
Introduction
When the Harveian oration was established at the College of Physicians in 1656, it was determined that it should address experimentation and be delivered in Latin, a tradition mercifully suspended during the mid-19th century.1 In deference to Harvey, I offer you the title of my lecture, ‘Pandemic HIV and its legacy for global health’, in Latin, ‘Pandemicum HIV eiusque legatum medicinae et sanitatis globalis’, but will continue in English.
William Harvey started his studies in medicine at the University of Padua in Italy, graduating in 1602.2 He was a model for contemporary scientists in benefiting from cross-European collaboration evident among the scholars of Padua University at that time. The Paduan scholar Fabricius had identified the valves of the veins in 1603,2 which gave Harvey one of his key ideas for his seminal discovery of the circulation of the blood, and enabled him to demonstrate the direction of the flow of the blood in the veins. Harvey's anatomical understanding would have benefited from studying dissection in the recently opened anatomy theatre, which is still visible in the University. Harvey might have also been exposed to the work of Giralomo Fracastoro (1478–1553) who, in 1546, published his book De contagione et contagiosis morbis et curationis, in which he proposed contagion as ‘specific infection which passes from one subject to another’ caused by ‘seminaria’ or something living.2 Remarkably, this was some three centuries before the germ theory became widely accepted. Harvey, describing the mechanism of the circulation of the blood, did not understand its many functions, least of all what we now know can also be its role in transmitting infectious agents, the subject of today's lecture.
As we emerge from the coronavirus 2019 (COVID-19) pandemic, and reflect on lessons learnt, and what we got right and wrong, I turn, in today's Oration, to a pandemic that we first became aware of just over 40 years ago. This paper provides a historical and current perspective and suggests 10 legacies arising from HIV, ranging from societal changes and scientific advances to health equity, in the UK and globally (Fig 1). I consider their influence on the practice of medicine and the evolution of global health and whether they have endured today.

Ten legacies of the HIV pandemic.
The first description of what became known as the ‘Acquired Immune Deficiency Syndrome’ or AIDS was published in the CDC Morbidity and Mortality Weekly Report in 1981.3 That first epidemiological investigation of a cluster of five young men with evidence of immunodeficiency, manifesting as Pneumocystis carinii pneumonia, showed that they had a homosexual lifestyle in common. This first description gave the clue that the cause would be a common exposure, likely to be an infectious agent.
It was another 2 years before the first isolation of a retrovirus from a patient at risk from AIDS. This was subsequently proven to be the cause of AIDS, and named ‘Human Immunodeficiency Virus’. For this, Francoise Barre-Sanoussi and Luke Montagnier were awarded the Nobel Prize in Physiology or Medicine in 2008.4
Although the earliest cases of AIDS were identified in men with homosexual lifestyles, recipients of infected blood transfusion or blood products, (notably those with haemophilia), or who had a history of sharing needles for injecting drug use, it soon became evident that an undetected but extensive epidemic of HIV was occurring largely as a result of heterosexual and mother-to-child transmission in parts of sub-Saharan Africa.5 For example, studies in the country that was then known as Zaire, showed that prevalence was high in the general population, with both women and men affected, but with the highest proportion occurring in young women.
