
Pleural effusion is a common clinical problem and may present to a wide range of specialties. Accurate aetiological diagnosis is key to subsequent management, requiring a multidisciplinary approach and knowledge of the correct investigation pathway. This article will focus on appropriate staged investigations for the patient presenting with pleural effusion rather than on its causes or treatment.
Clinical syndromes
Pleural effusion is often detected on plain chest radiography as an incidental finding and patients may be asymptomatic. Clinical symptoms are variable, depending on the size and aetiology of the effusion and rarely specific enough to suggest a diagnosis in the absence of further investigations. Large effusions are likely to be associated with dyspnoea, but this is often a late finding and oxygen saturations may not be severely lowered. Dyspnoea is the result of impaired mechanics and increased intrapleural pressure swings.
The presence of chest pain implies involvement of the parietal pleura which is heavily innervated. Inflammation, infection and malignant involvement may produce pain, including shoulder tip symptoms associated with diaphragmatic involvement. Weight loss, anorexia and malaise may imply malignancy or infection (eg empyema).
Causes
Pleural effusions are divided into transudative and exudative (Table 1). They are diagnosed according to pleural fluid biochemical characteristics (see below). However, transudates occur with structurally normal pleura, in which oncotic or hydrostatic pressure results in fluid leak. In contrast, exudates occur with damaged or altered pleura, resulting in loss of tissue fluid and protein causing fluid formation.1
Causes of exudative and transudative effusions and biochemical parameters.
Differentiation of transudate from exudate is key to further management. Treatment for transudative effusion relies on treatment of the underlying disease, and uncommonly requires specific pleural intervention. In contrast, exudative effusion usually needs further investigation and often requires intervention.
Initial diagnostic approach
The presence of bilateral, symmetrical effusions in the appropriate clinical context is highly suggestive of transudative effusion, and in general requires no further investigation.2 However, it should be noted that about 50% of heart failure effusions are unilateral and where bilateral may be larger on one side.3 In this circumstance or if the clinical course is atypical (eg lack of response to therapy), further investigations should be considered.
Key Points
Unilateral pleural effusion requires further aetiological investigation, with pleural fluid analysis as the usual first investigative step
All effusions in the context of pneumonic illness should be sampled to assess for the presence of complicated parapneumonic effusion (pH < 7.2) or empyema (frank pus)
Ultrasound is a far more sensitive technique for the diagnosis of pleural effusion than chest radiography. In cases where initial ‘blind’ aspiration has failed, or in the presence of an anatomically complex collection, image guidance (ultrasound or computed tomography) should be sought
Drainage of undiagnosed pleural effusions ‘to dryness’ is not recommended, as this makes further investigation techniques more difficult. In the case of a breathless patient, removal of 1–1.5 litres of pleural fluid will usually alleviate symptoms
Pleural fluid cytology is positive in only 60% of malignant pleural effusions. A negative fluid cytology in the absence of another clear cause for pleural effusion should prompt further investigations via a respiratory specialist
Unilateral effusions require further assessment. The initial investigation of choice is diagnostic pleural aspiration. Large effusions (> 1/2; hemithorax volume) may be aspirated easily without image guidance, but in the presence of a small effusion, or where initial ‘blind’ aspiration is unsuccessful, image guidance (usually ultrasound) should be sought. In the absence of a diagnosis (unless clearly infected), intercostal drain insertion and complete drainage of the chest is not recommended as this makes more difficult any further investigations that may be required. In symptomatic breathlessness with large effusions, large volume (eg 1 litre) thoracentesis for diagnostic/therapeutic purposes is usually sufficient to control symptoms until initial investigation results are obtained. These patients can in general be investigated in the outpatient setting.
Pleural fluid diagnostic tests
Appearance
Frankly purulent pleural fluid is diagnostic of empyema; it may also be malodorous. Turbid pleural fluid may be seen in infected pleural effusion or in oesophageal perforation. ‘Milky’ pleural fluid should prompt consideration of empyema or a lipid abnormality.
Biochemical parameters
Fluid should be sent in all cases for measurement of:
protein level
lactate dehydrogenase (LDH), and
glucose.
These parameters allow reliable differentiation of exudate from transudate by applying Light's criteria4 (for which simultaneous sampling of venous blood for protein and LDH is required) (Table 1). Pleural fluid pH measurement is recommended in cases of suspected infected pleural effusion (see below).
Special tests
Guidelines recommend biochemical analysis of pleural fluid in all sampled effusions as above, with microbiology (including specific requests for staining and culture of acid-fast bacilli) and cytology where indicated.5 Certain more specific tests should be undertaken, dictated by clinical circumstances, for example:
amylase in suspected oesophageal perforation or pancreatitis-associated effusion, or
lipid profile in suspected chylothorax or pseudochylothorax.
Pleural fluid autoantibody level measurement (eg antinuclear antibodies, rheumatoid factor) are representative of serum levels and add little diagnostic value.
