
ABSTRACT
Benign metastasising leiomyomatosis (BML) is a rare disease, predominantly seen in premenopausal women. It poses a diagnostic dilemma and can be misdiagnosed as malignancy. Here we present a case of 41-year-old woman with a previous history of hysterectomy 10 years ago for multiple fibroids. She presented with shortness of breath and chest discomfort. Chest X-ray showed pulmonary infiltrates. She was diagnosed with sarcoidosis and treated with steroids without any improvement. Further investigations including CT scan and bronchoscopy and lavage failed to confirm a diagnosis. Subsequently she underwent video-assisted thoracoscopic surgery and histopathology revealed leiomyomatosis (so-called leiomyomatous hamartomas/benign metastasising leiomyomatosis). Oestrogen and progesterone receptors showed diffuse and strong nuclear staining. The patient was commenced on tamoxifen and a repeat chest X-ray in 8 weeks showed significant improvement. In women of reproductive age with previous hysterectomy and multiple lung nodules on imaging, the diagnosis of BML should be taken into consideration.
Introduction
Benign metastasising leiomyomatosis (BML) is a rare disease characterised by solitary or multiple smooth muscle tumours at distant sites. It usually occurs in premenopausal women with prior history of hysterectomy for benign leiomyomas. BML poses a diagnostic dilemma as many patients are misdiagnosed initially with malignancy of unknown origin.1 Hence a detailed medical history, clinical examination, imaging studies, biopsy of tumour and multidisciplinary approach is vital for the diagnosis. Treatment options include observation in asymptomatic patients, surgery or antioestrogen therapy. In this article, we report a rare case of pulmonary BML presenting with a long-standing history of breathlessness and chest discomfort.
Case presentation
A 41-year-old premenopausal woman, previously healthy, presented to the pulmonology department with a 2-year history of shortness of breath associated with intermittent chest discomfort. She denied any fever, cough, weight loss or night sweats. Her past medical history included hysterectomy 10 years ago due to multiple uterine fibroids and she had recently received COVID-19 vaccination. She used to smoke shisha in the past and also had a pet cat. She lived with her husband and four healthy children. There was no history of malignancy in the family.