In subsequent decades, we have come to realise that HIV emerged from related primate viruses not 40 years ago, but during the first two decades of the 20th century. Virological detective work identified HIV antibodies in blood samples stored decades before the emergence of the pandemic. Through epidemiological investigation, detailed sequencing and studies of viral evolution, using molecular clock analysis, the likely temporal and geographic history of the pandemic was tracked.6
As with the current pandemic of severe acute respiratory syndrome-coronavirus 2 (SARS-CoV-2), the virus causing COVID-19, the start of the HIV pandemic was awash with scientific uncertainty because we had limited knowledge of the key biological and behavioural parameters that were driving the epidemic. We might have now become familiar with the prognostications of mathematical modellers, but both the methods and computing power of modern mathematical models were in their infancy in 1981. The first set of projections for AIDS in England and Wales in 1988 were undertaken by a working group chaired by Sir David Cox, whose report produced a wide range of estimates,7 with an order of magnitude difference between them even for a short time frame. All projections except those of Anderson and colleagues were based on extrapolation of epidemic curves rather than on modelling of the underlying factors driving the pandemic.8
Transmission dynamics
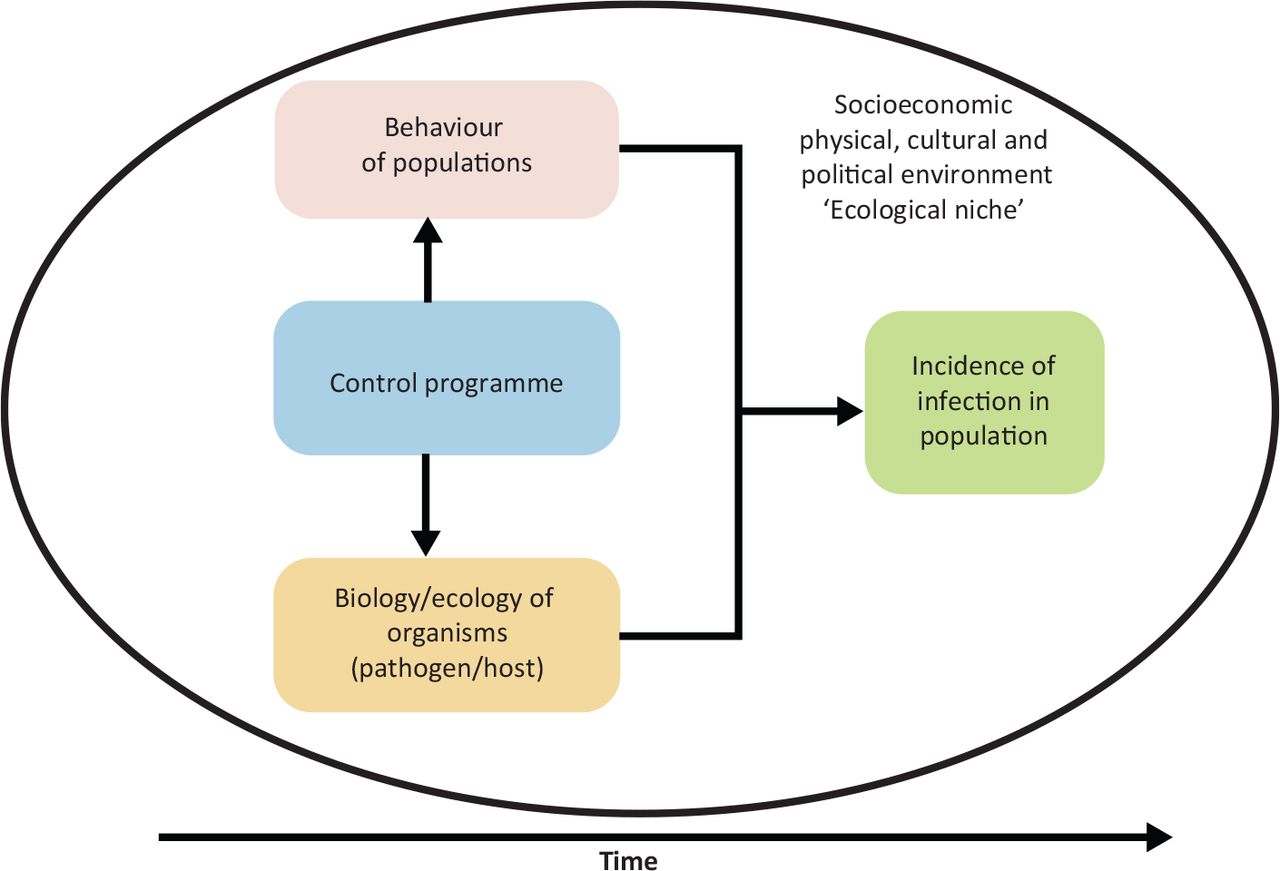
Understanding the trajectory of the pandemic needed a holistic approach to transmission dynamics exploring the interaction between the behaviour of populations and the biology of HIV (Fig 2). Early public health interventions rested on understanding the biology of both the virus and the human host. Key epidemiological parameters (which took years to unpick) included the incubation period from infection to disease, the duration and variability of infectiousness, the absolute and relative risk of different routes of infection, the variability in disease severity and the unknown duration of infection. The last of these we now know to be lifelong in all but exceptional cases. The spread of infection also depended crucially on patterns of behaviour. The public health response depended on changing the behaviour of populations in the most private areas of their lives, notably sexual behaviour. However, very little was known in 1981 about the variability of sexual partnerships, sexuality, injecting drug use or sexual practices.

Drivers of transmission of infections: a population view.
Infection incidence is also driven by wider social, economic and structural drivers, which, in turn, influence the biology of the organism and the human host and behaviour of populations over time. It follows that the control of infectious diseases needs to take account of this entire system when designing intervention programmes.
The COVID-19 pandemic has raised public awareness of the R (case reproduction) number. When a new infection is introduced into a susceptible population, we refer to Ro, defined as the average number of new infections transmitted by an infected person during the infectious period. Where R is greater than one, an epidemic will grow, where less than 1, it will decline. A simple mathematical model for a sexually transmitted infection uses three key variable determining the R number (Equation 1):
Ro = β C D [1],
where β is the probability of transmission of infection from an infected to an uninfected person, C is the effective rate of partner change and D the duration of infectiousness.9
For a sexually transmitted infection (STI), close sexual contact is required for transmission and β can vary by different sexual practices, use of condoms, stage of infection and other parameters, including presence of other STIs and circumcision.
