
Abstract
A 45-year-old woman presented to the hospital with bloody diarrhoea and significant weight loss over the past 1 month. On admission and evaluation, she was found to have acute ulcerative colitis. She was started on prednisolone and mesalamine therapy. Within 24 hours of initiation of this therapy, the patient complained of giddiness and chest discomfort and was found to have sinus bradycardia on ECG with no acute coronary event. After withdrawing mesalamine, her heart rate normalised within 24 hours and she remained symptom-free. This is a rare case report of severe symptomatic sinus bradycardia due to mesalamine therapy; to our knowledge, only four cases of mesalamine-induced bradycardia have been reported in the literature.
Introduction
Drug-induced bradycardia is a common side effect of several medications. Fortunately, symptomatic bradycardia caused by drugs is often reversible by simply withdrawing the culprit drug. The usual culprits are cardiac medications like calcium channel blockers, beta blockers, and other antiarrhythmics which cause bradycardia through known mechanisms affecting the cardiac electrical activity. Other non-cardiac drugs, such as phenytoin, tricyclic antidepressants and lithium, can also cause bradycardia. Sulfasalazine, the parent compound of all amino salicylates (ASAs), is used in the management of inflammatory bowel disease (IBD). Mesalamine, which is a sulpha-free 5-ASA, is used extensively in the treatment of IBD and is generally considered to be a safe and effective drug in the treatment of ulcerative colitis with headache, drug fever, rash, paradoxical disease exacerbation, pancreatitis, hepatitis, pericarditis, pneumonitis, and nephritis being reported with its use. Up to 45% of patients receiving 5-ASA compounds experience an adverse reaction to some degree.1 Bradycardia has rarely been reported as a side effect of mesalamine use, and to our knowledge there are only four case reports of bradycardia following mesalamine use in the literature. Here, we report a patient who developed symptomatic bradycardia after treatment with mesalamine.
Case report
A 45-year-old woman with diabetes was admitted to our hospital with complaints of bloody diarrhoea and significant weight loss over the past month. There was no significant past or family history of cardiac or gastrointestinal illnesses.
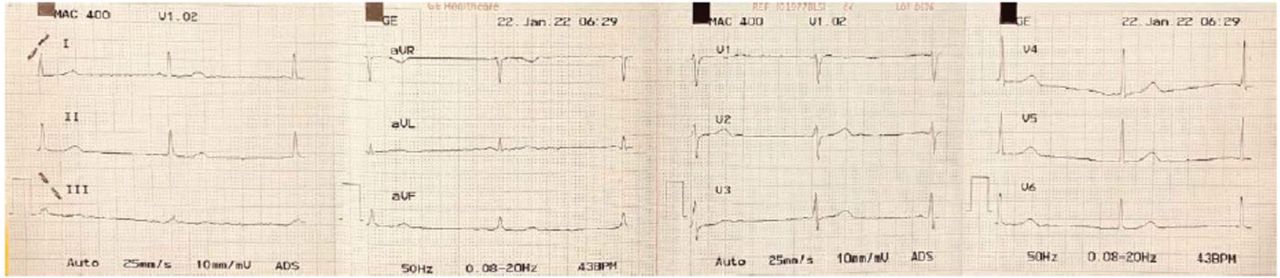
At presentation, heart rate was 110 beats per minute, temperature 36.8°C, blood pressure 120/86 mmHg and respiratory rate 18 cycles per minute. Per abdominal examination was unremarkable except for scar of abdominal hysterectomy. Routine blood work showed her haemoglobin was 13.4 g, erythrocyte sedimentation rate 56, and C-reactive protein 5.29 mg/dL. Stool routine was normal. Stool culture showed no growth. Contrast-enhanced CT abdomen showed mild circumferential rectal wall thickening (maximum thickness 5 mm) with perifocal fat stranding and perifocal lymphadenopathy suggestive of proctitis. A colonoscopy was done which showed ulcerative procto-sigmoiditis (Mayo endoscopic score 3). Colonic mucosal biopsy confirmed active ulcerative colitis, and the patient was initiated on IV hydrocortisone and oral mesalamine. However, within 24 hours of starting mesalamine, the patient complained of giddiness and chest discomfort. An ECG performed showed sinus bradycardia with a heart rate of around 40 beats per minute with no acute myocardial ischemia (Fig 1). Cardiology opinion was sought and work-up for bradycardia was performed. Her 2D echo was normal, as were cardiac enzymes, thyroid function tests and electrolytes including potassium, calcium, magnesium and phosphorus. Since the patient developed bradycardia after initiation of treatment for ulcerative colitis, mesalamine was considered as a probable cause for bradycardia and this was stopped. Her bradycardia resolved within 24 hours of stopping mesalamine and she remained asymptomatic throughout her hospital course (Fig 2). A rechallenge was not attempted due to possible serious cardiac adverse events. She was transitioned to oral steroids and given azathioprine on discharge.

ECG on mesalamine therapy.

ECG after stopping mesalamine therapy.
Discussion
Mesalamine is a sulpha-free 5 ASA preparation that is commonly used in clinical practice with a half-life of about 25 hours. Side effects of mesalamine include headache, arthralgia, nausea, vomiting, drug fever, rash, paradoxical disease exacerbation, pancreatitis, hepatitis, pericarditis, pneumonitis and nephritis. The mechanism of action is by inhibition of the activity of the nuclear factor-kappa B (NF-κB) pathway, inhibition of intestinal epithelial cell injury, inhibition of chemoattractant leukotrienes, and modulation of prostaglandin metabolism.2
Mesalamine-induced sinus bradycardia has been reported in four cases so far.3,4 In one case report, it was postulated to be due to an unrecognised unique predisposing factor like cardiac conduction abnormality unmasked by mesalamine use.2 One other case report postulated a modulating effect on prostaglandin metabolism as the pathologic mechanism of bradycardia.5 Another case report postulated mesalamine-induced myocarditis as the cause for bradycardia. However, there is inadequate evidence to identify the mechanism through which mesalamine causes bradycardia. Mesalamine is the cornerstone of ulcerative colitis treatment. In these patients, one must decide whether to discontinue the medication, reduce the dosage, or continue the same medication in the presence of symptomatic bradycardia. Such decisions are now made without knowledge of pathophysiology or natural history of mesalamine-induced bradycardia. Our case study highlights this gap in knowledge and need for further research into the pathophysiology and prognosis of mesalamine induced bradycardia.
Conclusion
Clinicians should be aware of this rare, albeit serious, adverse effect of mesalamine-induced bradycardia. Although the exact pathogenesis of this adverse effect is not known, further research is required to establish the mechanism, natural history, and prognosis of bradycardia in patients receiving mesalamine.
- © Royal College of Physicians 2023. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.