
Abstract
We describe an active and latent tuberculosis (TB) screening programme undertaken in Manchester, UK in response to the arrival of a cohort of refugees from Afghanistan. In total, 217 adults and 347 children were offered screening, which involved a symptom questionnaire, Mantoux test or interferon gamma release assay, blood-borne virus screening and a chest X-ray in participants over the age of 11. We found a latent TB infection (LTBI) rate of 15% in adults and 1.5% in children, which is lower than global LTBI estimates. One case of active TB was detected. Screening was undertaken in the hotels where participants were temporarily housed, leading to high participant engagement levels. Attendance rates were almost doubled compared with a previous hospital-based screening programme. Hotel-based screening for TB presented several challenges, including transfer of information and results to secondary care. Understanding these challenges and learning from the programme has helped us refine our screening protocol to optimise migrant TB screening in Manchester in the future.
Introduction
Tuberculosis (TB) is the second-leading infectious cause of death globally, after COVID-19. In 2020, 10 million people developed TB, including 1.1 million children, and 1.5 million people died from the disease.1 Of the global population, 25% are estimated to have latent TB infection (LTBI). Of these, 5–15% will go on to develop active TB.2 In low-incidence countries, such as the UK, most new active TB infections are likely the result of reactivation of LTBI. In migrants, reactivation from latent to active TB is more common during the first 5 years after migration.3 In the UK, 72% of active TB cases occur in people born outside of the UK.4
In August 2021, the Taliban took control of Afghanistan. In response, there was a large-scale evacuation of people from Afghanistan. Under the Afghan Relocations and Assistance Policy (ARAP), 8,000 adults and 2,000 children were relocated to the UK. They were housed in ‘bridging’ hotels and given indefinite leave to remain. Afghanistan has a high incidence of TB, with 193 cases per 100,000 people in 2020. By contrast, in the same year, the UK had 6.9 cases per 100,000 people.1 A country is considered to have high incidence if it has more than 40 TB cases per 100,000 people per year. The overall prevalence of LTBI in Afghanistan is unknown, although one study of Afghan healthcare workers found an LTBI rate of 47.2% when using tuberculin skin testing.5
LTBI is defined as a persistent immunological response to Mycobacterium tuberculosis in the absence of active TB disease. There are several tests available for LTBI, all of which assess the T cell response to M tuberculosis. The Mantoux test is a tuberculin skin test (TST) that requires skilled practitioners to administer and read the test. Two interferon gamma release assay (IGRA) blood tests are available in the UK. No test for LTBI has 100% sensitivity or specificity; IGRA is more specific than a Mantoux test and can be sampled in one visit, but has higher rates of ‘indeterminate’ results in children,6 for whom venepuncture can be a more challenging procedure. As such, National Institute for Health and Care Excellence (NICE) recommends only using IGRA alone in young people if a Mantoux test is ‘not available or impractical’.7 Where many adults need to be screened, NICE recommend the use of IGRA.
There is UK-based guidance from both the UK Health Security Agency (UKHSA) and NICE on LTBI screening for migrants. UKHSA recommends screening migrants aged 16–35 years from countries with a TB prevalence of >150 per 100,000 people, who have arrived in the UK within the past 5 years.8 These age and prevalence figures are based on cost effectiveness and the recognition that the risk of drug-induced liver injury increases with age. NICE guidance recommends screening all new entrants from high-incidence countries who present to healthcare services for LTBI.7 Additionally, the UK Government requires pre-entry screening for active TB in migrants from high-incidence countries. This comprises a symptom questionnaire, chest X-ray (CXR) and physical examination. NICE recommends that this screening is undertaken in the UK for vulnerable migrants from high-incidence countries who have not had pre-entry screening.7
On 27 August 2021, NHS England wrote to NHS leaders setting out the health needs of newly arrived persons from Afghanistan, for which £3 million was set aside. There was a requirement for all persons to be screened for active TB within 3 months of arrival and for LTBI within 2 years. Following NICE guidelines, all adults and children were to be screened for LTBI.
In response to this, Manchester Health and Care Commissioning approached our Trust to plan and implement a TB screening programme. Key stakeholders in the initial planning meetings included adult and paediatric TB medical and nursing teams, commissioners, primary care and a hospital manager, who coordinated the project. Representatives from radiology, microbiology and virology were also involved. Screening pathways for adults and children were developed by the TB clinicians (Figs 1 and 2).
