
ABSTRACT
The use of cancer immunotherapies such as immune checkpoint inhibitors (ICIs) has been a paradigm shift in harnessing the immune system to act against cancer cells, and transformed the treatment of several solid and haematological malignancies. Cancer immunotherapies have a unique toxicity profile dependent on their mechanism of action, related to upregulation of immune activity. These can be severe and lead to life-threatening organ toxicity, and therefore identification of at-risk patient groups, early detection and prompt initiation of steroids and other immune-modulating agents is imperative. Acute presentations with toxicity related to these agents comprise a significant proportion of primary and secondary care presentations related to treatment toxicity in oncology. This article will focus on the diagnosis and management of common toxicities associated with immune checkpoint inhibitors, the most commonly utilised cancer immunotherapies.
Key points
Immune checkpoint inhibitors release a natural brake on the immune system, which leads to increased T-lymphocyte activity.
These effects have proven beneficial in several common advanced malignancies including metastatic melanoma, lung cancer and renal cancer.
A unique set of immune-related adverse events are associated with ICIs, and broadly can be considered as immune-mediated inflammation of any organ system.
Awareness of immune-related toxicity is important in the primary and secondary care setting.
Early diagnosis of toxicity and prompt initiation of systemic immunosuppression with steroids and other agents is necessary to reduce the risk of progression to more severe and potentially life-threatening organ toxicity.
Immune checkpoint inhibitors
Immune checkpoint inhibitors (ICIs) release a natural brake on the immune system, inhibiting the interaction of programmed death (PD)-1 on T lymphocytes and its ligand, PD-L1 on antigen presenting cells, including tumour cells. Another important checkpoint protein that can be targeted in this way is cytotoxic T lymphocyte antigen (CTLA)-4.1 Inhibition of activity at immune checkpoints leads to increased T lymphocyte and associated immune activity, conferring an anti-tumour response in some cancers. A unique set of immune-related adverse events are associated with ICIs, and broadly can be considered as immune-mediated toxicity and inflammation of any organ system.2
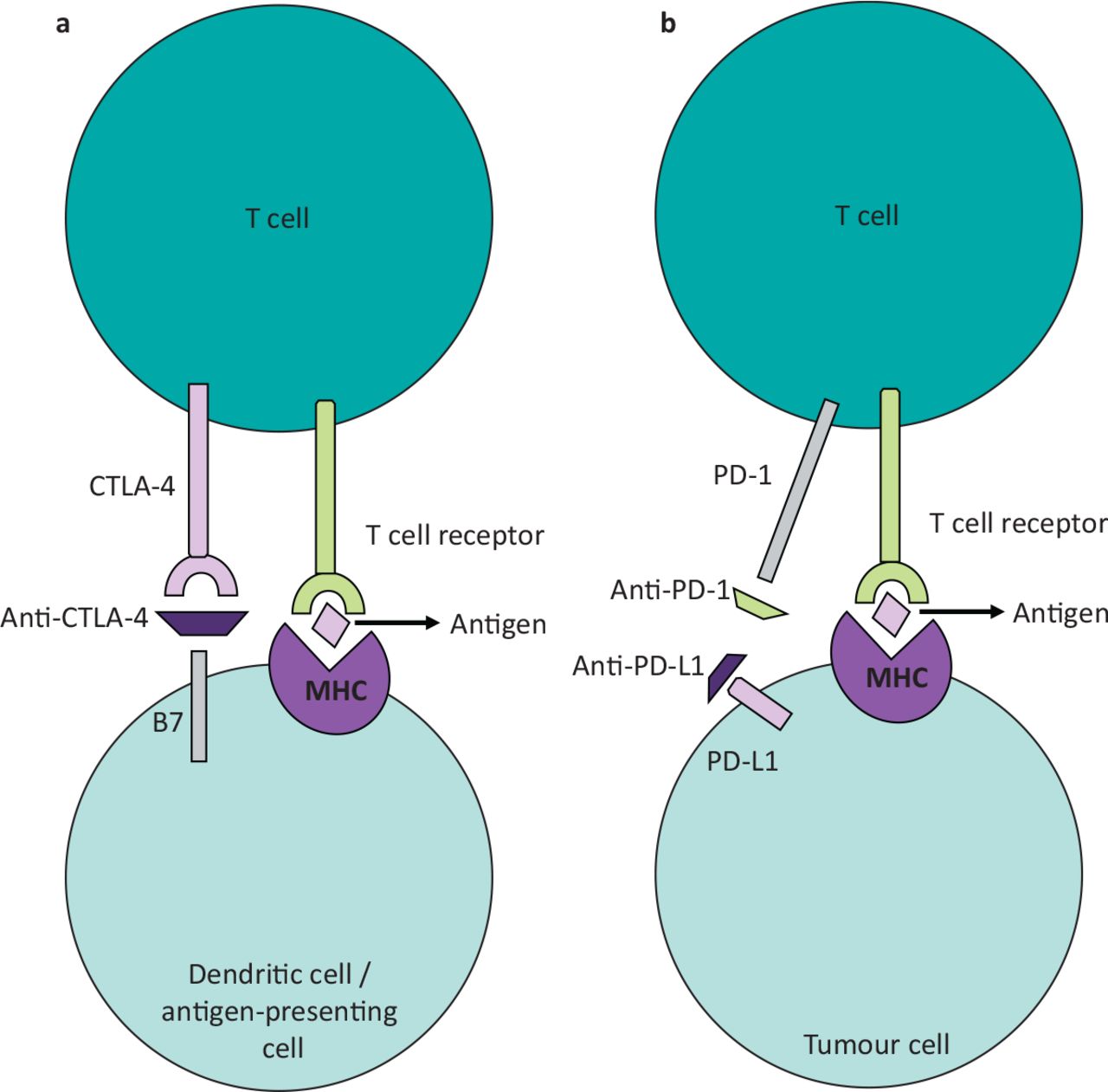
Important ICIs to be aware of are listed in Box 1 and their mechanism of action shown in Fig 1.

Immune checkpoint inhibitors in tumour immunology: mechanism of action. (a) Anti-CTLA-4 antibodies such as ipilimumab block the interaction between CTLA-4 on T-cells and B7 on dendritic cells and other antigen presenting cells, leading to up-regulation of immune activity. (b) PD-1 is expressed on activated T cells; its interaction with PD-L1 expressed by cancer cells causes a reduction in T-cell activity. Blockage of this interaction by an anti-PD-1 or anti-PD-L1 checkpoint inhibitor leads to up-regulation of T-cell activity that can have an anti-cancer effect.