She was investigated for above symptoms in another hospital and underwent chest X-ray, which showed pulmonary infiltrates. Bronchoscopy was unremarkable. Bronchial washing cytology was negative for malignancy and TB-PCR was also reported negative. Subsequently a clinical diagnosis of sarcoidosis was made and she was commenced on prednisolone 20 mg twice daily for 4 weeks with no change in clinical condition; and repeat chest X-ray showed no improvement.
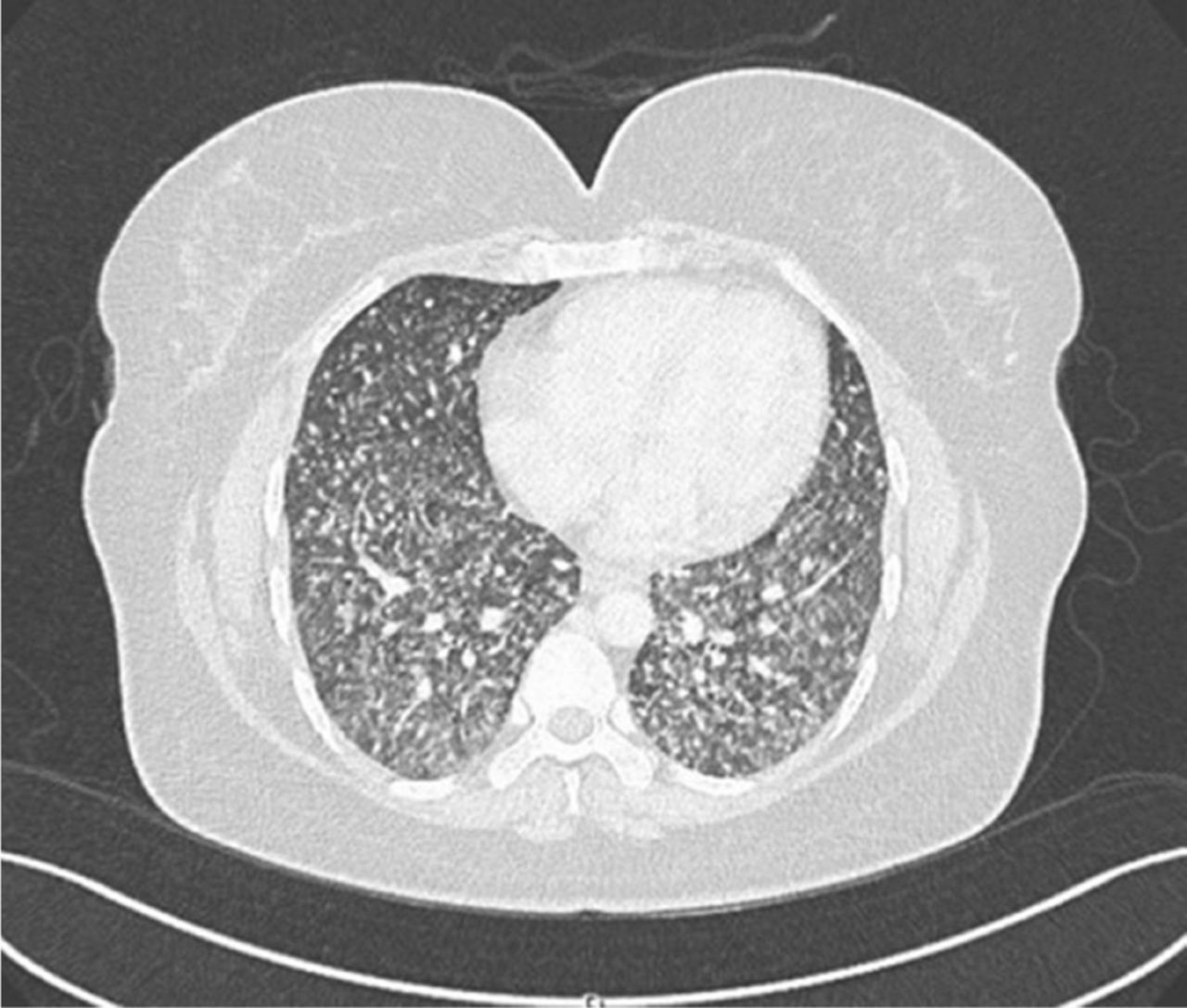
On admission to the pulmonology department, clinical examination was unremarkable with normal vital signs. Routine laboratory investigations including full blood count, urea and electrolytes, serum creatinine, liver function tests and inflammatory markers were within normal limits. Chest X-ray showed scattered micronodular opacities in both lungs (Fig 1). CT scan chest with contrast reported bilateral miliary nodules, mild localised pleural effusion and pleural thickening (Fig 2). CT scan abdomen and pelvis with contrast showed small right adrenal adenoma but no other abnormality apart from evidence of previous hysterectomy. COVID-19 PCR, TB PCR, acid-fast bacillus smear and culture and inflammatory markers were negative. She underwent video-assisted thoracoscopic surgery (VATS) by cardiothoracic surgeon. Wedge resection biopsy showed several small round tan-yellow to grey white solid nodules. Histopathology revealed leiomyomatosis (so-called leiomyomatous hamartomas or benign metastasising leiomyomatosis (BML)). In-house immunohistochemistry (IHC) for estrogen receptors (ER), progesterone receptors (PR), Ki67, human herpesvirus-8 (HHV8), CD34, S100, CD117 and smooth muscle actin (SMA) was performed and showed strong expression of SMA in tumour cells consistent with smooth muscle tumour with no morphological features of malignancy. ER and PR showed diffuse and strong nuclear staining (Fig 3). Ki67 showed a 5–10% proliferation index in the tumour cells. The remaining markers were negative. The case was discussed in a multidisciplinary team meeting, where histology and imaging were reviewed and a diagnosis of BML was confirmed. The patient and her family were counselled about the rare diagnosis and further management.
