricted access to healthcare. Here, we present real-world findings and the experience of our secondary care lung cancer service during the pandemic in an income-deprived area, compared with the findings elicited from the preceding year.
Methods
Approval and setting
This was a single-centre, retrospective, observational study comparing two independent cohorts. The observational analysis was approved by the hospital committee as a service evaluation activity. The first cohort (pre-COVID) included all patients investigated for lung cancer before the COVID-19 pandemic, from January 2019 to December 2019. The second cohort included all patients investigated for lung cancer during the pandemic, including a period from January 2020 to December 2020. A third cohort derived from lung cancer presentations in 2021 was also reviewed, with particular emphasis on staging presentation. All components of this study were carried out at a district general hospital in the UK. All information was taken from the Somerset Cancer Register (www.somersetft.nhs.uk/somerset-cancer-register/), as well as patient electronic records and lung cancer multidisciplinary team (MDT) meeting outcomes, which are only accessible by healthcare staff involved in lung cancer patient care.
Demographics
Demographic information corresponding to age, gender, WHO performance status, source of referral and setting of first review was collated.
Outcomes
The primary outcome was a new diagnosis of lung cancer, either confirmed from histology or imaging (in cases in which the patient was not fit enough for a biopsy and/or histology would not change the management, as agreed in the lung cancer MDT meeting). Secondary outcomes included staging described as per TNM 8th edition classification and WHO staging,11 treatment intent (curative or palliative) and subsequent treatment strategy (surgery, chemotherapy, radiotherapy, chemoradiotherapy or best supportive care (BSC)).
Statistical methods
Categorical variables were expressed as frequency and percentage. Median and interquartile range (IQR; 25th–75th percentiles) was used to describe nonparametric continuous data. Mean and corresponding confidence intervals were used to describe parametric continuous data.
Comparisons between unpaired groups of parametric data were conducted with the Student's t-test, whereas nonparametric data unpaired comparisons were conducted with the Mann–Whitney U test. Categorical variables were compared with the use of the Chi squared test. p <0.05 was considered statistically significant.
Statistical analyses were conducted with the use of GraphPad Prism 8 (GraphPad Software, Inc., CA, USA).
Results
Primary outcome
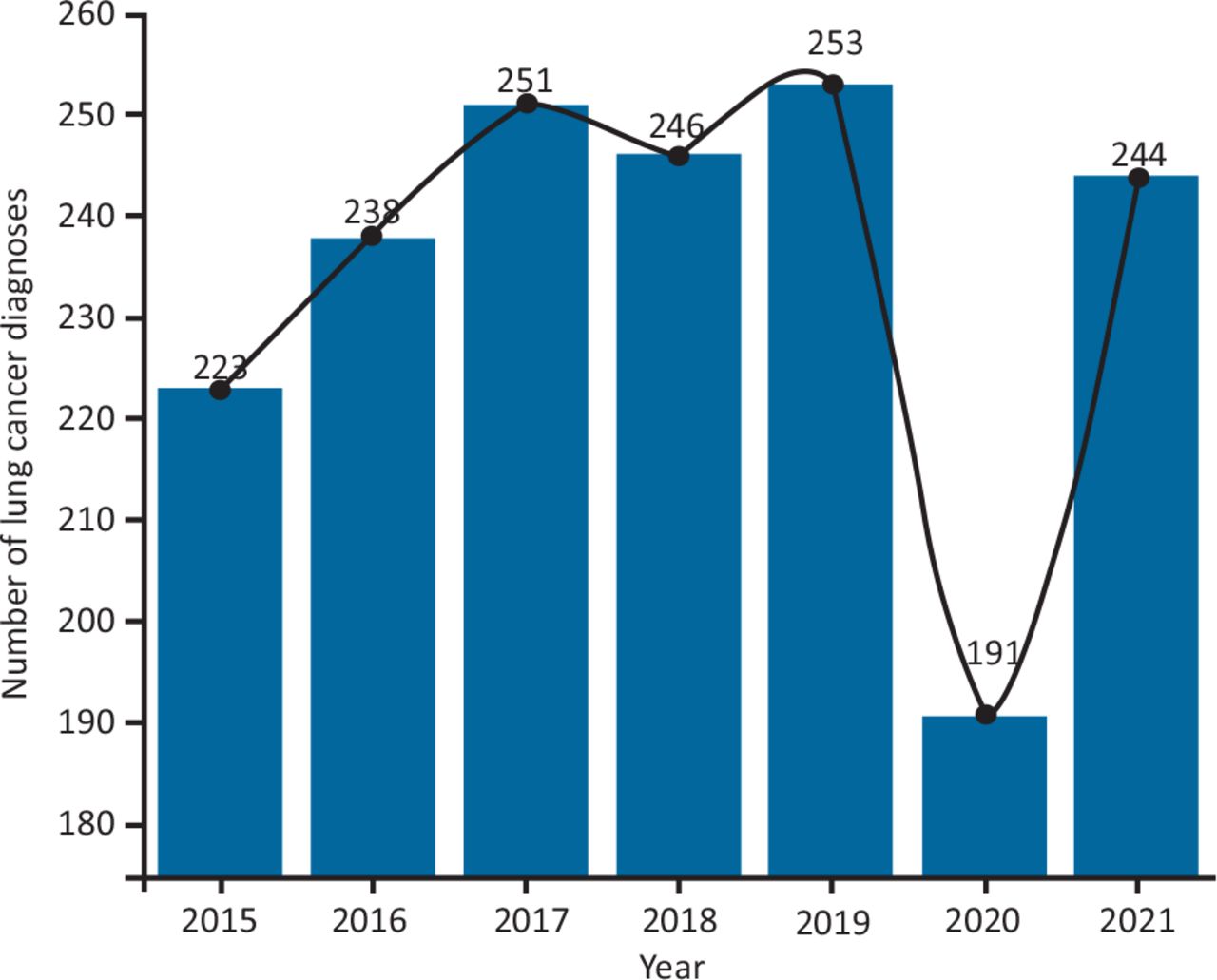