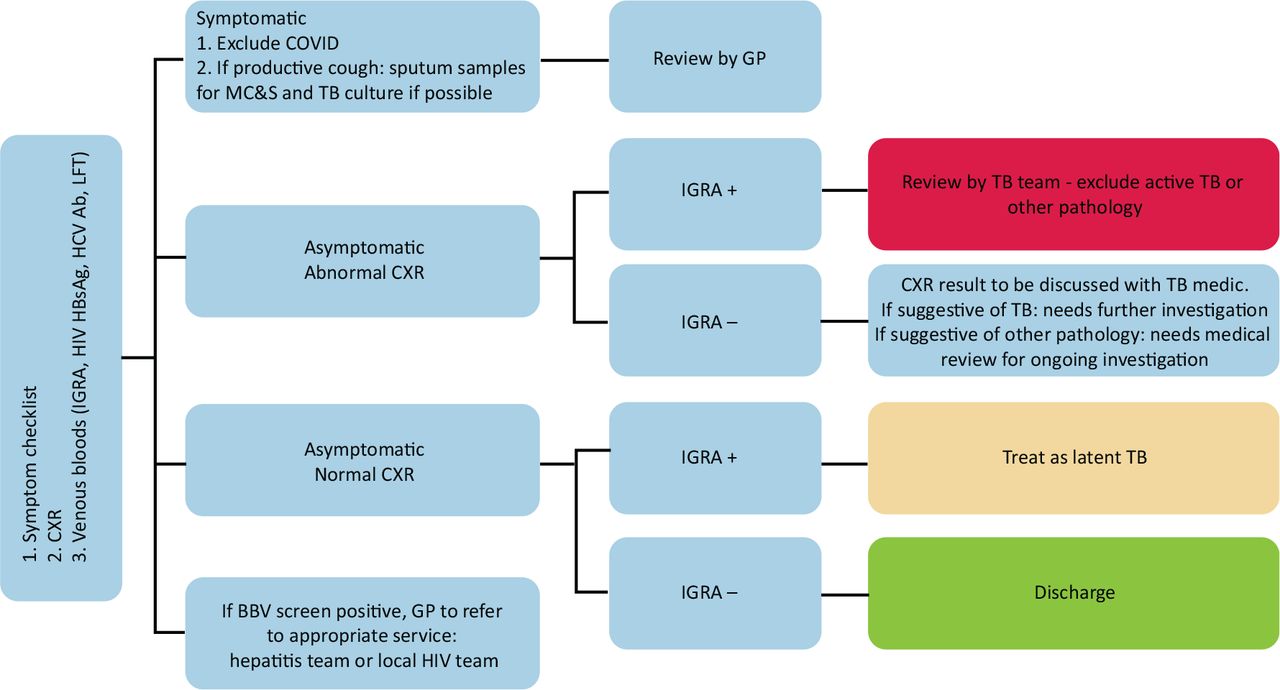
Adult screening pathway for tuberculosis (TB). BBV = blood-borne virus; COVID = coronavirus 2019; CXR = chest X-ray; GP = general practitioner; HCV = hepatitis C virus; HBsAg = Hepatitis B surface antigen; IGRA = interferon gamma release assay; LFT = liver function test; MC&S = microscopy, culture and sensitivity.
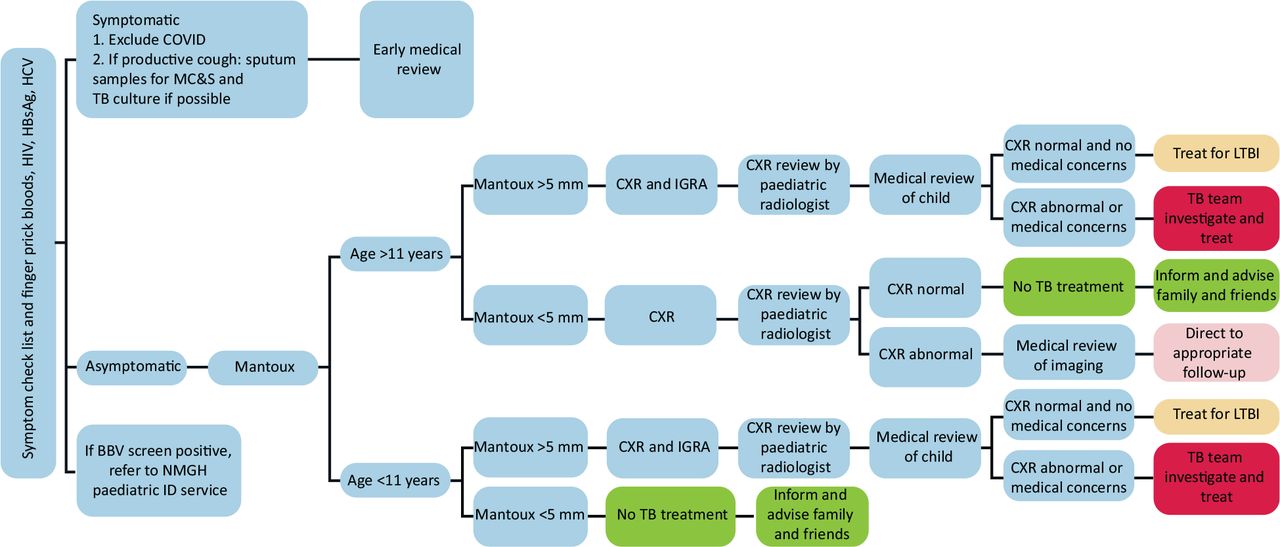
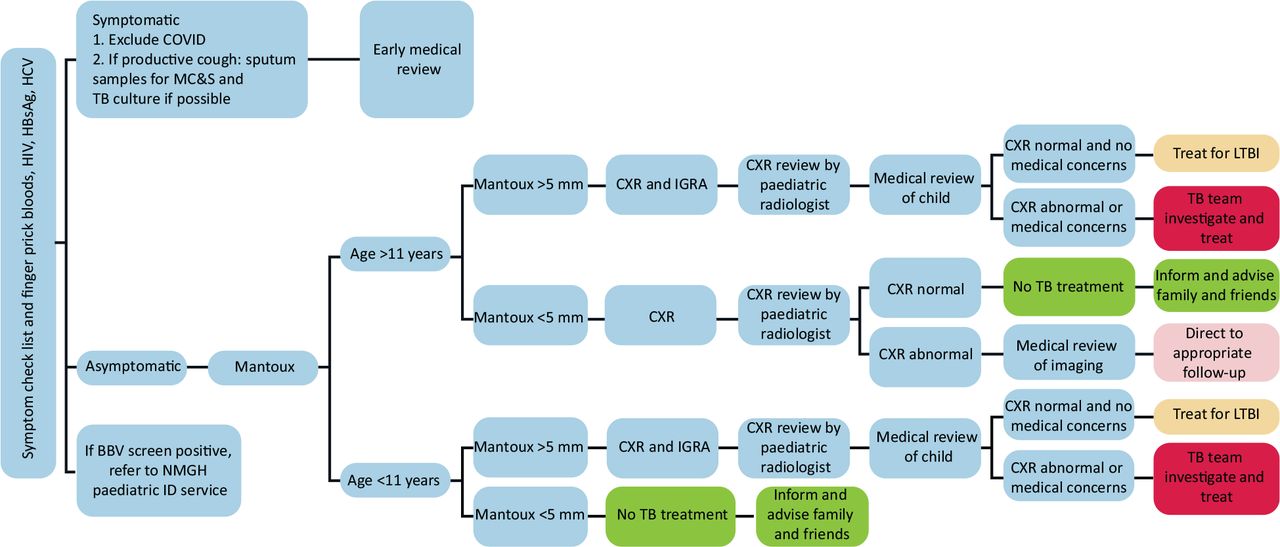
Paediatric screening pathway for tuberculosis (TB). Patients aged <16 years. BBV = blood-borne virus; COVID = coronavirus 2019; CXR = chest X-ray; GP = general practitioner; HCV = hepatitis C virus; HBsAg = Hepatitis B surface antigen; IGRA = interferon gamma release assay; LTBI = latent TB infection; MC&S = microscopy, culture and sensitivity; NMGH = North Manchester General Hospital.
Methods
All newly arrived people from Afghanistan were registered under one general practitioner (GP) practice, which provided hotel-based clinics, with a GP team on-site. All screening tests were requested using the primary care IT system and results were returned to the GP. Results were also visible to the TB team via the Trust IT system. This ensured that results would remain available within primary care if a participant moved to a different area.
Initial screening focused on the two airport hotels where most of the participants resided. Screening started on 11 November 2021, 2.5 months after they had arrived. Screening of adults included a symptom questionnaire completed by a primary care-based advanced nurse practitioner. Blood tests for IGRA and blood-borne virus (BBV) screening were taken by primary care-based phlebotomists and transported to the hospital for analysis, with the results being available to the TB clinicians. An external provider was commissioned to provide on-site chest radiography at the hotels, because the hospital radiology services were unable to perform and report an extra estimated 500 CXRs at short notice. The images were reported and uploaded to our Trust radiology system for review by TB clinicians.