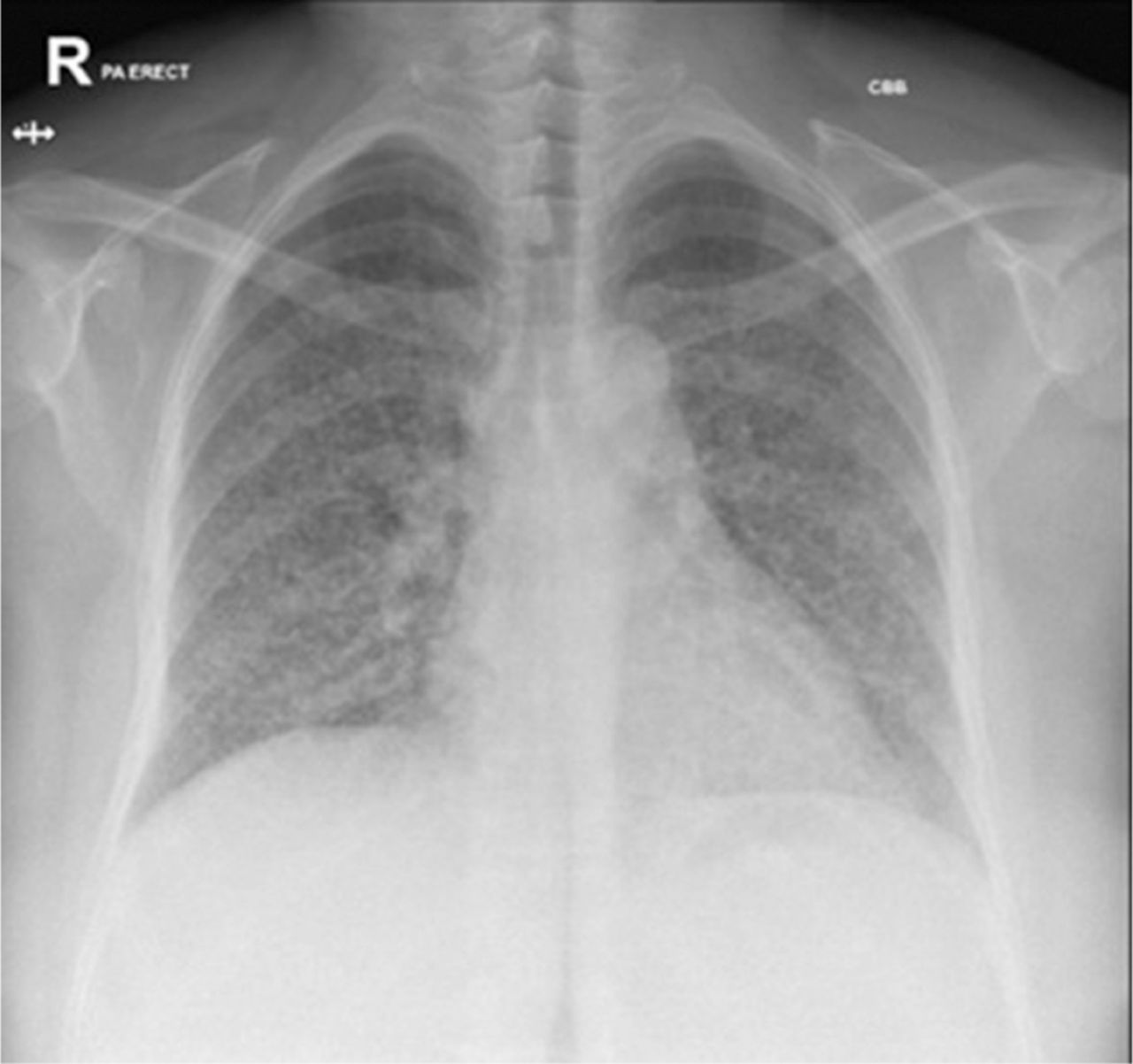
Chest X ray shows micronodular opacities in both lung fields.