There were 228 new lung cancer diagnoses in the pre-COVID group, and 196 in the group diagnosed during the COVID-19 pandemic. Overall, the year 2020 observed a total of only 191 new lung cancer diagnoses, compared with 253 and 246 new cases in the years 2019 and 2018, respectively (Fig 1), whereas the year 2021 saw 244 new cases. The clinical characteristics of the patients are detailed in Table 1. The median age (IQR) of the pre-pandemic group and the group during the pandemic was 73 years (65–81) and 75 years (68–82), respectively (52% and 48% were male, respectively). Non-small cell lung cancer (NSCLC) adenocarcinoma was the most frequently observed histology in both groups (p=0.41) (Table 2) (Fig 2c). There were more cases of NSCLC squamous cell lung cancer diagnosed in the pre-COVID group (27.8%) compared with during the COVID-19 pandemic (12.4%; p=0.0001). Both groups exhibited a similar number of confirmed small cell lung cancer (SCLC) cases.

Number of lung cancer diagnoses over the past 7 years.
Patient demographics, source of referral and setting of first review
Histology and staging of patients with lung cancer at presentation before, during and after the COVID-19 pandemic
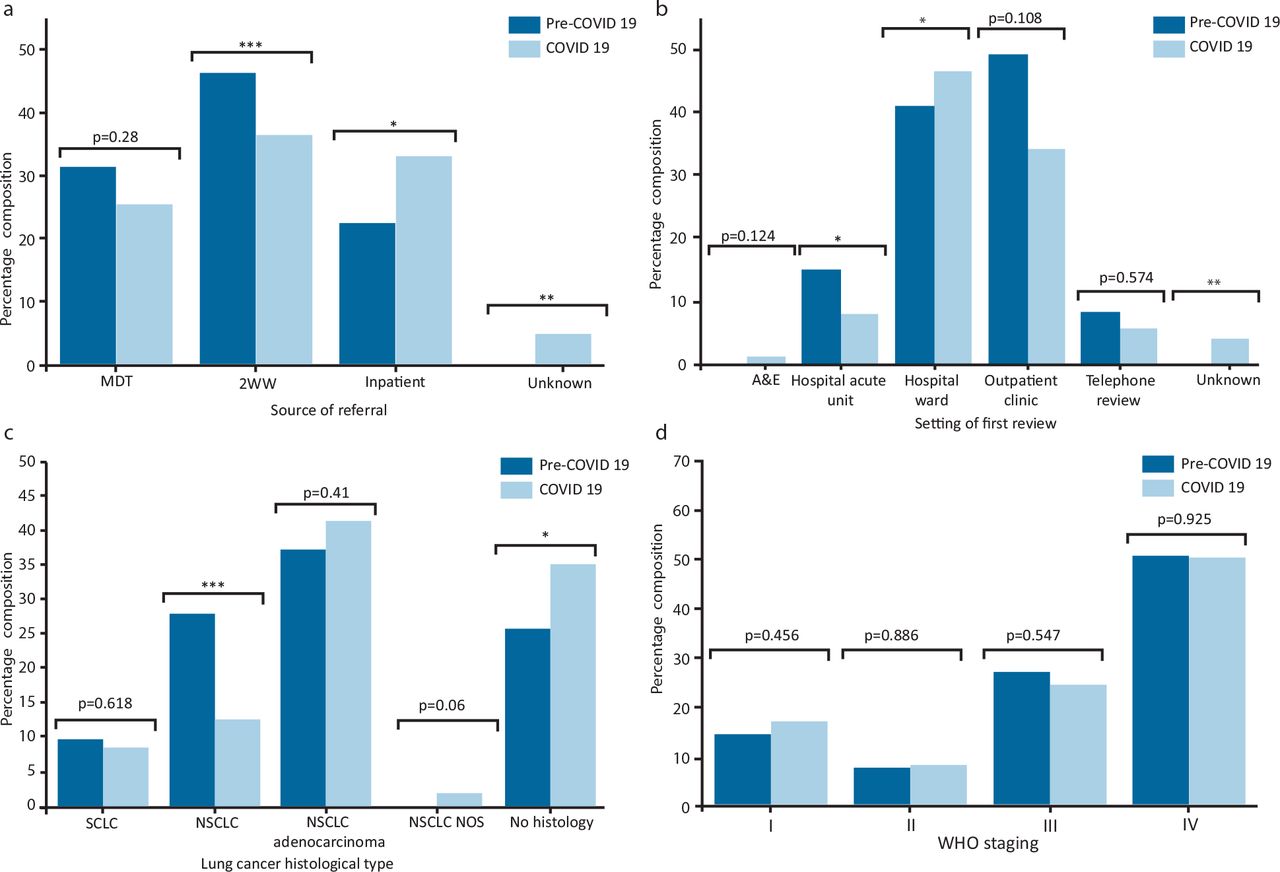
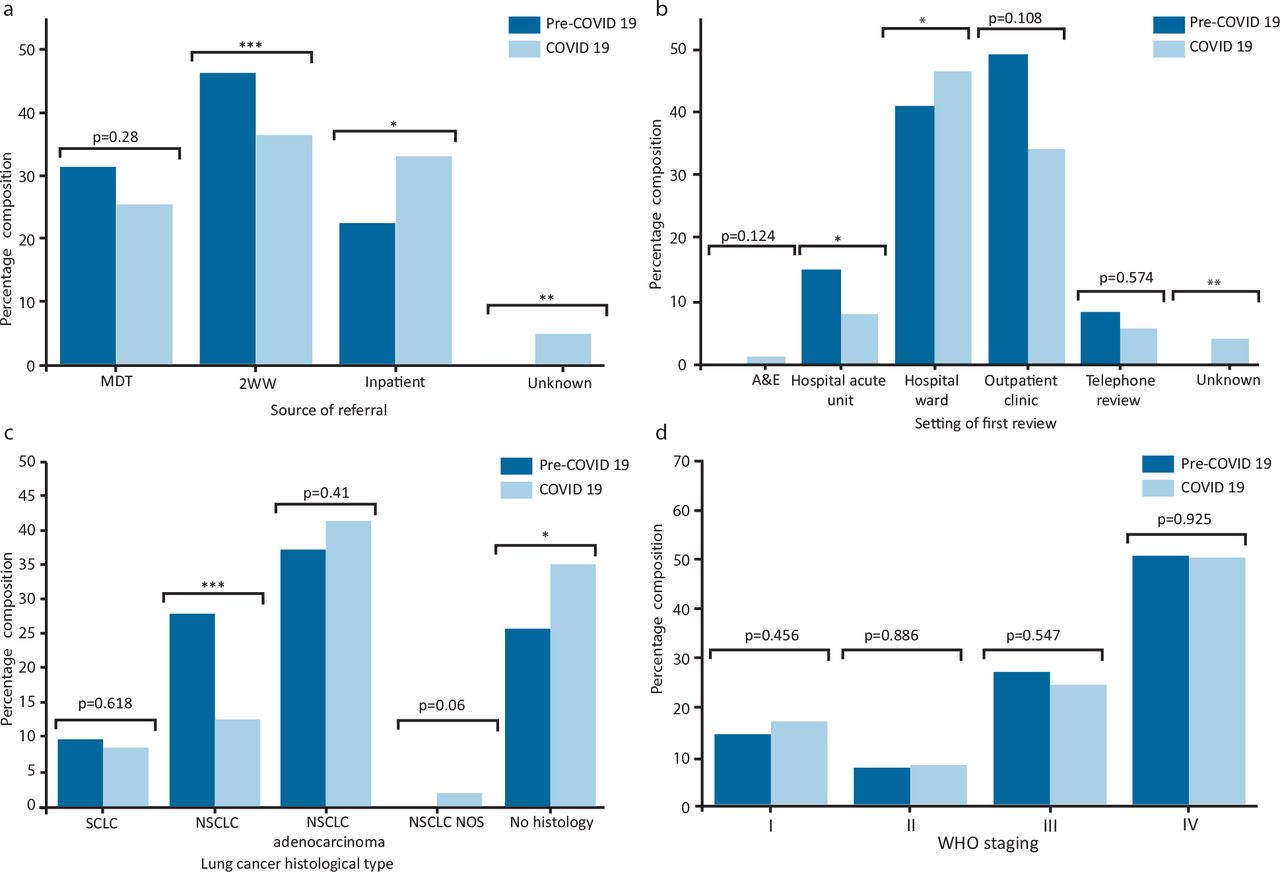
Comparison of (a) source of referrals, (b) setting of first review, (c) lung cancer histological type, and (d) World Health Organization (WHO) staging during the pre-Coronavirus 2019 (COVID-19) versus COVID-19 time period. *p<0.05; **p<0.005; ***p<0.0005. 2WW = 2-week wait; A&E = accident and emergency; MDT = multidisciplinary team; NOS = not otherwise specified; NSCLC = non-small cell lung cancer; SCLC = small cell lung cancer.
