
Abstract
Aims The study tests the hypothesis that a higher acute systemic inflammatory response was associated with a larger decrease in blood hemoglobin levels in patients with Coronavirus 2019 (COVID-19) infection.
Methods All patients with either suspected or confirmed COVID-19 infection admitted to a busy UK hospital from February 2020 to December 2021 provided data for analysis. The exposure of interest was maximal serum C-reactive protein (CRP) level after COVID-19 during the same admission.
Results A maximal serum CRP >175mg/L was associated with a decrease in blood haemoglobin (−5.0 g/L, 95% confidence interval: −5.9 to −4.2) after adjustment for covariates, including the number of times blood was drawn for analysis.
Clinically, for a 55-year-old male patient with a maximum haemoglobin of 150 g/L who was admitted for a 28-day admission, a peak CRP >175 mg/L would be associated with an 11 g/L decrease in blood haemoglobin, compared with only 6 g/L if the maximal CRP was <4 mg/L.
Conclusions A higher acute systemic inflammatory response is associated with larger decreases in blood haemoglobin levels in patients with COVID-19. This represents an example of anaemia of acute inflammation, and a potential mechanism by which severe disease can increase morbidity and mortality.
The chronic anaemia of inflammation is well recognised1 and is observed in a range of diseases associated with higher systemic inflammation, including chronic infections, such as tuberculosis,2 and non-infectious diseases, such as rheumatoid arthritis.3,4 The precise biological mechanism by which chronic inflammation can decrease blood haemoglobin is not fully understood, but might involve suppression of the haematopoietic production of new red blood cells in the bone marrow, possibly along with a modest reduction in the survival of red blood cells.1
Given that the chronic anaemia of inflammation is observed in a wide range of infectious and non-infectious diseases, the common pathway appears to be through the systemic inflammatory response rather than being specific to individual diseases. The time course of this phenomenon is unknown, but it is possible that the same biological process occurs in the context of acute inflammation.
Thus, we tested the hypothesis that higher levels of systemic inflammation are associated with larger decreases in blood haemoglobin in patients admitted to a single UK teaching hospital with Coronavirus 2019 (COVID-19) infection.
Methods
Study population
The study population comprised consecutive unselected patients admitted to Nottingham University Hospitals NHS Trust between 1 February 2020 and 31 December 2021 with either suspected or microbiologically confirmed COVID-19 infection who were eventually discharged from hospital.5
Data collection
From routinely collected electronic data, all venous haemoglobin and C-reactive protein (CRP) laboratory measurements within the first 30 days of each admission were extracted. The timing of the blood test was defined as the number of days from the admission date.
Statistical analysis
We assessed whether the peak level of inflammation, as measured by the highest serum CRP measurement during the admission period, predicted the overall change in haemoglobin across each hospital admission. For each patient's admission, the following summary measures were calculated: maximum serum CRP (mg/L) during the admission period; length of stay (days); mean baseline blood haemoglobin (g/L); the fall in haemoglobin (g/L) during the admission period; age; and sex. The total number of unique dates and times that blood tests were taken during each admission was also calculated (N). Therefore, multiple blood tests at a single timepoint were only counted as one blood test draw.
The change in haemoglobin was defined as the difference between the baseline haemoglobin measurement on admission and the last measurement before discharge from hospital. The maximum serum CRP for each admission was categorised into quartiles, and this was used to tabulate each summary measure.
A linear regression model was then used to predict the association between the maximum serum CRP as a continuous variable with the decrease in haemoglobin during the admission, adjusted for age, sex and length of stay. This was tested for a departure from the linear trend by fitting CRP categorised into frequency deciles and comparing this nested model with a generalised likelihood ratio test, to determine the optimal analytical modelling approach. Finally, because length of stay was likely to be correlated with the total number of blood tests, we assessed the total number of blood tests and length of stay both separately in different regression models and together with their calculated generalised variance inflation factor (VIF)6 to check the potential impact of co-linearity on the stability of the model. The final model adjusted for both length of stay and the number of blood tests as covariates to explore the associations of interest adjusted for both factors.