A multidisciplinary team (MDT) was set up with the adult TB team and primary care to review results. All abnormal blood results and CXRs were reviewed by a member of the TB team. Patients with a positive IGRA and normal CXR were referred to the latent TB nurse-led clinic. Those with a positive IGRA and abnormal CXR were urgently reviewed by a TB clinician to investigate for active TB. Those with a negative IGRA but abnormal CXR were referred on to other relevant specialities if the CXR was not suspicious for active TB. Those with a positive HIV, hepatitis C virus or hepatitis B virus (HBV) result were referred to the appropriate clinic. If any participant moved out of the hotels with either positive IGRA or was under investigation for active TB, the TB physicians referred them to the new local TB services.
Paediatric screening was undertaken by TB specialist nurses and paediatric medical and nursing staff at the hotel site. In a single visit, a symptom questionnaire, BBV screening using a finger-prick method and Mantoux testing were completed. The TB nurses returned 48 h later to read the Mantoux tests. As for adult participants, CXRs were performed on site in children aged ≥11 years (Fig 2). Up to three further hospital-based appointments were offered for those who failed to attend. Mantoux rather than IGRA tests were used because sufficient staff trained in paediatric venepuncture were not available at short notice. There were also constraints on laboratory availability for IGRA tests, given the pressure for these from the adult participants. Children with an abnormal (5 mm or more) Mantoux result were then offered IGRA and CXR. All CXRs were reported by an external company and reviewed by a paediatric respiratory/TB physician. Those in whom there were concerns were reviewed by a tertiary paediatric radiologist.