Ecological niche
Understanding these parameters was crucial to understanding the ecological niche that facilitated the HIV pandemic. Given that HIV is transmitted only through sexual contact and blood, it followed that the virus would only achieve epidemic status in populations with sufficient rates of sexual partner change. The virus has the advantage of a long incubation period to disease (many months to years) and a long asymptomatic and infectious period (D), which allowed for a hidden epidemic to emerge unnoticed over several decades. Biologically, the virus has the advantage of attacking the host immune system and, thus, escaping immune control mechanisms.
Equally important were the changing behaviours in human societies. This included the emergence of the injecting drug epidemic during the 1960s, the use of blood and blood products therapeutically, which led to infection through that route, and the substantial changes in sexual behaviour that emerged across the world from at least the late 1950s onward. The related and concurrent occurrence of STIs and genital ulcer disease, we were to discover, also contributed to the increased probability of transmission. HIV could also pass from one generation to another through maternal-to-child transmission.
Individual behaviour was, in turn, influenced by socioeconomic changes, including rural–urban migration in many parts of sub-Saharan Africa, population growth, travel and circular migration, and employment practices, which separated men from women, and stimulated the social and economic drivers of commercial sex. Alongside this was the stigmatised nature of both affected communities and the behaviours driving the epidemic, such that many were frightened to seek care.
The medical and health professions themselves had limited skills and language to address STIs, which were frequently managed in anonymous highly confidential services, hidden from the mainstream of medicine.
Legacy 1: bringing sexual health into the mainstream
This brings me to the first legacy of the HIV epidemic: bringing sexual health into the mainstream of medicine.
Addressing HIV meant not only dealing with a lethal infection killing previously healthy young men in the UK, but also learning to talk about sex, sexuality and injecting drug use, topics that were then small print in the medical curriculum. It also meant addressing stigma and prejudice, which, during the 1980s, was tricky territory. The fictional account of the early days of HIV in the BBC television series ‘It's a sin’ in 2021 was a remarkably realistic reminder to many of us working on AIDS at the time, of the fear, stigma and hidden nature of the epidemic. Arguably, it underlined our inability as a profession to recognise that sex and sexuality were crucial parts of the human experience, which have a wide range of consequences for human health, including STIs, HIV, unplanned pregnancy and sexual violence.
As during the current pandemic, the then chief medical officer, Sir Donald Acheson, had to negotiate the presentation of emerging scientific evidence to policymakers and politicians whose views on policy were coloured by their own attitudes, experience and political leanings. Royalty had their role too, notably that of Diana Princess of Wales, when she famously shook hands with a patient with AIDS at the opening of the first ward for such patients at the Middlesex Hospital in 1987. Interestingly, this single event probably had one of the biggest impacts on overcoming fear of casual contagion. However, in the widely publicised photograph of the time, the patient's identity was hidden, at a time when HIV/AIDS was so highly stigmatised.
Margaret Thatcher and the national AIDS response
Political nervousness was at its height and recently released papers from the National Archive, which I extracted in preparation for this talk, illustrate the extent to which some of the politicians of the day were out of touch with the sexual behaviours and mores of the time. The views of the then prime minister, Margaret Thatcher, regarding the proposed newspaper adverts are informative here. In response to being informed that ‘Norman Fowler is proposing to place explicit and distasteful advertisements about AIDS in all the Sunday papers’, her handwritten marginalia say ‘Do we have to do the sections on risky sex? I should've thought it could do more harm if young teenagers were to read it’.10
Yet, we were trying to design public health interventions and information for the public based on very little qualitative or quantitative information on sexual attitudes and lifestyles, such as the proportion of the population with same-sex relationships, rates of partner change and sexual practices. The Cox Report7 had emphasised the need for such information and for a large-scale representative population survey to determine the risk of future spread. In 1988 a group of us that included myself, Jane Wadsworth, Kaye Wellings and Julia Field, set out to address this data gap.11
However, direct measurement of the behaviours that were crucial to designing the public health response, turned out to be as controversial and stigmatised as the infection itself. After successful completion of a large-scale feasibility study that demonstrated the acceptability of a survey of sexual lifestyles in the general population,12 proposals for Government funding of the survey created nervousness at the highest level.