Important immune checkpoint inhibitors
Immune-related adverse events (irAEs) typically occur within 3 months of commencement of ICIs, but can appear later.2 Prior to starting ICIs, risk factors for irAEs should be identified, for example autoimmune disease or previous toxicity. Given the diversity of possible irAEs, initial assessment of any toxicity should involve grading, investigation to assess the toxicity and consider possible differential diagnoses, identification of risk factors for immunosuppression, and finally consideration of first-line immunosuppressive agents. Multidisciplinary specialist involvement for further assessment and escalation of therapy may be required.
irAEs are graded using the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0, which is readily available to all clinicians.3 Early grading following presentation with a suspected irAE is imperative, as consensus guidelines on management are based on this assessment of severity.
Corticosteroids are the recommended first line systemic approach to management of irAEs graded 2 and above. A broad range of steroid-sparing agents are used in severe and refractory cases, include conventional disease-modifying anti-rheumatic drugs (DMARDs) such as mycophenolate and azathioprine, and biologic DMARDs such as infliximab. Other agents such as intravenous immune globulin (IVIG) are recommended in specific cases. Second- and later-line immunosuppressive therapies should only be used with input from the treating oncologist and relevant medical specialist for the organ system involved. irAEs can be slow to resolve and robust follow-up and frequent interval assessment is required in all cases.
The European Society of Medical Oncology (ESMO) publishes detailed and regularly updated guidelines on the management of irAEs, with organ-specific guidance based on severity of the observed toxicity, and on which the following summaries are based.2
Skin toxicity
Clinical presentation
ICI-related skin toxicities are the most commonly reported irAEs and can present as non-specific or as more characteristic autoimmune cutaneous presentations.4 Most commonly observed is a maculopapular rash with or without pruritis. Skin toxicity represents more than 50% of all observed irAEs and tends to occur in the weeks after initiation of ICI.4
Examples of other presentations include psoriatic rash, bullous presentations, erythroderma and rarer severe skin toxicities such as Stevens-Johnson syndrome, drug reaction with eosinophilia and systemic syndrome (DRESS), toxic necrolysis and cutaneous vasculitis.
Diagnosis
Clinical assessment, including a robust history which notes the onset of skin changes/rash in relation to ICI administration in addition to examination of clinical signs, is sufficient for initiation of treatment in suspected cases. This should be supported by referral to dermatology for further assessment and skin biopsy.