Ethical approval
Approval for this work was granted via a Nottingham University Hospital (NUH) Clinical Effectiveness Team audit (reference: 21-294C) and the Integrated Research Application System (IRAS) (REC: 20/WM/0142, project ID: 282490, amendment No. SA02 20/07/21).
Results
There were 10,722 admissions among 4,201 patients suspected of COVID-19 infection available for analysis who survived to be discharged from hospital. Patients who had a higher maximal serum CRP measurement had a lower baseline mean haemoglobin, higher decreases in blood haemoglobin, longer lengths of stay and more blood draws/days (Table 1).
Description of the study population
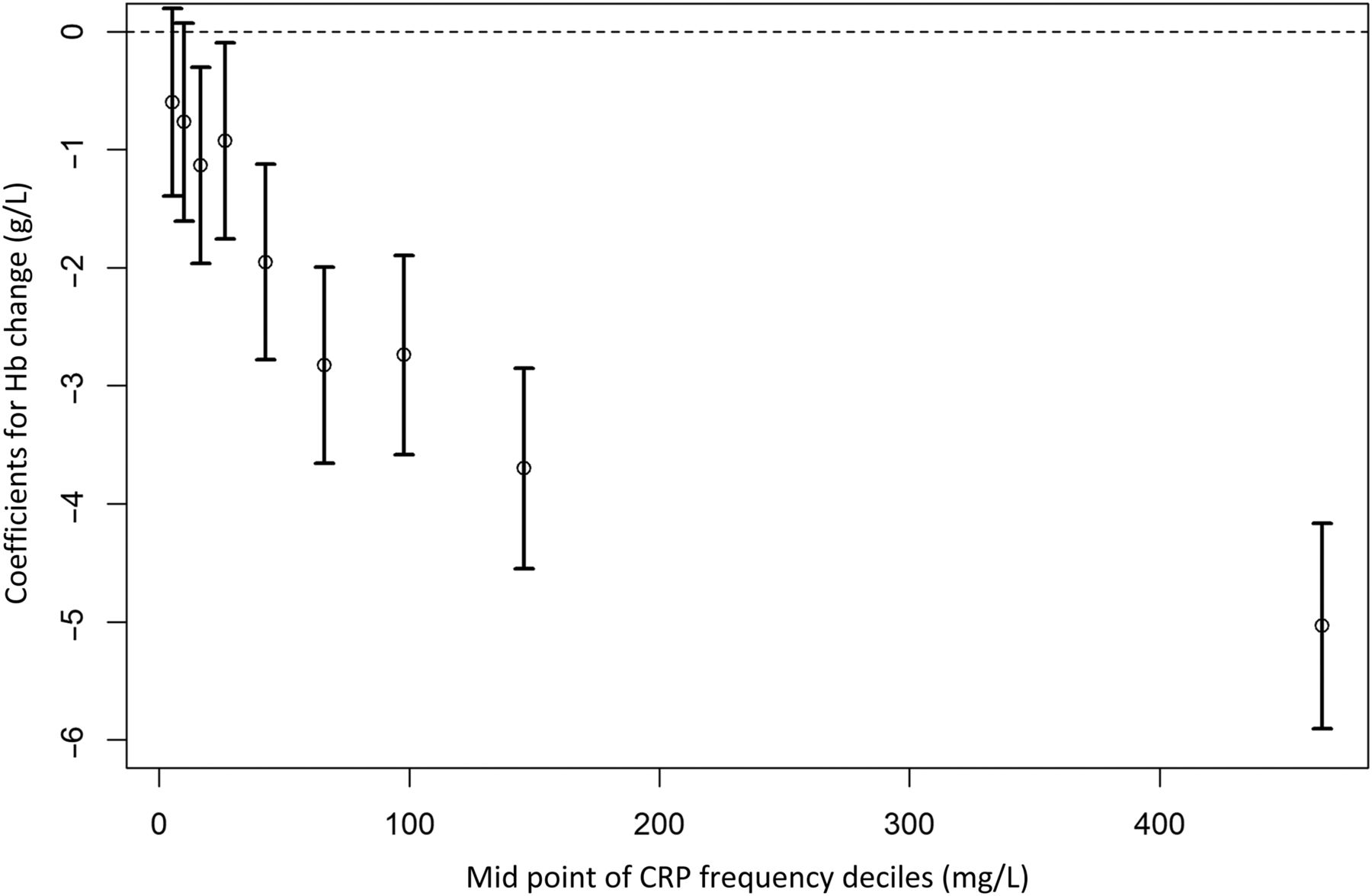
The change in haemoglobin during an admission versus peak serum C-reactive protein (CRP) categorised into deciles. Coefficients for additional haemoglobin (Hb) change for each CRP decile adjusted for length of stay, blood draws, baseline Hb, age and sex. Dashed line indicates the reference category for CRP decile between 0 and 3.5 mg/L. Data are estimates with 95% confidence intervals.