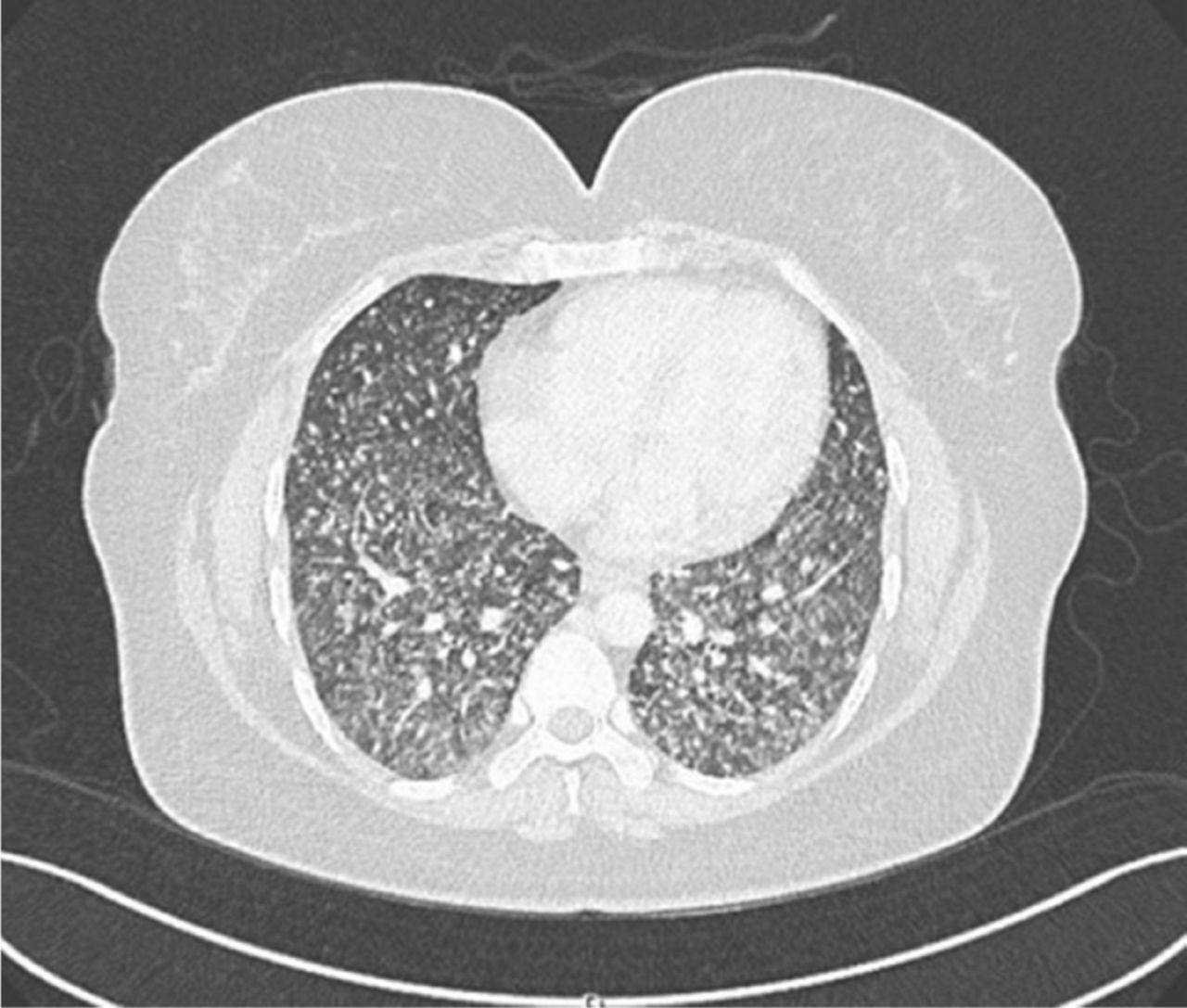
CT scan chest with contrast shows bilateral miliary nodules.