In cases of ICI-related maculopapular rash, pathological examination usually demonstrates lymphocytic infiltration, oedema and presence of eosinophils. Lymphocytic infiltration and other evidence of immune-mediated changes are evident in other specific autoimmune-like presentations.
Management2
For grade 1 cases of ICI-related maculopapular rash, the ICI can most likely be continued and toxicity managed with topical steroids, oral antihistamines and topical emollients, alongside suitable investigations to rule out other aetiologies. In grade 2 cases, temporary interruption to ICI therapy should be considered, alongside initiation of higher potency topical steroids, supportive medications and consideration of systemic steroids in refractory cases. Grade 3 cases will involve a rash covering >30% of body surface area, and at least moderate symptoms. Alongside topical and supportive medications, these cases will likely require initiation of oral prednisolone at 0.5–1 mg/kg.
For CTCAE grade 4 cases, hospital admission is required. Both the cutaneous presentation and secondary systemic upset is severe and potentially life-threatening. Intravenous methylprednisolone at 1–2 mg/kg should be initiated in this situation.
Once commenced, steroid therapy should generally be tapered slowly over >4 weeks if improvement is observed. Early involvement of dermatology in grade 3 and above cases and all those requiring hospital admission helps to facilitate early consideration of second line agents in steroid-refractory toxicity, with examples including ciclosporin, infliximab and tocilizumab.
In severe or refractory cases, permanent discontinuation of the ICI will be considered by the oncology MDT.
Table 1 gives examples of topical steroids by potency.
Examples of topical steroids by potency
Lung toxicity
Clinical presentation
Immune-related interstitial lung disease (ILD)/pneumonitis has an incidence of <5% for all subgroups of ICI therapy, but can be life-threatening.5 Presentation may be with or without symptoms, as radiological early grade pneumonitis with only evidence of changes on CT is recognised. Common symptoms include dyspnoea, cough, chest pain and fever, with symptoms often worse on exertion.
Diagnosis
Dyspnoea and cough should trigger comprehensive work-up in oncology patients receiving ICI therapy and includes CT imaging which may demonstrate pneumonitic changes (although these can be absent early in the disease course), bloods, pulse oximetry, screening for atypical infections and consideration of cardiac pathology. Bronchoscopy and pulmonary function tests often form part of the work-up in grade 2 or higher cases.6
Management
Management is according to CTCAE grade. Grade 1 and 2 cases can be managed in the outpatient setting with cessation of ICI therapy and oral corticosteroids. Grade 3 and above cases of ICI-associated pneumonitis will require hospital admission and treatment with IV methylprednisolone 1–2 mg/kg OD in the first instance. Antibiotic therapy for concurrent infection should be considered in all cases and given to patients receiving IV steroid therapy in hospital. Tocilizumab and mycophenalate are used in severe or refractory cases.2
Gastrointestinal toxicity
Clinical presentation
ICI-associated enterocolitis and microscopic colitis are recognised as distinct clinical syndromes with different histological patterns of immune-related inflammation, with ICI-associated enterocolitis being the most common form of recognised gastrointestinal toxicity. Incidences of any grade diarrhoea with ICI treatment is above 30% and more commonly observed with combination immunotherapy treatments.7
Diarrhoea, abdominal pain and PR bleeding are the most common presenting symptoms. Additional important symptoms to note are a persistent change in bowel habit, fever, nausea and vomiting. Patients can present acutely with severe colitis, where there is a risk of systemic sepsis, colonic perforation and fistulation. Monitoring and diagnosis of early grade gut toxicity is imperative to reduce the proportion of higher-grade presentations.8
Diagnosis
Clinical and radiological signs of colitis, in addition to non-specific markers of gut inflammation, can be sufficient to support initiation of management in the acute setting. However, early involvement of gastroenterology to facilitate colonoscopy and luminal biopsy to identify characteristic features is recommended in any grade >1 diarrhoea.
Management
Management is again according to grade. Stool cultures, calprotectin and additional tests such as a CMV PCR can be useful to confirm the diagnosis and exclude important differentials. Grade 1 ICI-related diarrhoea can be monitored with treatment continuation, low fibre diet and oral anti-diarrhoeal agents such as loperamide. Cases of grade 2 toxicity can be managed with oral steroids, with immunosuppressive agents such as infliximab reserved for refractory cases.