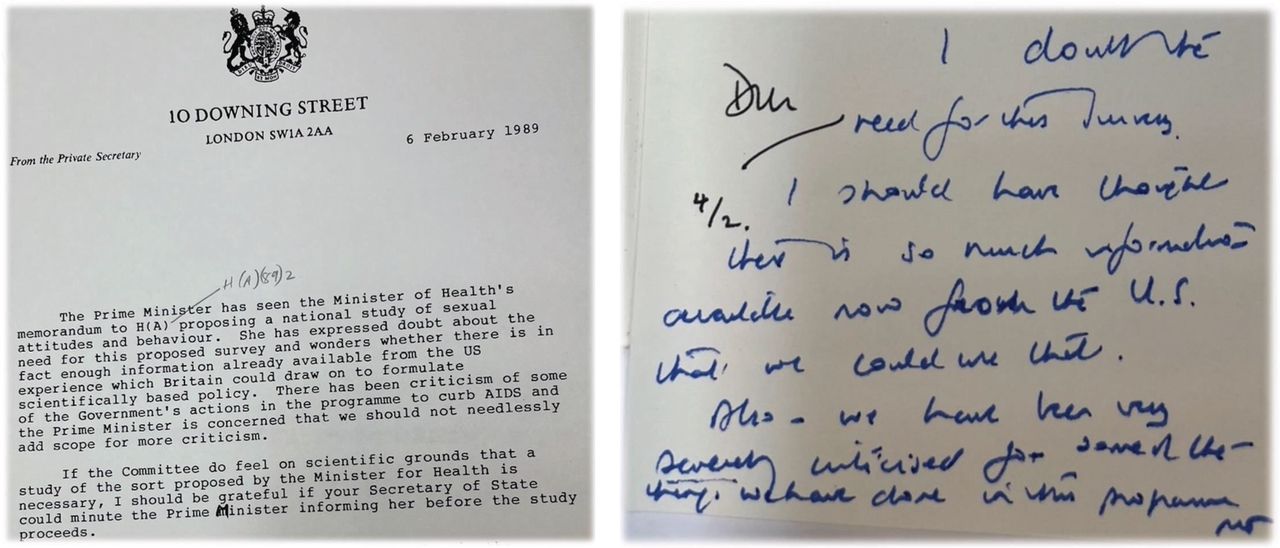
Margaret Thatcher's hand-written annotations of February 1989 record ‘I doubt the need for the survey. I should have thought there was so much information available now from the USA that we could use that. Also, we have been very severely criticised for some of the things we have done in the programme’.13 Despite apparent support at ministerial level and elsewhere, Government decisions were delayed (Fig 3).

Political nervousness about the proposal for a survey of sexual behaviour for the prediction and prevention of an HIV pandemic: Margaret Thatcher's notes from February 1989. Source: National Archive PREM 19/2775 (reproduced with permission from the National Archive).
Five months later, the prime minister's views had hardened further. On being advised that ‘Mr Mellor seems to think that government can keep at arm's length from the survey and recommends that it goes ahead’, she noted in hand-written marginalia:
‘I think people rightly would be deeply offended by questions of this nature and I do NOT think we are entitled to intrude into their privacy. Neither government nor government money should be involved in any way if this survey goes ahead’ (Margaret Thatcher's notes on the proposed National Survey of Sexual Lifestyles. July 1989).13
Despite extensive scientific support and many studies among high-risk populations, such as men who have sex with men and injecting drug users, general population studies of the behavioural drivers of HIV that were crucial to control, were not deemed acceptable for public funding. In September 1989, The Sunday Times ran an exclusive story, entitled ‘Thatcher halts survey on sex’ reported the banning of the survey from public funding. By this time, a crucial year had been lost. Similar squeamishness about behaviour surveys was evident in other countries, notably the USA.
However, Wellcome Trust came to the rescue and, only 10 days after the ban, agreed support and we were able to progress the first National Survey of Sexual Attitudes and Lifestyles ahead (Natsal).14 Three decennial surveys have subsequently addressed not only the drivers of HIV, but also many other aspects of sexuality (a fourth is now in train). The surveys tracked extensive changes in lifestyles that had occurred over the decades preceding the pandemic, characterised by earlier age of first sexual intercourse, increasing numbers of sexual partners and a widening time gap between first intercourse and first child. Proportions of those reporting same-sex experiences also increased, both prior and subsequent to the emergence of HIV.11,15
Data from the these and other surveys were widely used to inform not only HIV policy, but also a wide range of related issues that came into focus as a result of HIV, ranging from STI epidemiology and Chlamydia screening, to human papilloma virus (HPV) vaccination, sex education, contraception and sexual violence.