Secondary outcomes
The 2WW referral pathway was the main source of referrals for the pre-COVID group (46.3%) (p<0.0001) (Fig 2a). There was an increase in the proportion of referrals from inpatient admissions during the COVID-19 pandemic (33.2%) compared with pre-pandemic (22.4%) (p=0.01).
The most frequent setting for the first clinical review during the COVID-19 pandemic was inpatient hospital wards and admission units/emergency care (46.6%) compared with the pre-COVID group (40.9%) (p=0.01) (Fig 2b). Significantly fewer patients were reviewed for the first time in an outpatient clinic setting (34.2%), in contrast to the preceding year (49.2%) (p=0.108).
Interestingly, both groups observed similar staging distributions at presentation (Table 3). T4 disease was noted in 43.9% and 41.7% of cases pre-COVID and during the pandemic, respectively. This was also consistent with the 2021 cohort, exhibiting a T4 disease prevalence of 42.6%. A greater burden of advanced lymph node involvement (N3) was seen in the pre-COVID group compared with the group during the COVID-19 pandemic (25%) (p=0.008). A comparable frequency of M1 disease was observed in all three groups (53.3% pre, 50% during and 50.8% after the pandemic). With respect to WHO staging, all three groups demonstrated an almost-identical prevalence of stage IV disease at the time of diagnosis, in ∼50% of the respective cohorts (p=0.893) (Fig 2d).