Results
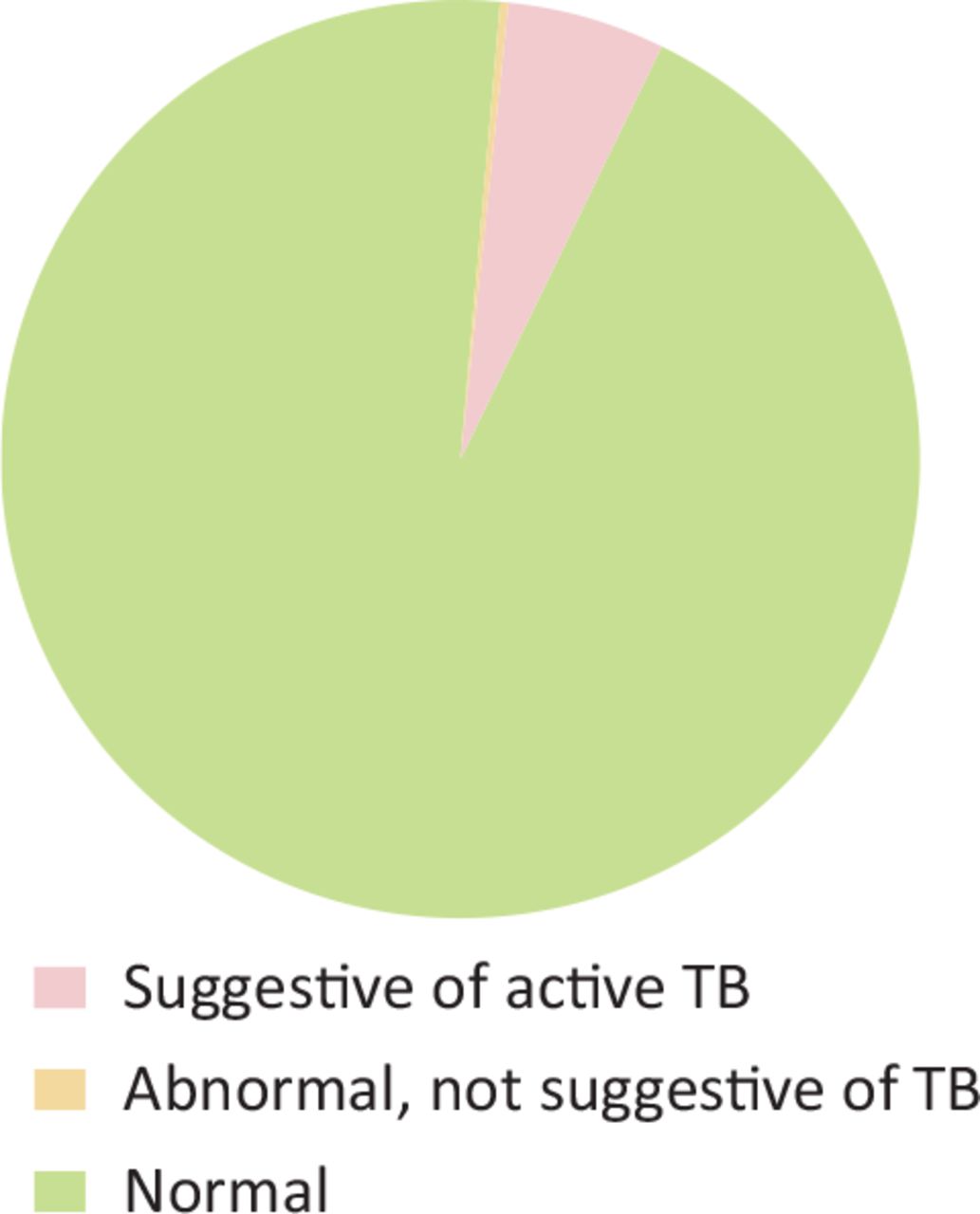
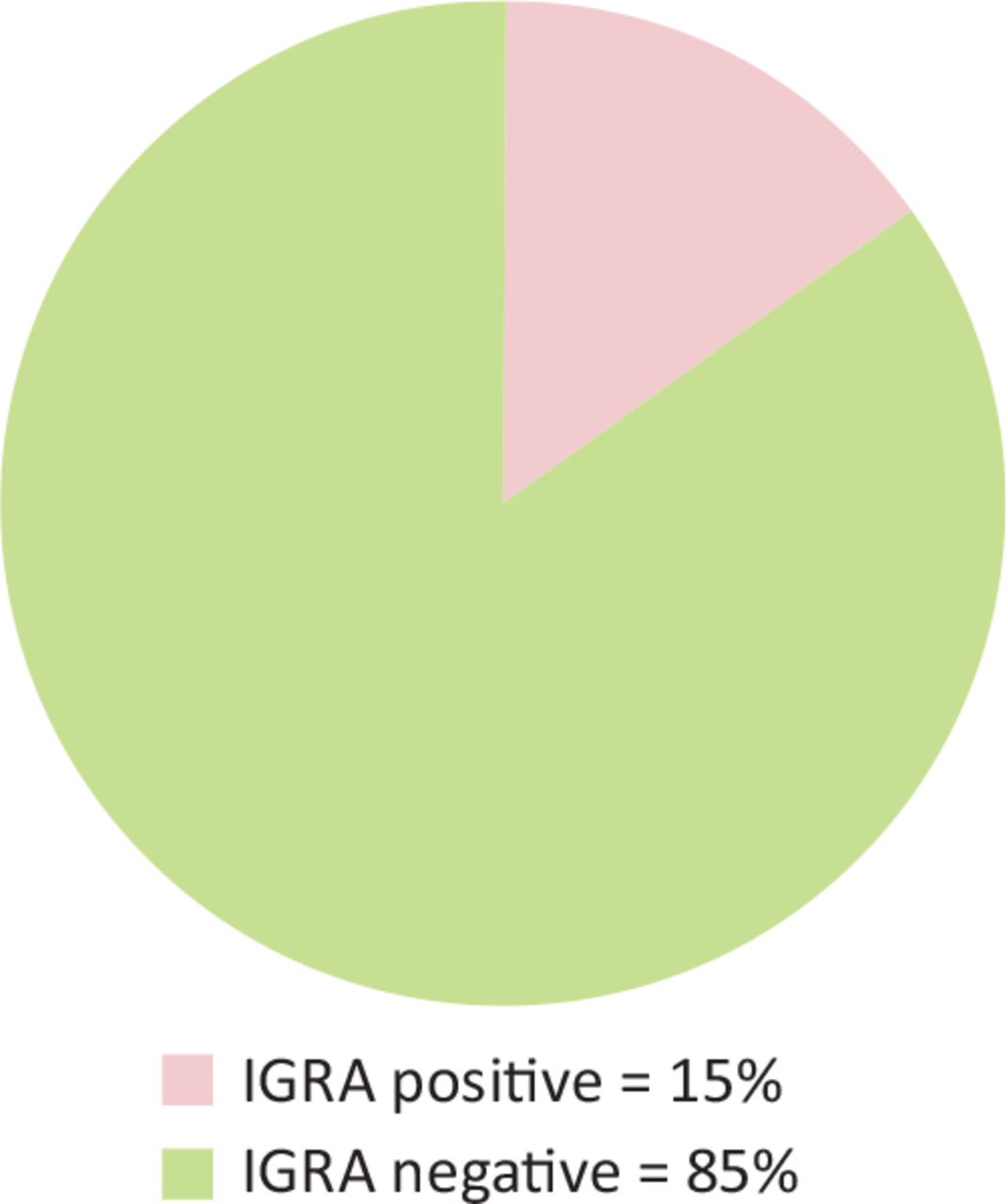
In total, 217 adults were offered screening. The mean age was 32.5 years (range 16–77 years), 1.4% were over the age of 65 and 54% were male (Fig 3). Of the adults, 183 (84%) were screened for symptoms of active TB using the symptom questionnaire (Box 1). No participants reported TB symptoms at the time. In addition, 203 (93%) adults had a CXR, the majority of which did not suggest active TB (Fig 4); however, one showed enlarged mediastinal lymph nodes. A biopsy subsequently confirmed mediastinal TB and the patient was prescribed anti-TB treatment. In addition, 13 CXRs demonstrated other abnormalities and these patients were referred to appropriate specialists. Of the adults, 194 (89%) were screened for LTBI using IGRA. The same number had