By 2013, attitudes had changed, a range of new sexual health services had been developed and, in 2001, the Department of Health published a sexual health strategy addressing ‘the sexual causes of preventable death and ill health’.16 By the time of publication of the third Natsal survey in 2013, which addressed a much wider range of issues, the field had come a long way to a position in which sexual lifestyles were increasingly recognised as a mainstream and legitimate focus of public health policy ‘practice and research’.17
Legacy 2: Co-production of science, prevention and care
A key component of challenging stigma and opening the conversation about sex was work by, and with, affected communities. The concerted and organised efforts of AIDS activists and the public had a profound impact on overcoming stigma, in turn driving the co-production of science and public health response. What was achieved in HIV research has become the accepted standard for much clinical research, which is now routinely expected to demonstrate a strategy for patient engagement and public participation. Affected communities were crucial in driving the initial behavioural response, advocating for research, access to treatment and moving the provision of care from that of passive recipient to active participant. This was at the heart of care provided on the first AIDS wards in London, and has now percolated to many other areas of clinical care.18
The impact of efforts of the gay community, notably the Terrence Higgins Trust, were profound. Nicholl et al demonstrated that the peak of HIV incidence in men who have sex with men occurred around mid-1983, following intensive community campaigns. Incidence had already fallen substantially by the time the broader population government campaigns were introduced in 1986.19
Community action, and cultural and behaviour changes, have remained at the heart of the pandemic and have been essential in reducing incidence. Despite the increasing worldwide availability of antiretroviral therapy, combination prevention remains essential. Condom use alone is estimated to have averted over 110 million HIV infections globally.20
Community engagement remains a core asset for research and service delivery throughout the world to this day. For example, the PROUD trial provided key evidence of the effectiveness of pre-exposure prophylaxis for HIV prevention and involved community advice at its centre, in design, recruitment and dissemination.21
Legacy 3: driving a holistic right based approach to sexual health
This brings me to the third legacy. The public discourse around HIV opened a much wider global debate, which extended far beyond concerns for HIV control to those of challenging stigma and developing a rights-based approach, to not only sex and sexuality, but also a wide range of sexual health issues. This was formalised in the WHO definition of sexual health in 2006. According to the current working definition, sexual health is:
‘...a state of physical, emotional, mental and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction or infirmity. Sexual health requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination and violence. For sexual health to be attained and maintained, the sexual rights of all persons must be respected, protected and fulfilled’.22
Although there are many other streams of evidence, community action and fields of health contributing to this definition, HIV was one of the key drivers of a holistic and rights-based approach to sexual health now advocated by many in the HIV field. In all this, the public have had a profound role alongside the professionals involved.
Legacy 4: innovation in surveillance
However, while activists, the public and professionals drove forward changes in attitudes, behaviour and services, HIV also drove profound changes in a range of scientific methods. This brings me to the fourth legacy. Infection surveillance moved from clinical case counts to much more sophisticated measures using population surveys, data integration and mathematical modelling. These were not only key to understanding the HIV pandemic, but also laid the groundwork for enhanced surveillance in other infections, including the COVID-19 pandemic.
Here, it is interesting to reflect on the historical development of surveillance. The stigma of HIV diagnosis and testing had the paradoxical effect of enabling some of the first unbiased population surveys of HIV and other STIs to be undertaken. In 1986, when HIV testing first become available, patients were cautioned against testing at a time when there was no effective treatment, and the interpretation of HIV positivity was clinically uncertain. Testing was only undertaken in the context of counselling regarding the risks and benefits of knowing one's status given the stigma around diagnosis.23 The early stigmatisation of HIV effectively discouraged diagnosis and threw a long shadow, which has extended to many parts of the world, and continued into the time when those living with HIV could receive substantial benefits from treatment and care. In 1998, Kevin de Cock and I proposed that HIV testing needed to move from ‘exceptionalism to normalisation’ to encourage HIV testing and secure therapy, thus avoiding suffering from undiagnosed late-stage disease. 24 However, the stigma of HIV diagnosis has persisted over the past 40 years, and it was only in 2022 that Terrence Higgins Trust, for example, was able to welcome the announcement of routine HIV testing of patients in a wide range of clinical settings.
Limited testing demanded a different approach to population surveillance. After considerable ethical debate, the UK embarked on a large-scale unlinked anonymous testing programme. This used unselected residual blood specimens from patients in a range of settings, which were tested anonymously for HIV antibodies without return of results, to estimate the prevalence of infection.25
The first UK unlinked anonymous HIV prevalence study was undertaken in the Middlesex hospital during the mid-1980s and provided shocking results. In men who have sex with men attending the genitourinary medicine services at the Middlesex hospital, the proportion infected with HIV (ie prevalence) rose from 3% in 1982 (only 1 year after the first cases of AIDS were identified) to over 20% in 1984, but then levelled off as behaviour changed and incidence declined.26
In the majority, this infection remained undiagnosed and without symptoms, but it showed the scale and speed of spread of hidden infection during the early years of the epidemic. These types of population survey in key populations became the global standard, driving one of the most sophisticated global surveillance system for any infection.
The development of modern infectious disease surveillance systems is now well established, at least for HIV. The UNAIDS reference group aggregates data from sentinel surveys in 170 countries. Combined with demographic data and mathematical modelling, they have built an ongoing international surveillance capability.27
In this, we can see a blueprint not only for other infections globally, but also a capability for response to future emerging infections. Unlinked anonymous testing has been widely used for other infections and conditions in large-scale surveys and cohorts, whereas large-scale population surveys have become the gold-standard for COVID-19 surveillance.