Treatment approach to lung cancer before, during and after the COVID-19 pandemic
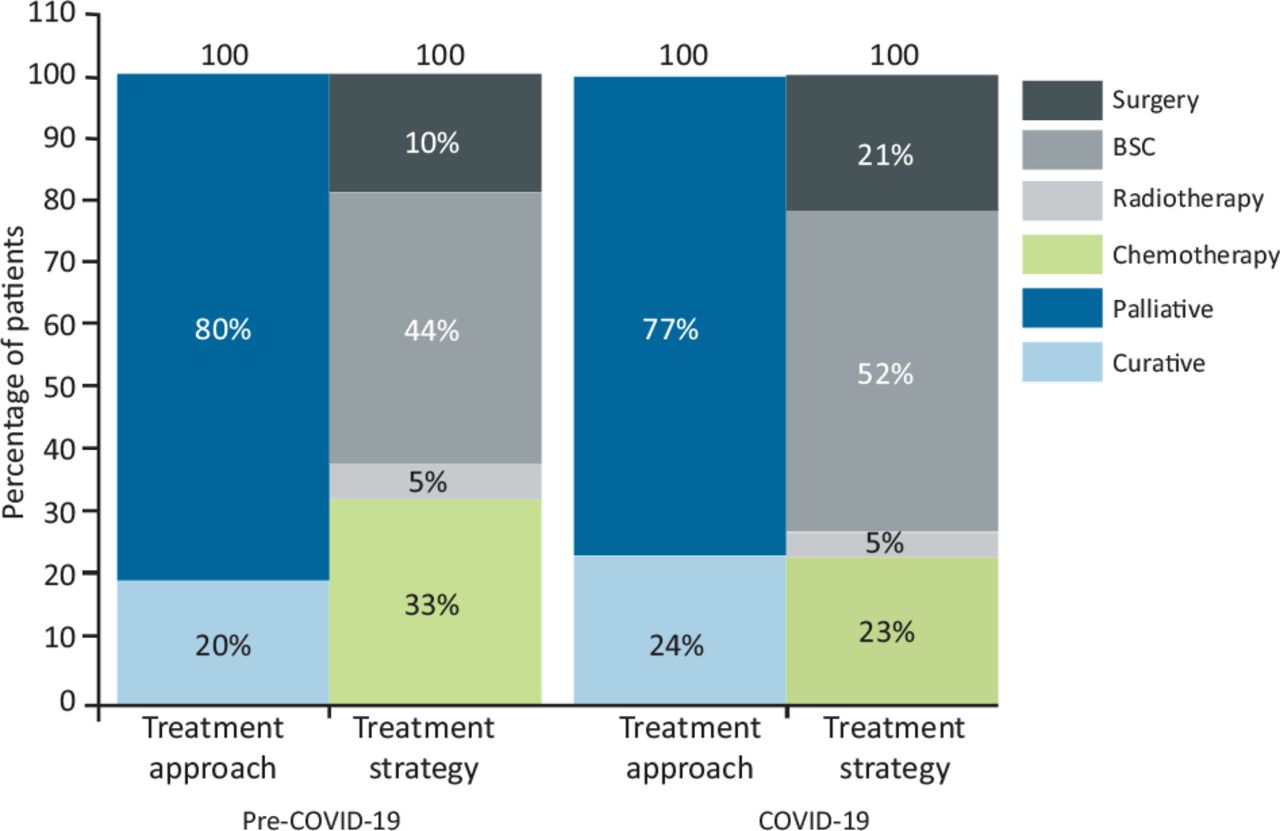
The palliative treatment approach was used significantly both pre-COVID (80.2%) and during the pandemic (76.5%) (p=0.351) (Table 3) (Fig 3). Initiation of chemotherapy during the COVID-19 pandemic decreased (23%) compared with pre-COVID-19 (32.9%) (p=0.02), and a similar trend was also observed for radiotherapy (p=0.08). Interestingly, in contrast to national data, there was an increase in surgical intervention during the pandemic in our cohort (20.9%) compared with the pre-pandemic cohort (18%) (p=0.0445). Unfortunately, BSC was common in both cohorts (43.9% pre-pandemic and 51.5% during, p=0.115).

Lung cancer treatment approach and strategy. BSC = best supportive care; COVID-19 = Coronavirus 2019.