a BBV screen. Of these, 30 adults (15%) had a positive IGRA and were referred to the LTBI clinic (Fig 5), with 17 adults advised to take LTBI treatment by our service. Most were treated with rifampicin and isoniazid for 3 months, although three people were treated with isoniazid for 6 months. One patient with a positive IGRA had active TB and was treated appropriately. Of the initial adults, 10 moved away from Manchester before they could be seen in the LTBI clinic; they were referred to their new local TB team to ensure continuity of care. Three adults did not attend the LTBI clinic. In addition, four cases of HBV were detected and the patients were referred to the hepatitis clinic.

Age and gender characteristics of screening population.
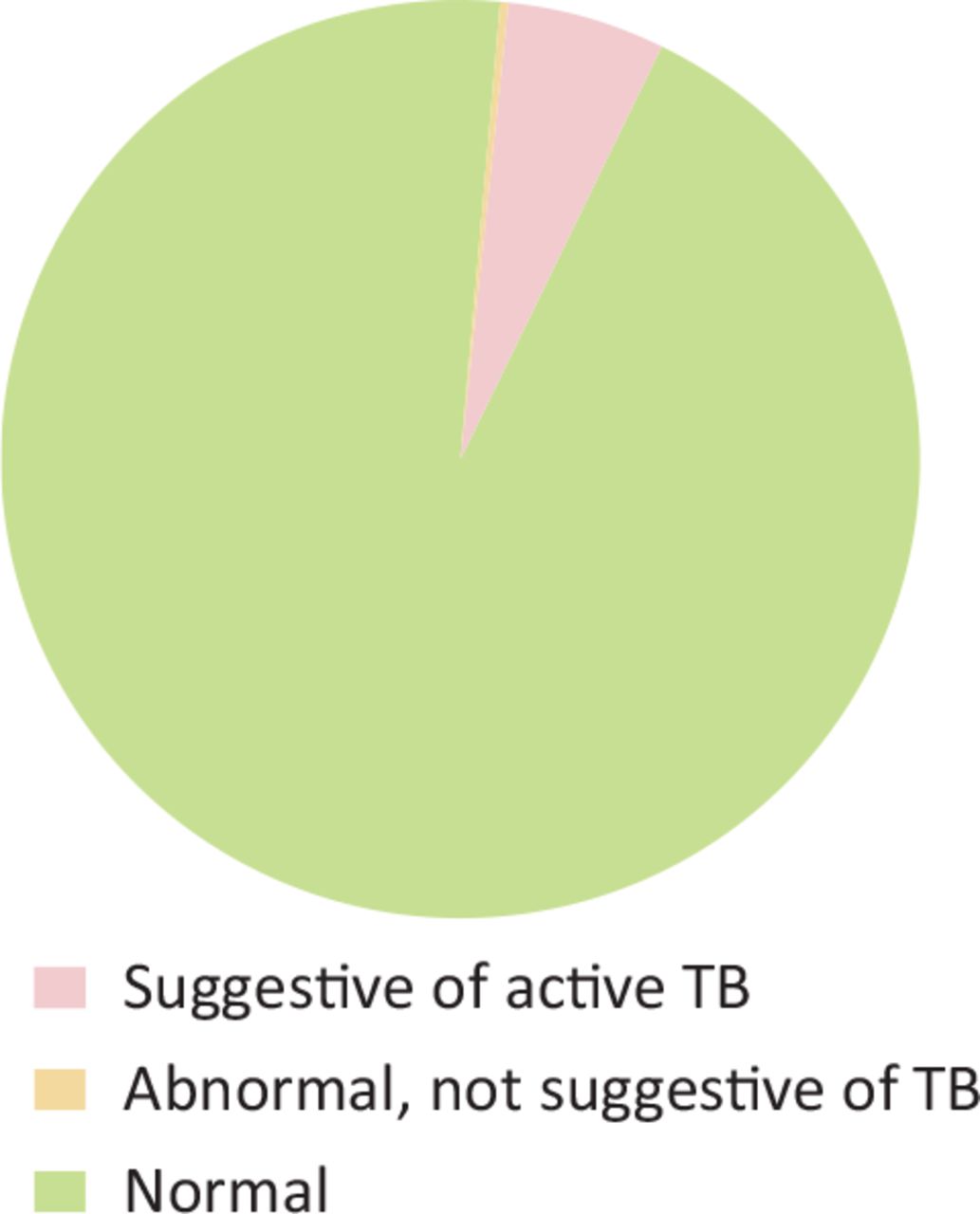
Adult chest X-ray results. TB = tuberculosis.