Legacy 5: new methods for complex population interventions
With better methods available to understand the magnitude of the epidemic came the opportunity for experimentation to intervene at the population level. This meant devising novel approaches to randomised control trials for complex population interventions. These had been developed in other fields, such as malaria, but HIV provided a significant impetus to improve methods. Among the first of these was the trial led by Heiner Grosskurth to examine the impact of population-level treatment of STIs on HIV transmission, in the days before antiretrovirals were available.28 Key to these interventions was that they frequently involved combined behavioural and biological interventions with randomisation, not at the level of individual, but at the level of the population or community, leading to cluster-randomised trials. These involved strong community engagement of leaders and participants alike, and a wide range of disciplines.
An example from a decade later is a study of pupil-led sex education led by Judith Stephenson and Ann Oakley. It was one of the first studies in the UK to involve the randomisation of schools and extend methods rarely used in the educational setting, and was also controversial in its time.29 More recently, the PopART study, published in 2019, examined the effect of universal testing and treatment on HIV incidence in 21 communities in Zambia and South Africa.30
Where these studies are fundamentally different from traditional randomised controlled trials of individual therapeutic interventions is that interventions were compared by randomising communities not individuals and were concerned with measuring population-level rather than individual clinical outcomes. They led to significant advances in methods, process evaluation, combined qualitative and quantitative analysis, and novel statistical techniques for assessing public health interventions.
Legacy 6: innovation in diagnostics
The sixth legacy is one of innovation in diagnostics and their application. The COVID-19 pandemic has highlighted the relative paucity of investment in diagnostic research as well as problems of governance and comparable measures for evaluation. We could do well to translate some of the legacy from HIV. Development of the first HIV antibody test was slow and tests only became widely available during the mid-1980s, around the same time as the invention of polymerase chain reaction (PCR). PCR transformed our ability to identify HIV. Although PCR has become familiar to the general public in the context of COVID-19, HIV was the first infection for which PCR was routinely used not only for diagnosis, but also for quantitative monitoring of response to antivirals, for the development of methods for anti-viral resistance monitoring and for studies of viral evolution. This in turn has built the field of molecular epidemiology and viral sequencing to better understand the evolution of viruses and their origins.
One of the most important developments has been the ability to understand the emerging evidence of antiviral resistance under pressure from antiretroviral drugs. This has inevitably emerged and increased over time and has led to use of resistance monitoring to guide therapy.31 Viral load testing has become a routine part of clinical care, although availability remains limited in lower- and middle-income countries but could be transformed by point-of-care assays for viral load monitoring.
HIV has also been one of the first fields to develop point-of-care antibody tests used for clinical care. In 2015, the first legal HIV antibody self-test was approved in the UK. The field now has significant experience of delivering point-of-care tests in hospitals, communities and their use by the general public, which could be logically extended to many other infections. It is also driving the use of linked mobile diagnostics and care in the field, helping to overcome issues of access, stigma and clinical follow-up through linked remote diagnostics and care.32
Legacy 7: development of antiretrovirals
This brings me to the seventh legacy of driving drug development and other interventions.
The first antiretrovirals became available within a few years of the identification of HIV. Since then, several classes of drug have been identified, including through rational drug design.33 Initial monotherapy rapidly resulted in drug resistance, driving the need for combination therapies. We should not have been surprised by the emergence of drug resistance with monotherapy for a long-term condition given, for example, the experience of needing combined antibiotics for tuberculosis (TB) to overcome resistance. However, HIV has driven broader research into antiviral therapies and their use at scale, all relevant to the search for new antivirals for other conditions. HIV has driven the growth of novel technologies, novel manufacturing and novel drug formulations, such as depot injectables, alongside clinical trial capabilities globally. All of these are applicable to the novel challenges we will face in future pandemic prevention and control.
These advances in combination antiretroviral therapy transformed the prospects for people with HIV. The European Cascade study demonstrated that, once effective combination regimes were proved effective in reducing mortality and suppressing viral load, and treatment was made widely available, mortality dropped dramatically. By 2004 to 2006, HIV mortality in those taking treatment had fallen close to that of the general population.34 Similarly, adult life expectancy of the population in KwaZulu Natal in South Africa had been falling as a result of widespread untreated HIV infection between 2000 and 2004, but rose rapidly following public sector provision of antiretroviral therapy.35
Legacy 8: ethics and human rights in global health research
Initially, only a small fraction of those infected with HIV had access to antiretroviral drugs. Global health inequities were stark and researchers and communities began to question the ethics and human rights in both research and delivery of interventions. In 1997, Lurie et al questioned the ethics of research to reduce perinatal transmission of HIV in developing countries.36 They suggested that we held double standards for research. A controversy arose over the use of placebo randomised controlled trials examining different antiretroviral dosing schedules to prevent perinatal transmission when an effective treatment was already available in high-income countries. This, in turn, provoked debate among researchers, public-health experts and patients on ethical standards and human rights.