Radiological investigations
Most pleural effusions are detected on plain chest radiography, although lateral (and specifically lateral decubitus) radiographs increase sensitivity. About 200 ml of pleural fluid must be present before any change is evident on the plain posteroanterior (PA) chest radiograph.6 The classical appearance of pleural effusion is easily recognised. However, loculated fluid may appear atypically and encysted fluid within the lung fissure may give the appearance of an intraparenchymal mass (Fig 1).

Encysted fluid in the fissure appearing as a lung mass.
Thoracic ultrasound
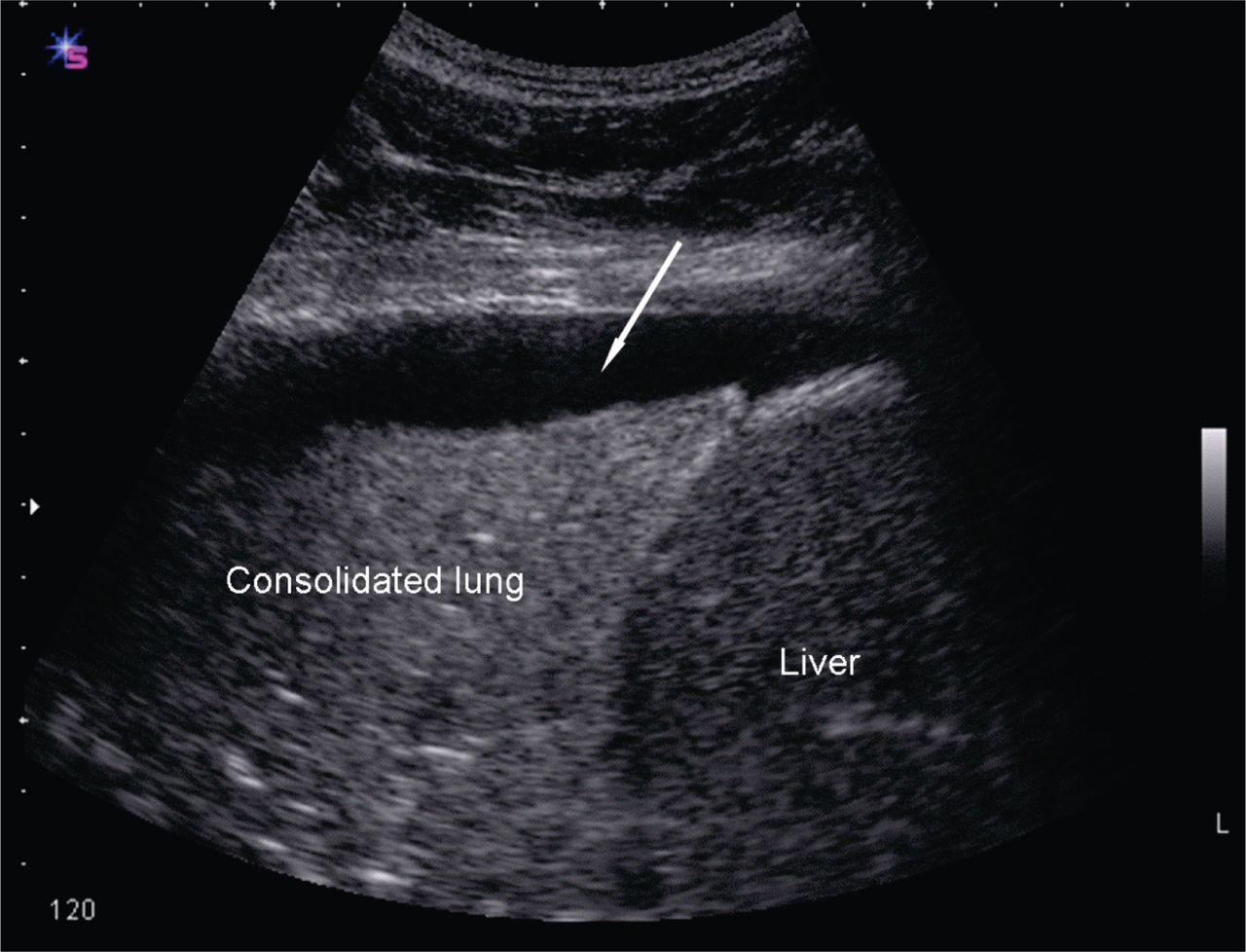
Lateral decubitus chest radiography has largely been superseded by thoracic ultrasound, which is more widely available and increasingly being performed by physicians on the ward. It permits detection of very small amounts of pleural fluid. Several studies have demonstrated that it is more sensitive in detecting fluid, more accurate in guiding aspiration and safer than ‘blind’ procedures (Fig 2).7 A recent National Patient Safety Audit committee report8 detailing 12 deaths due to malposition of chest drains suggests that drains should be placed with ultrasound guidance wherever possible, always by an operator with adequate competence in both drain insertion technique and ultrasound.