Therefore, three linear regression models were fitted, with serum CRP categorised into deciles based on their frequencies (Table 2). The first model was the association between maximal serum CRP and acute decrease in haemoglobin over the period of the admission. A serum CRP between 4.5 and 7 mg/L was associated with a ∢0.6 g/L (95% confidence interval (CI): −1.4 to −0.2) decrease in haemoglobin during admission after adjustment for age, sex, peak haemoglobin and length of stay. This fall in serum CRP increased almost 10-fold for CRP over 175 mg/L to −5.8g/L (95% CI: −6.7 to −4.9).
Association between maximal C-reactive protein and change in haemoglobin in patients admitted with COVID-19 infectiona
The total count of blood tests was correlated with the length of the admission (r=0.96, p<0.0001, Spearman correlation coefficient) and a generalised VIF of 3.3. Therefore, a separate regression model replaced the total count of blood tests for the length of stay co-variate. Adjusting for the total number of blood draws reduced the fall in haemoglobin for the highest serum CRP decile with a haemoglobin fall of −5.0 g/L (95% CI: −5.9 to −4.2) for a peak CRP >175 mg/L (Fig 1).
A final regression model that included both length of stay and the total blood test count did not substantially change this association between peak CRP and fall in haemoglobin, with a haemoglobin fall of 5.0 g/L (95% CI: −5.9 to −4.2) for a peak CRP >175 mg/L.
Using the final model with length of stay and number of blood draws, for a 55-year-old male patient with a maximum haemoglobin of 150 g/L, a 28-day admission, two blood tests a day, a peak CRP of over 175 mg/L predicted a 11.0 g/L drop in haemoglobin, compared with only a 6.0 g/L drop if the maximal CRP was <4 mg/L.
The number of times blood was collected for analytical testing was also an independent risk factor for a decrease in haemoglobin (−0.05 g/L per blood collection, 95% CI: −0.06 to −0.04).
Discussion
This is the first analysis to demonstrate that higher levels of systemic inflammation are associated with decreases in blood haemoglobin in the context of patients with acute infection with COVID-19. The mean decrease in blood haemoglobin of ∼11 g/L in the patients with a maximum serum CRP >175 g/L suggests that this observation is clinically important as well as potentially enhancing our understanding of the host response to a high level of acute systemic inflammation.
The strengths of these data are that they are from a complete prospectively collected dataset of all admissions with confirmed or suspected COVID-19 infection over a specified period, thus allowing the hypothesis, that higher systemic inflammation is associated with acute decreases in blood haemoglobin, to be tested in a population with the same microbial cause of infection. Unsurprisingly, there was co-linearity between length of stay and the number of blood tests; thus, we adopted a conservative statistical modelling strategy, adding both of these individually to separate models. However, the generalised VIF of 3.3 for including number of blood tests in the model with length of stay was below the generally accepted threshold (<5); thus, the impact of this co-linearity on the model precision was not excessive.7 Given that it is important to distinguish between decreases in blood haemoglobin that are associated with maximal serum CRP and those that are a result of a higher number of blood samples taken for analysis, a third regression model, which included both length of stay and the number of blood tests, was analysed. This demonstrated that the inverse association between systemic inflammation and the change in blood haemoglobin levels persisted after correction for the number of times blood samples were drawn, although this was also an independent risk factor for decrease in blood haemoglobin.