The debate continues to this day, but was one of the key stimuli to the development of ethical principles in global health research. In 2002, the Nuffield Council on Bioethics set out a framework for healthcare research in developing countries. They set out four principles: (1) the duty to relieve suffering; (2) the duty to show respect for persons; (3) the duty to be sensitive to cultural differences; and (4) the duty not to exploit the vulnerable. In addressing the key issue of the standard of care, several key recommendations were made: that of independent ethical review in the sponsor's country in addition to the country in which the research is to be conducted; that post-trial treatment should be available for participants; and that, when appropriate, participants in the control group should be offered a universal standard of care. However, when ‘it is not appropriate to offer a universal standard of care the minimum standard of care that should be offered to the control group is the best intervention available for that disease as part of the national public health programme’.37
The debate around ethics and human rights and research in lower- and middle-income countries, particularly when that research is sponsored from outside that country, remains an important and vocal debate. This has widened to ongoing concerns about the need to decolonise research in lower- and middle-income countries and to drive global health equity and capability in the delivery and standards of care and of research.
Legacy 9: improving global health equity
In striving to improve global health equity, perhaps the greatest achievement of the response to the HIV pandemic has been that of driving universal access to antiretrovirals, even though the roll-out did not start in earnest until a decade after therapy had already become available in higher-income countries. The high price of antiretrovirals remained a persistent impediment for some years.
In 2002, health economists and others argued that funding highly active antiretroviral therapy at the expense of prevention would result in greater loss of life and, therefore, that effort should focus primarily on prevention38,39 Articles such as these provoked a vigorous response. Piot40 emphasised the false dichotomy between care and prevention, spelt out the wider societal benefits of treatment, the rapidly falling price of antiretroviral drugs, and the crucial need for a synergistic approach to care and prevention.
The antiretroviral regimes that became available in 1996 were complex, required clinical monitoring, often not available in low and middle-income countries, and were extremely expensive. UNAIDS and WHO launched successful drug access initiatives and, in 2003, President Bush's US$15 billion US President's Emergency Plan for AIDS Relief (PEPFAR) initiative was announced. A key step was finally the World Trade Organization's Doha declaration, which enabled manufacturing of generic medicines for public health crises.
In all this, civil society and political activism had major roles alongside competition from generic drug manufacturers in driving access to therapy. These combined and sustained efforts drove down the price of antiretroviral medicines from US$14,000 per person year in 1990 in high-income countries to US$100 per year for fixed-dose combinations in sub-Saharan Africa in 2018, with a concomitant dramatic increase in people receiving HIV treatment to nearly 30 million, and a parallel decline in AIDS deaths (and HIV incidence).41,42
By 2020, UNAIDS had set targets for HIV testing and treatment. However, a significant gap remains in reaching 95% of all people living with the HIV knowing their status, 95% of these taking treatment, and 95% of those in turn virally supressed. The latest indicators suggest that, rather than 95%, these figures are 84%, 73%, and 66%, respectively.42 Achieving these goals has required a massive financial investment for not only the drugs themselves, but also the testing capability, training of healthcare staff, imaginative approaches to community engagement and service delivery, novel approaches to education, and innovative clinical trial and complex intervention protocols.
While during the first decade of the millennium, clinicians, economists and public health specialists were arguing about the merits of prevention compared with treatment, perhaps one of the key breakthroughs in our understanding of HIV was to identify the role of treatment in preventing not only disease, but also transmission. In 2011, the HIV Prevention Trials Network (HPTN) 052 trial showed that antiretroviral treatment could essentially prevent transmission of infection even without using condoms.43 Observational studies demonstrated similar results in both heterosexual and homosexual discordant couples, with zero transmissions when patient viral load was suppressed and undetectable.44
Here was the missing link in the HIV story, because, if treatment could render individuals uninfectious, this could provide a major incentive to get tested and get treated, knowing that this would protect partners. This led to the campaign for U = U (Undetectable = Untransmittable), which has been heralded as a mechanism to reduce transmission and stigma, encourage participation and bring forward the ambitions to halt transmission, maximise access to treatment and achieve the UNAIDS ambition for zero AIDS by 2030.45
Legacy 10: prevailing against pandemics: putting people at the centre
This brings me to the tenth and final legacy and the one that brings us full circle. In its World AIDS Day report for 2020, UNAIDS focused on ‘Putting people at the centre’, recognising that HIV control could never be achieved without a people-centred context-specific service, integrated with other services, providing comprehensive HIV prevention and care services and removal of the societal and legal impediments to an enabling environment for HIV. Alongside the 95% targets for treatment are the key societal targets for reducing to 10% the number of countries with punitive laws, the population experiencing stigma and discrimination and the proportion experiencing gender inequality and violence.