(a) Pathological examination of lung wedge resection specimen reveals multiple variable sized eosinophilic stromal solid nodules in the lung parenchyma. (b) Histology shows intersecting bundles of smooth muscle spindle cells. (c) The spindle cells are positive for smooth muscle actin immunomarker. (d) The spindle cells show nuclear staining for estrogen receptor.
In view of the patient's symptoms and strong ER, PR staining of tumour cells, the option of active therapy with endocrine manipulation was recommended. The patient was commenced on tamoxifen 20 mg daily and discussed molecular profiling to further characterise the disease and investigate potential targeted treatment.
Discussion
Uterine leiomyoma are very common tumours in premenopausal women. The tumour originates from uterine smooth muscle cells or myometrium and its growth is dependent on the levels of circulating oestrogen.2 The majority of the uterine leiomyoma are benign, while malignant cases account for up to 6%.3 However, despite being benign, they can sometimes metastasise to extrauterine sites.
BML is rare and often associated with a past history of uterine fibroids, myomectomy or hysterectomy.4,5 BML is associated with distant spread of leiomyoma to extrauterine sites including lung, bone, spine, lymph nodes, retroperitoneum, skin, central nervous system and intravascular spread.5,6 The lung is the predominant site of metastasis. The mean time from primary surgery to BML diagnosis has been reported to be between 8 and 15 years.
There are several hypotheses about the origin of BML, as the lesions show close resemblance to uterine leiomyomas.5 Some believe that the tumour is hematogenously spread and surgical procedures including uterine curettage, hysteromyomectomy and hysterectomy may disseminate the tumours to the lung through the venous circulation.7 However, it has been reported in some cases without a history of uterine surgery.
Pulmonary BML (PBML) is characterised by presence of multiple bilateral benign leiomyomas in lungs. Clinical presentation is variable and some patients present with a history of shortness of breath, cough and (rarely) chest pain. Although the majority of patients present with minimal symptoms, there are case reports of patients presenting with severe and distressing symptoms requiring hospitalisation.8
PBML usually presents with multiple bilateral pulmonary nodules, but solitary lesions have also been reported. Required imaging investigations include chest X-ray and CT chest scan. PET scan usually shows no FDG uptake. Extrapulmonary disease is rarely found on further diagnostic investigations.
BML is often misdiagnosed initially. Histological diagnosis is required in all cases to rule out underlying malignancy; however, it can be difficult. Most patients require invasive procedures including wedge resection and video-assisted thoracoscopic surgery (VATS).
Histologically, BML is characterised by well-defined nodules ranging from miliary size to up to 10 cm. Immunohistochemistry (IHC) markers are positive for SMA, desmin, estrogen receptor (ER), progesterone receptor (PR), with low Ki-67 score. IHC is negative for S-100, CD34, CD117. Our patient was positive for SMA, ER, PR and Ki-67 was 5–10% (higher than reported in other case series).
Due to the rarity of BML, there is a lack of standard treatment strategies. Jacobson et al. have reported response to LHRH analogue after failure of treatment with progesterone analogue, medroxyprogesterone and tamoxifen in very symptomatic oxygen dependent patients.9 Some patients with solitary nodules can be treated with surgery; however for the vast majority of patients, curative resection is not possible due to multicentricity of the disease. Asymptomatic patients can undergo a period of observation. Other treatment modalities have been tried including castration (surgical or medical), oestrogen receptor antagonist and aromatase inhibitors.8
Conclusion
BML is a rare entity and tends to be asymptomatic; however, many patients present with clinical features resembling underlying malignancy. Therefore, in women of reproductive age with previous hysterectomy and multiple lung nodules on imaging, the diagnosis of BML should be taken into consideration. Treatment should be individualised based on symptoms and extent of disease.
- © Royal College of Physicians 2023. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.