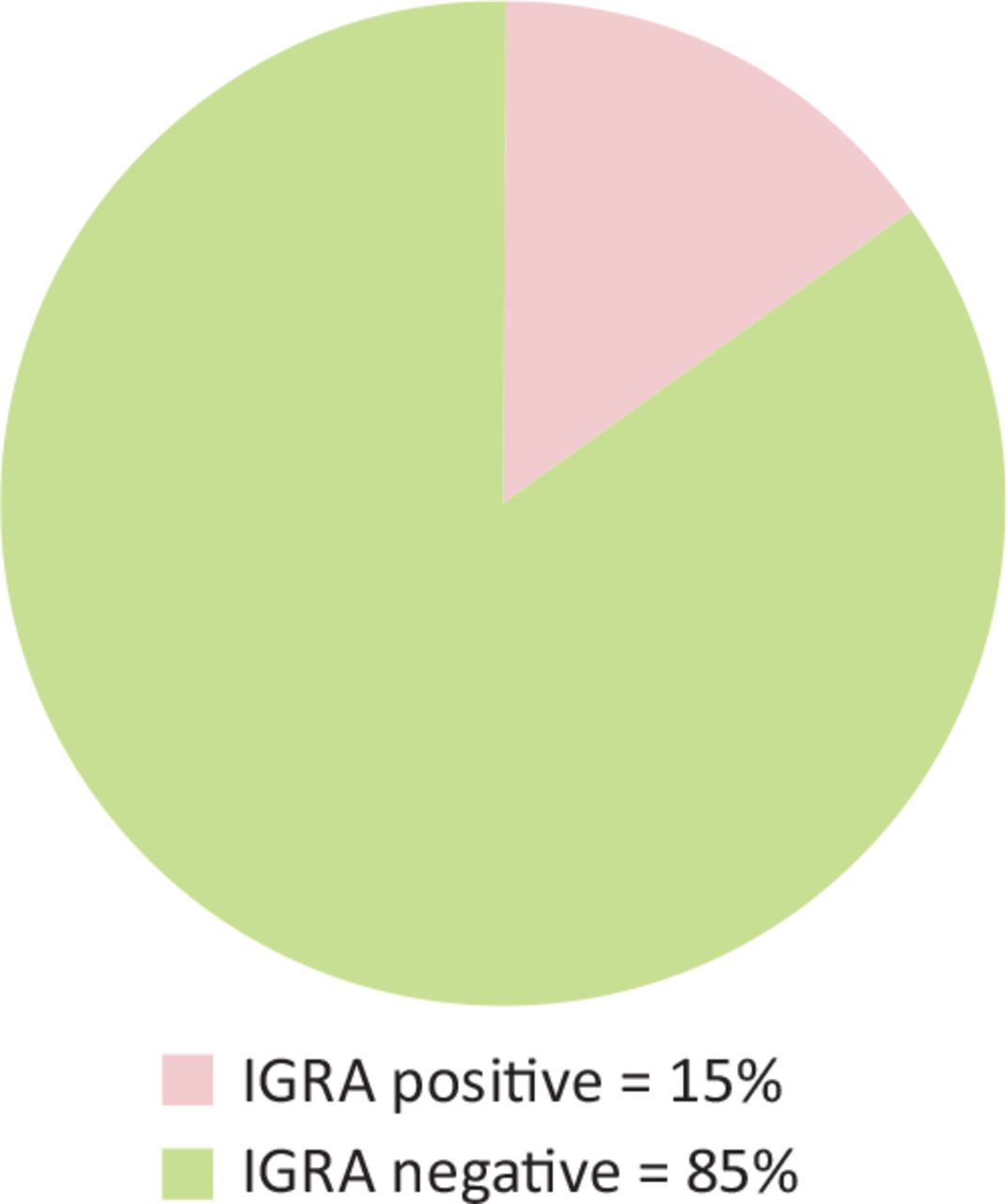
Adult interferon gamma release assay (IGRA) results.
Tuberculosis (TB) symptom questionnaire
In total, 347 children were identified for screening. The mean age was 7 years, (range 0-<16 years), with 262 (76%) aged <11 years (Fig 3). However, 20 children had already moved before the screening visit and a further 70 children moved before the screening process was completed. Of those 327 children available at the start of screening, 313 (96%) completed a symptom questionnaire and 302 (92%) completed Mantoux testing. Of the 25 children who did not complete Mantoux testing, 12 had a subsequent IGRA test. Eight children had a positive (>5 mm) Mantoux result (Fig 6) and 56 out of 85 (65%) children aged ≥11 years and five children under the age of 11 had a CXR. Of the children who were present at the start of screening, 311 (95%) completed LTBI screening and five (1.5%) had results consistent with LTBI (Fig 7). These children were referred to the Royal Manchester Children's Hospital for investigation and treatment. Six children completed LTBI treatment with rifampicin and isoniazid for 3 months. One child started LTBI treatment but did not tolerate it and, therefore, did not complete treatment. No children had evidence of active TB disease or a CXR suggestive of other significant pathology. Of the children, 306 (89%) underwent finger-prick BBV screening and there were no positive results. Bacillus Calmette–Guérin (BCG) immunisation was offered to all those with no evidence of a BCG scar and in whom parents did not recall prior BCG vaccination; thus, 14 children subsequently received a BCG.