Discussion
The two groups demonstrated comparable demographic characteristics with respect to age, gender and WHO performance status. The lung cancer services experienced a substantial surge in the source of referrals from inpatient healthcare teams, whereas a reduction in the use of the 2WW pathway was observed. These findings might not be surprising given the considerable impact of the COVID-19 pandemic. Although strict measures taken by the UK Government saw positive effects with respect to controlling the dissemination of the COVID-19 infection, they might have had a deleterious impact on the diagnostic pathways of significant medical conditions. Protocols, including postponement and triaging of clinical visits as per their presumed severity, have the propensity to result in missed diagnoses or clinical suspicion. Public fears of COVID-19 transmission further accentuate this, because patients with symptoms might express reluctance to enter healthcare settings. Various studies have published findings indicating a reduction in the incidence of malignancies since the start of the pandemic and subsequent lockdown.12–16 The reduction in referrals from the primary care setting has led to significant concerns of delayed presentations potentially leading to further advanced disease and negative outcomes. Furthermore, Ellis-Brookes et al described how the late presentation of cancer can lead to a late diagnosis and, thus, lower survival rates in the first year after diagnosis.4
Lai et al predicted substantial mortality for patients with malignancy because of the impediments in the cancer pathway.9 With respect to the increase in inpatient referrals, the pandemic led to an increase in inpatient admissions owing to considerable respiratory compromise and appreciable virulence of the COVID-19 infection. As a result of the frequent use of cross-sectional imaging, pulmonary malignancies might also be detected. Another consideration is the severity of COVID-19 infections in patients with a concomitant lung cancer, because this cohort is at risk of higher morbidity and mortality and, thus, is more likely to be admitted to hospital. The Thoracic Cancers International COVID-19 Collaboration (TERAVOLT) registry indicated that 76% of patients with lung cancer and a COVID-19 infection required admission to hospital.17 Furthermore, some patients might have undiagnosed lung cancers that increase their susceptibility and severity of a COVID-19 infection.18,19
The most frequent setting of initial reviews during the COVID-19 pandemic was on inpatient wards, as expected, in contrast to the outpatient clinic settings observed during the previous year. A systematic review conducted by Riera et al identified factors contributing to delays and disruptions to cancer healthcare during the pandemic. Provider/system-related explanations included COVID-19 risk reduction strategies, personnel shortages and concerns regarding service availability.20 Ranganathan et al published findings from a cohort study further evaluating the disruption to healthcare services and reported a 54% reduction in the number of new patients registered with cancer centres along with a 46% reduction in follow-up visits.21 Naidich et al reported a decrease in the volume of outpatient imaging in 2020 (327,738 examinations) compared with 2019 (440,314 examinations).22 Unfortunately, because of inherent limitations of the study acknowledged by the authors, specific details categorised by individual imaging modalities were not ascertained. Despite the aforementioned challenges in outpatient service availability, national healthcare organisations strived to maintain cancer diagnostic services at an optimal level right from the start of the pandemic.
With respect to staging, there were few discrepancies in the WHO and TNM distributions across the three groups. TNM M1 and WHO stage IV were at ∼50% across all groups. This is particularly relevant, because these findings potentially testify to the efficacy of the protocols implemented in cancer services during the pandemic. The prominent concerns during the initial stages of the pandemic were delayed diagnoses and potentially advanced progression at later presentation; however, these findings indicate that primary care and cancer services adapted to the logistical impediments of the pandemic and determined diagnostic strategies to enable them to perform at a similar level to the pre-pandemic period. Another possible explanation could be the previously known numbers of ‘late presenters’ in our area of interest. In the NHS Long Term Plan,23 late presentation associated with an advanced stage of lung cancer can reach 50% of cases, whereas, in our area, this number was closer to 75%, and has been associated with income deprivation and lack of patient engagement with healthcare services. Unfortunately, these confounders have remained unchanged during the pandemic and it is likely those ‘late presenters’ in our area would not engage early even if there was no pandemic. This highlights two important points. First, looking to identify a potential ‘stage shift’ as a sole indicator to assess the impact of the pandemic in similarly income-deprived areas might be inappropriate, because it does not reflect the entirety of the challenges and access issues that this population faces, even during non-pandemic times, which affects treatment pathways and subsequently outcomes.24 Second, because of the above, it is now evident that a targeted national lung cancer screening programme is a necessity to significantly reduce access inequalities in such areas.