As the global community regroups and the G7 and others formulate their pandemic preparedness plans,46 we would do well to remind ourselves that technological fixes alone will remain tools on the route to resilience without a much wider set of people skills, community engagement, public health and health service infrastructure and evidence, to reap the population benefits.
There is still a long way to go toward meeting UNAIDS 2030 targets but with a policy of combination prevention based on a policy that brings together biomedical, behavioural and structural interventions, HIV infections globally are continuing to decline. A great deal has been achieved. Forty years on, UNAIDS is looking at least to end AIDS and the UK to achieve not only zero AIDS, but also zero HIV transmission with an 80% reduction in transmission target by 2025.47
So far so good, but will these ambitions be achieved as globally health systems struggle to recover from the direct and indirect impacts of COVID-19? UNAIDS has seen evidence of reduced investment from bilateral donors for HIV control over the past 2 years.48
COVID-19 and HIV
Will the current shocks of the COVID-19 pandemic, conflict and global economic challenges set us off track once again? As we reflect on the COVID-19 response, it is evident that the same areas of the world with limited access to antiretrovirals have similar limited access to COVID vaccines. Over two-thirds of the world's population had had at least one dose of a COVID-19 vaccine but only one-fifth of people in low-income countries as of August 2022.49
Progress in HIV was achieved through extraordinary progress in antiretrovirals, diagnostics and clinical research, but has involved far more than the technologies alone. It has depended on integrated service delivery, community engagement, cultural and behavioural change, political commitment, and global cooperation and funding. Many of these advances and the infrastructure investment have in turn had a key role in the COVID-19 response. Take, for example, the importance of the capability in HIV research in South Africa, which led to the well-established infrastructure for early identification of the SARS-COV-2 Omicron variant.
Multiple initiatives are in place to improve access to COVID vaccines and other medical advances through WHO50 and to deliver the G7 ambition for future pandemic preparedness.46 There is much we could learn from the hard-won integrated approach taken to HIV control.
In summary, I have set out 10 legacies for which I believe we have the evidence that HIV has influenced not only the control of HIV itself, but also broader aspects of medicine, ranging from public participation, holistic and rights-based approaches to sexual health and global health equity, and improved methods for surveillance diagnostics, therapy and clinical trials. These have had reverberations across a range of topics in medicine. particularly as we face controlling new and emerging infections. The question now is whether these legacies will endure. In recent years, the halcyon days of national sexual health strategies have passed. In the UK, we are seeing continuing decline in investment and sexual health services. The monkeypox epidemic has once again brought stigma against men who have sex with men to the fore.
While a rights-based approach to sexual health continues to be advocated, 69 jurisdictions criminalise private, consensual same-sex activity.51 The decision of the US Supreme Court to overturn Roe vs Wade US means that a woman's right to choose to have an abortion is no longer constitutionally protected. Globally, rights of women, such of those to education and a reproductive health service, continue to be challenged.
During the COVID-19 response, we made great progress in diagnostics and self-diagnostics. We made multiple behavioural and diagnostic investments costing billions of pounds, including investments in testing programmes and a wide range of approaches to test and trace. However, we do not understand their public health impact well. We might not have had the luxury of time in a rapidly moving pandemic, but few nonpharmaceutical interventions, with rare exceptions, were subject to multidisciplinary trials. Anthropological, social and communication science did not receive the prominence that biological science received and yet we remain highly dependent on the willingness of populations to adopt behavioural interventions and vaccines in controlling the pandemic.
Despite all we learned about HIV systems approaches to control, and the pricing policies for antiretrovirals, vaccine equity remains a major global challenge. We have witnessed stark inequalities in COVID impacts and struggled to listen to the voices of communities, families and individuals impacted by the pandemic.
The control of infectious diseases in populations must take a holistic, multidisciplinary, systems approach that considers the entirety of the ecological niche that allows an infectious agent to survive or die-out in the human population. That is the challenge that we face for the future and there is much we could continue to learn to make the legacy of HIV a lasting one across a wide range of fields. Given his background and training in an international, multidisciplinary University in Padua, which understood the importance of cross-fertilisation of ideas, I hope this would be a sentiment of which Harvey would have approved.
- © Royal College of Physicians 2023. All rights reserved.
References








{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Introduction
- Transmission dynamics
- Ecological niche
- Legacy 1: bringing sexual health into the mainstream
- Legacy 2: Co-production of science, prevention and care
- Legacy 3: driving a holistic right based approach to sexual health
- Legacy 4: innovation in surveillance
- Legacy 5: new methods for complex population interventions
- Legacy 6: innovation in diagnostics
- Legacy 7: development of antiretrovirals
- Legacy 8: ethics and human rights in global health research
- Legacy 9: improving global health equity
- Legacy 10: prevailing against pandemics: putting people at the centre
- COVID-19 and HIV
- References
- Figures & Data
- Info & Metrics