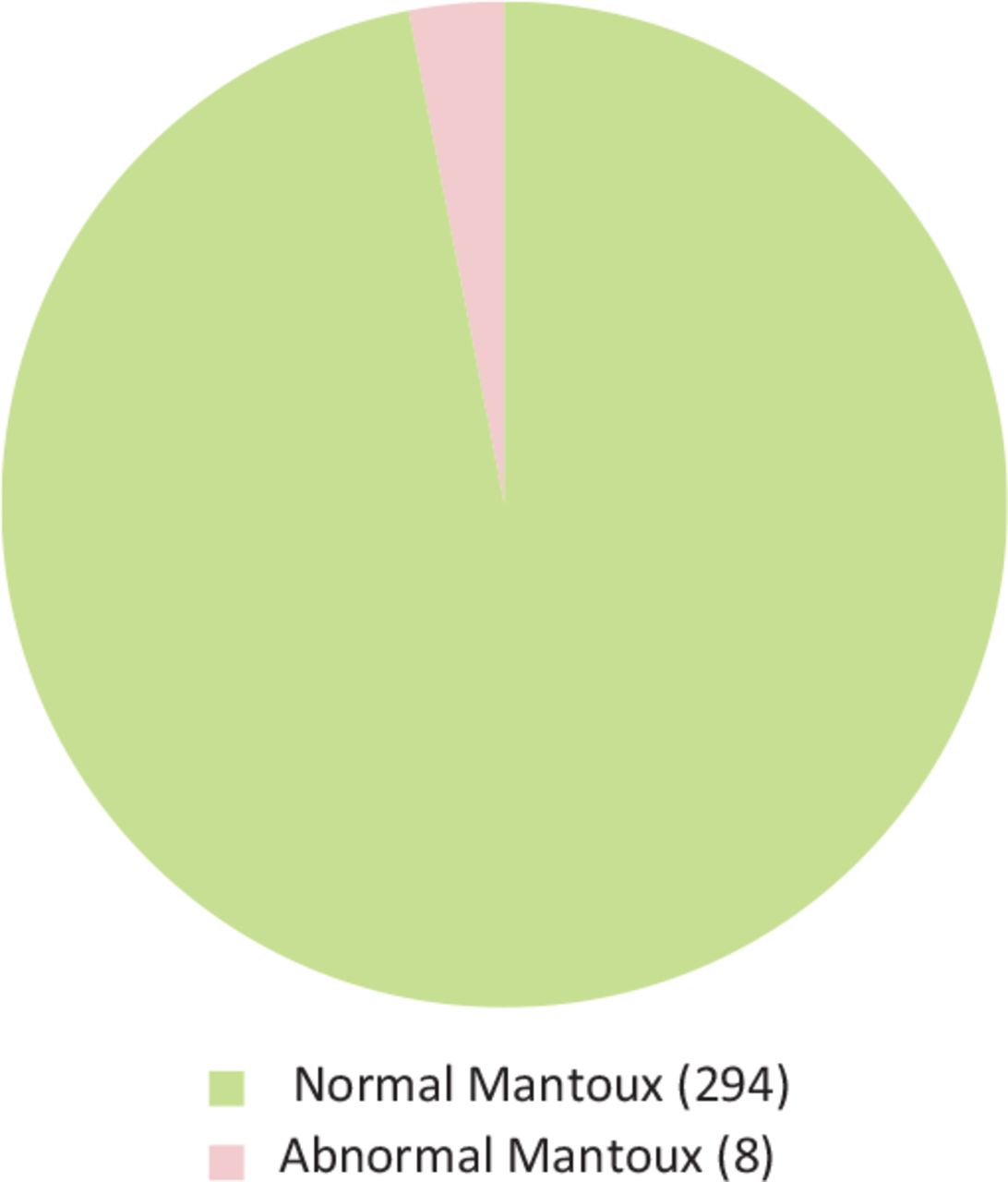
Paediatric Mantoux test results.

Paediatric latent tuberculosis infection (LTBI) screening results in 347 children.
Discussion
Only one case of active TB was identified in this refugee population from Afghanistan: a prevalence of 0.17%. An analysis of a German TB screening programme found two cases of active TB among 7,433 Afghan asylum seekers: a rate of 0.026%.9 A different meta-analysis of immigrant TB screening programmes around the world found an active TB prevalence of 0.28%.10
The same meta-analysis of studies reporting active TB rates in refugees and immigrants found a fourfold increase in cases of active TB in refugees compared with ‘planned’ immigrants.10 This was attributed to the fact that sudden unexpected events can lead a person to become a refugee, irrespective of their previous heath status, whereas immigration is more often planned if a person is healthy. Additionally, refugees often spend time in overcrowded camps, which would promote TB transmission. This was not the case for our population, which was evacuated directly from Kabul to hotels in Manchester. Afghans evacuated under the ARAP policy had worked with the UK Government and military as interpreters and in other roles in Afghanistan.11 TB is a disease of poverty and is associated with a low educational level. There were no data available on the educational status of the population evacuated under ARAP, but it could be presumed that they had a relatively high educational level given their work as interpreters and with government agencies. This could explain our finding of a 15% adult and 1.5% paediatric LTBI prevalence, which is lower than the global prevalence of 25%.