The limitations of the analysis include the issue that these are observational data and, hence, a causal association between systemic inflammation and acute decreases in blood haemoglobin cannot be conclusively demonstrated. However, our study design is probably the optimal option to test the hypothesis that higher levels of systemic inflammation are associated with larger acute decreases in blood haemoglobin levels in humans. Serum CRP can be regarded as a biomarker of systemic inflammation and disease severity, and it is likely that biological pathways associated with these processes lead to decreases in blood haemoglobin. It is important to emphasise that we observed decreases in blood haemoglobin in association with higher levels of systemic inflammation in a single disease model (COVID-19 infection) and that this observation cannot be generalised to other causes of acute inflammation without validation from appropriately designed studies.
The clinical implications of an acute drop in blood haemoglobin associated with higher levels of systemic inflammation associated with COVID-19 infection are manifold. Patients with COVID-19 with higher serum CRP levels are known to have a worse prognosis compared with those with lower levels,8 and, because treatment with dexamethasone is associated with lower maximal serum CRP in patients with COVID-19,9 systemic inflammation might be one of the biological processes that contributes to this increase in mortality. The observation that the use of anti-inflammatory therapeutic medication, such as dexamethasone, reduces mortality in patients with COVID-19 infection10 with a dose response to the clinical benefit11 suggests that the acute host inflammatory response is an important determinate of outcome in this disease, and that some of this effect is mediated by reducing systemic inflammation rather than by simply treating inflammation in the lungs alone. The current threshold for starting dexamethasone therapy for patients with COVID-19 is in the context of pulmonary disease requiring oxygen,10 but future use of dexamethasone and other anti-inflammatory treatments for COVID-19 could consider titrating the dose and duration of corticosteroid treatment against the systemic inflammatory response.
The exact mechanism of how a large systemic inflammatory response is associated with an acute decrease in blood haemoglobin remains speculative. It is likely to be similar to that observed in the anaemia of chronic inflammation, which is generally considered to be a reduction in haematopoiesis along with reduced red blood cell survival.1 In chronic inflammation, erythropoiesis is limited by hypoferraemia and cytokines acting on erythroid progenitors, whereas erythrocyte lifespan is shortened by phagocytosis resulting from cytokine active macrophages.12 Hepcidin, a peptide that is part of the innate immune system, appears to have a key role in iron metabolism by blocking iron absorption and macrophage iron recycling, resulting in lower blood haemoglobin levels.13 This process is activated by inflammatory pathways, and higher serum hepcidin levels were observed in patients with COVID-19 compared with control patients without COVID-19.14 Hence, this might be an area for future investigation for studies investigating the interactions and causal processes that determine the relationships between inflammatory pathways and anaemia in the context of COVID-19.
This is an important area for future study, because understanding the biological pathways involved is likely to lead to new therapeutic options to protect red blood cell production in patients with higher levels of systemic inflammation from COVID-19 and possibly other diseases. This might be of particular potential use in the context of intensive care units, where a 98% prevalence of anaemia has been reported,15 which was not related to phlebotomy practices.
Conclusions
These data demonstrate that, in patients with COVID-19, higher levels of systemic inflammation are associated with larger decreases in blood haemoglobin. This contributes to our understanding of the extrapulmonary effects of COVID-19 and introduces the option of targeting novel biological pathways to help preserve red blood cell production in patients with severe COVID-19 infection.
- © Royal College of Physicians 2023. All rights reserved.








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.