Treatment approaches exhibited similarities across the groups, with a palliative approach being the more prevalent strategy, likely because of a large proportion of the patients presenting with metastatic disease. Chemotherapy and radiotherapy were used less, although a few patients during the COVID-19 pandemic started treatment with chemoradiotherapy. This was initially thought to be because of reduced access to curative surgery; however, in our analysis, there was an increase in surgery during the pandemic. Research has indicated that, with proper precautionary measures, a high volume of surgeries can be safely carried out even in a pandemic.25 However, it important to consider the current burden on intensive care units because highly invasive and complex thoracic surgery might necessitate a period of intensive monitoring during recovery.
Although some of the findings of the study are reassuring, we acknowledge that there are several limitations given its retrospective observational nature and because it was a single-centre analysis. Certain demographic information would have not been initially collated and, thus, unknown confounders will be present. Furthermore, matching between groups was not carried out, although baseline demographics were comparable. Stratification into homogenous subgroups was not conducted because of concerns of reduced power to detect effect change. Performance bias will be inevitably present given the difficulties associated with the pandemic that would have made a standardised exposure/process across the three groups unfeasible. Information bias is also inherent in retrospective studies, although the outcome variables were all collated in the same way. Furthermore, there is limited generalisability of the results, because the data were collated from a single centre. However, other income-deprived areas in England experience the same challenges in lung cancer care and, thus, it would be interesting to know the experiences and outcomes of other centres serving similar populations.
One would argue that, to strengthen our findings further, we must also provide survival data. Given that most of our patients from the group diagnosed during COVID-19 are still receiving treatment, such data are not currently available and will be collected as they become available.
Our study is the first to report real-world data specifically from an income-deprived area in England regarding the true effect of COVID-19 on lung cancer diagnosis, staging and treatment. Although small and retrospective, it provides a strong signal that COVID-19 has negatively affected lung cancer care in this income-deprived area, highlighting the need for not only cancer recovery plans in similar areas, but, more importantly, also a nationwide lung cancer screening programme.
Conclusion
In our catchment population of an income-deprived area, there were overall fewer diagnoses of new lung cancers and a significant reduction in referrals via the 2WW pathway (in line with national data). At the same time, inpatient ‘first diagnosis’ of lung cancer was significantly more frequent during COVID-19. More importantly, there was neither a significant ‘stage shift’ observed nor differences in WHO performance status at diagnosis between the pre- and during COVID-19 groups.24 Although single-centre and retrospective with the accepted weaknesses, our study suggests that, in income-deprived areas, looking at ‘stage shift’ alone to assess the pandemic impact might not be as accurate as other approaches, because it does not reflect the entirety of the challenges and access inequalities that this population faces. Additional local data collection and analysis from similarly income-deprived areas would guide future healthcare strategies to increase public awareness and engagement with healthcare services, identify more intricate reasons for ‘late presentation’ and support the rollout of a national lung cancer screening programme.
Data sharing
Anonymised data can be made available on request.
Summary
What is known?
The COVID-19 pandemic has had a significant impact on NHS resources and services and augmented late presentations. Lung cancer care has experienced delays, with the clinical community predicting poor outcomes. A national lung cancer screening programme is currently in a public consultation phase.
What is the question?
What has been the impact of the COVID 19 pandemic on lung cancer care and service recovery in an income-deprived area in England?
What was found?
The local impact of the pandemic in new lung cancer diagnoses specifically in income-deprived areas has not been well documented. Staging at presentation might not be a true reflection of negative impact, especially in deprived areas, where late presentation is the norm. Herein, our real-world data from an income-deprived area show that delay of first presentation was more prominent than in other areas in England, leading to an excess of first diagnoses taking place during inpatient care, whereas staging at presentation did not differ in relation to the pandemic.
What is the implication for practice now?
This study will hopefully inform further research and evaluation into lung cancer burden and services specifically in similarly income-deprived areas in England. We highlight the fact that looking at ‘stage shift’ alone in such areas should not be used as a sole indicator, because it does not reflect the entirety of the access challenges. There is vital need for a national rollout of a lung cancer screening programme to help reduce in inequalities in lung cancer detection.
Acknowledgement
We thank the staff of the NHS for their hard work in running lung cancer services during the COVID-19 pandemic.
- © Royal College of Physicians 2023. All rights reserved.
References








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.