We faced several challenges and learned some key lessons while implementing this screening programme.
At the start of the screening programme, there was a lack of information regarding how many people had been relocated to Manchester and needed to be screened. This caused challenges with workforce and clinic planning. This improved with the employment of an operations manager at the hotels via the GP practice. The operations manager was a vital team member who coordinated the screening within the hotels and was a key link in communicating between the hotel and secondary care.
Significant language barriers were effectively overcome using face-to-face, but not telephone, interpreters. Although the participants themselves were generally very willing to take up offers of screening, there were a small number of families that persistently failed to attend. Some of these cultural obstacles were overcome by using female healthcare workers or by seeing women and children in their rooms.
Shortly after arriving in the UK, some members of our cohort were moved at short notice to various locations around the UK. This meant that some individuals missed their screening altogether and others were moved mid screening or before or during treatment. There was no communication from the UK Home Office to healthcare professionals before these moves; thus, we tried to ensure that results were communicated to patients in a timely manner as soon as they were available. It is notable that one-third of adults with LTBI were moved before they could be offered treatment. In these cases, we wrote to their new local TB team to ensure ongoing follow-up. However, moving to a different geographical area increases the risk of patients being lost to follow-up and not receiving LTBI treatment. Improved communication between the UK Home Office and healthcare professionals regarding upcoming moves might have allowed treatment to be started before the move occurred, improving the rate of LTBI treatment and ultimately reducing the risk of active TB cases developing.
The Trust was unable to accommodate the significant number of CXRs required; therefore, an external private provider was commissioned to perform and report the CXRs. There were delays in these CXRs and reports being uploaded to our Trust IT system, resulting in delays in them being reviewed and some children requiring repeat imaging. For future screening, we aim to use NHS radiology services so that images and reports are available in a timely manner. This will require additional workforce planning to ensure that radiology services can cope with this demand.
Guidance from NHS England recommended that all children over the age of 11 had a CXR to screen for active TB. After 56 paediatric CXRs were performed, all were normal. There was limited capacity for paediatric X-ray reporting and a high rate of non-attendance for CXRs because of children attending school. With agreement from the British Association for Paediatric Tuberculosis (BATB), we amended our protocol; children would only require a CXR if they were symptomatic or had a positive Mantoux result.
Early in the process, we identified the need for a database to track and organise results, as well as identify participants who had not attended for screening. Initially database management was undertaken by the clinicians; however, this process was refined and improved with the employment of a programme manager, collated and managed data from multiple sources. The programme manager also streamlined the development and running of the screening programme by coordinating multiple stakeholders to work together.
We had a high rate of engagement in the screening programme, and attribute this to the fact that screening appointments were offered in the hotel rather than in hospital, which made them much easier to attend. This was made possible because of rapid and collaborative teamwork between multiple stakeholders in primary and secondary care across several hospital sites. The on-site GP service included a dedicated GP and primary care manager, who provided holistic care to participants. They helped organise the screening and encouraged participants to attend. Primary care provision in the hotels was key to the success of the screening programme. Until now, new entrant TB screening has been provided in hospital clinics. There was a high rate of non-attendance at these clinics; in 2016–2019, only 42.6% of TB screening appointments offered at our Trust were attended. We had 10% rate of non-attendance at clinic for patients with proven LTBI. Although this is a low rate compared with our previous experience, these episodes of non-attendance might have been because these clinics were in hospital rather than at the hotel.
Undertaking this project has highlighted a large backlog of migrants and asylum seekers in Manchester who have not had the required TB screening. This has led us to review our previous ‘hospital-based’ approach to new entrant screening in Manchester with a move to delivering a more easily accessible, closer-to-home service in the future. This will be challenging because, compared with the ARAP population, who tend to stay months or weeks in the same bridging hotel, other asylum seekers are often moved rapidly and repeatedly around the country. The paediatric protocol is also being implemented in other bridging hotels in Greater Manchester and will be further developed to meet the more complex needs of children in asylum-seeker hotels.
Conclusion
We have described a successful active and latent TB screening programme in refugees relocated from Afghanistan within 3 months of arrival in the UK. One case of active TB was identified. There was a low LTBI rate of 15% in the adult population and 1.5% among the paediatric population. These patients were offered LTBI treatment to prevent reactivation to active TB disease.
We improved screening attendance rates from 42.6% at hospital-based appointments to more than 80% by implementing a hotel-based screening programme. This is possible to implement at short notice, although it is a complex process that requires close collaboration and detailed project planning between all stakeholders. Managerial oversight in both primary and secondary care is important to coordinate screening and collect data.
A CXR is not required for TB screening in children aged 11 or over, if they had no symptoms and a negative Mantoux test or IGRA. Our protocol was adapted to reflect this during the screening programme; this was discussed and agreed with BAPT.
Acknowledgements
The authors write on behalf of the ARAP TB screening MDT and would like to acknowledge the work of all members of this team, including, but not exclusively, Rochelle Baron, Joshua Bainbridge, Mandy Curran, Suzanne Dixon, Kenny Li, Ryan Noonan and Jenny White.
- © Royal College of Physicians 2023. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.