Grade 3 and above cases will require hospitalisation, immediate commencement of IV methylprednisolone at 1–2 mg/kg alongside general supportive measures of acute colitis (such as bowel rest, IV rehydration, nutritional support and monitoring for acute/severe colitis). Involvement of multidisciplinary specialist teams such as a dietician, gastroenterology and general surgery is imperative, as is early re-assessment of steroid refractory disease and initiation of second-line infliximab.2
Endocrinopathies
Immune-related endocrinopathies are a common occurrence in patients receiving ICI therapy. These tend to persist after completion/cessation of ICI therapy. Endocrine dysfunction rarely necessitates cession of treatment, and the requirement for high dose steroid therapy is also unusual.
Routine thyroid function and 9 am cortisol tests are carried out in the outpatient setting for all patients receiving ICI therapy. The commonest immunotherapy related endocrinopathies are thyroid dysfunction (hypothyroidism more commonly than hyperthyroidism), hypophysitis, diabetes and adrenal insufficiency. Immune-related hypogonadism, parathyroid dysfunction, Cushing syndrome and diabetes insipidus are rarer but have also been described.9
Important recommendations2
Immune-related hypothyroidism should be treated, particularly in symptomatic cases, with levothyroxine 50–100 micrograms/day and titrated until normalisation of the TSH.
Grade 3 and above immune-related hypophysitis can present with characteristic neurological symptoms and will often require hospitalisation and IV steroid therapy.
Adrenal crisis is an important differential diagnosis to consider in patients who have received ICI therapy and present as systemically unwell, with electrolyte disturbance and/or with significant fatigue and dizziness.
In low grade or asymptomatic primary adrenal insufficiency, steroid replacement should be initiated and titrated according to response. A short Synacthen test is required to support diagnosis.
The recognition of diabetic ketoacidosis as a presenting complaint or complication of immune-related diabetes is important in the acute setting.
As with all ICI toxicity, treatment cessation must be considered in grade 3 and above toxicity and refractory toxicity.
Other
Cardiovascular toxicities
A diverse range of potential cardiovascular toxicities associated with ICI therapy includes myocarditis, acute coronary syndrome, arrhythmias and non-inflammatory heart failure. Risk factors include prior cardiovascular disease, chronic diseases such as kidney disease, diabetes and autoimmune conditions, as well as concurrent use of other cardiotoxic agents.10 Serial troponin measurement, ECG, echocardiography and cardiac MRI can aid diagnosis and monitoring of response to immunosuppressive therapy.11
Hepatotoxicity
Between 1 and 2% of grade 3 ICI-associated toxicity is accounted for by hepatitis.12 Routine monitoring of liver function enables early diagnosis of ICI-associated hepatotoxicity. Management is according to grade, systemic treatment is necessitated in grade 3 and above toxicity, and should be considered in grade 2. Steroids are recommended first line, with second-line agents including mycophenalate, tocilizumab, azathioprine and tacrolimus. Of note pancreatic toxicity and cholangitis are recognised as distinct categories of ICI-related toxicity.2
Haematological toxicity
ICI-related haematological toxicity and associated myelosuppression is relatively rare, observed in <5% of patients treated with these agents, and can present with grade 3 or higher/life-threatening toxicity.2 Presentations can be varied and include cytopaenias and more specific immune-mediated toxicities such as autoimmune haemolytic anaemias, haemolytic uraemic syndrome and thrombotic thrombocytopaenic purpura. Investigation guided by a haematologist is important and will include blood film analysis and early consideration of a bone marrow biopsy. Treatment paradigms are as for other immune-related adverse events.
Neurological and rheumatological toxicities
These are important broad categories of ICI toxicity, with a diverse range of potential presentations. It is important to be familiar with the more common of these including arthralgia, myalgia, myositis, meningitis and encephalitis and suspect ICI-related toxicity in all patients receiving treatment who present acutely with neurological or rheumatological phenomena.1,2,13
Conclusions
ICIs are associated with a diverse range of immune-related toxicities that can range from mild to severe and life-threatening. Management is both organ-specific and according to grade, with corticosteroids forming the mainstay of first-line systemic treatment. Early involvement of a specialist multidisciplinary team is important to facilitate escalation to second line therapy in severe and refractory cases. Awareness of the diversity of immune-related AEs associated with ICIs that can present to primary and secondary care is important to promote early diagnosis ad appropriate management of these complex conditions.
- © Royal College of Physicians 2023. All rights reserved.








{kind=link}