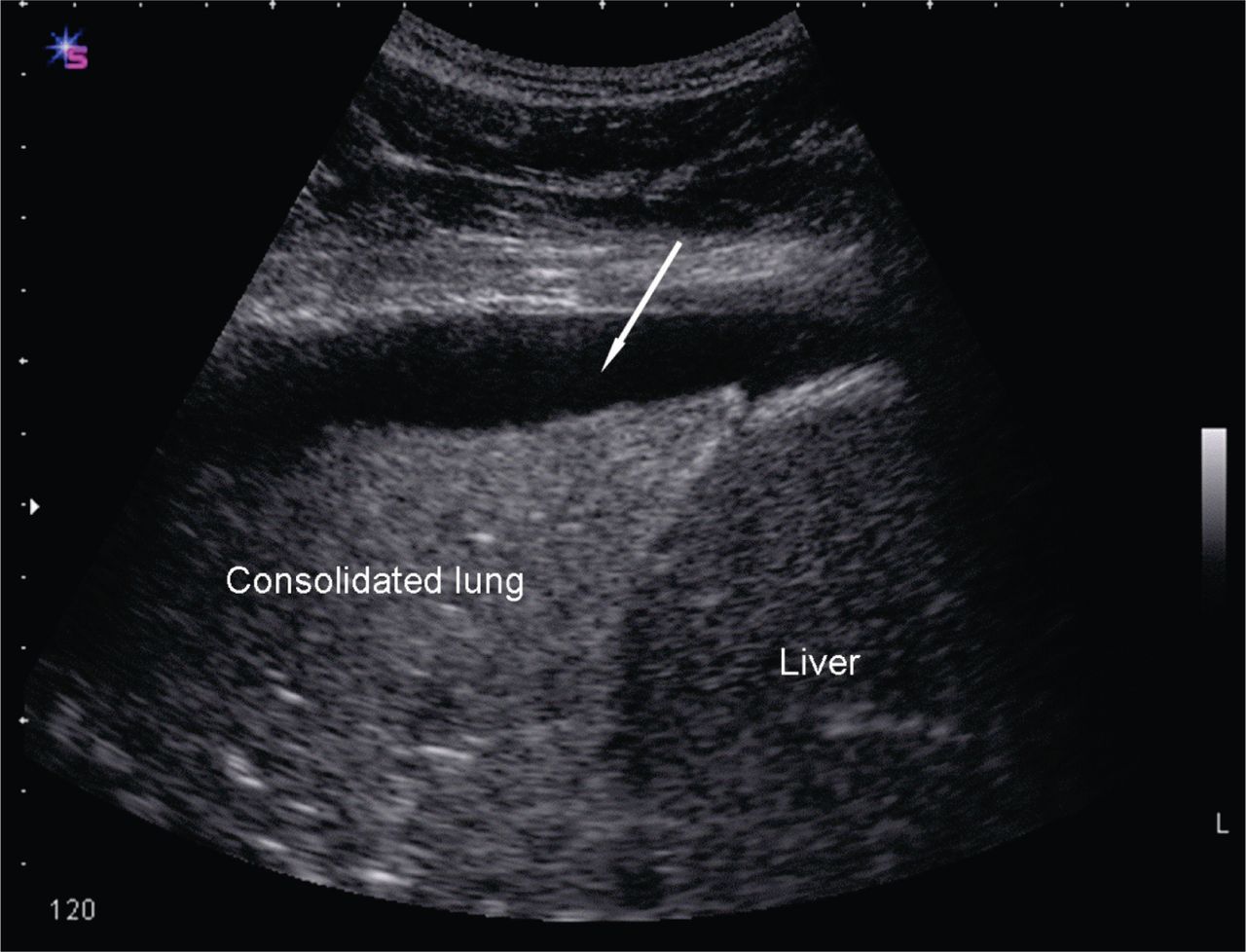
Thoracic ultrasound demonstrating consolidated lung and a very small parapneumonic effusion (arrow) about 1.5 cm deep. The chest radiograph showed basal consolidation only.
Contrast-enhanced computed tomography
A powerful tool in the diagnosis of pleural effusion is contrast-enhanced computed tomography (CT).9 The technique is most valuable when:
there remains a substantial effusion because it improves the contrast between pleural abnormality and fluid, and
the scan is conducted in the late venous phase (ie 60–90 seconds after injection), permitting enhancement of the pleural surfaces.
CT permits assessment of the underlying lung parenchyma, mediastinal structures and associated liver and upper abdominal pathology.5
Specific circumstances
Infective pleural effusion
A pleural effusion occurs in about 50% of cases of pneumonia.10 Most of them require no specific treatment, but it is mandatory to sample all but the smallest effusions as no clinical parameters are able to predict which patients will require more aggressive therapy.11 In cases of doubt, ultrasound or CT scanning should be requested to assess for possible effusion.
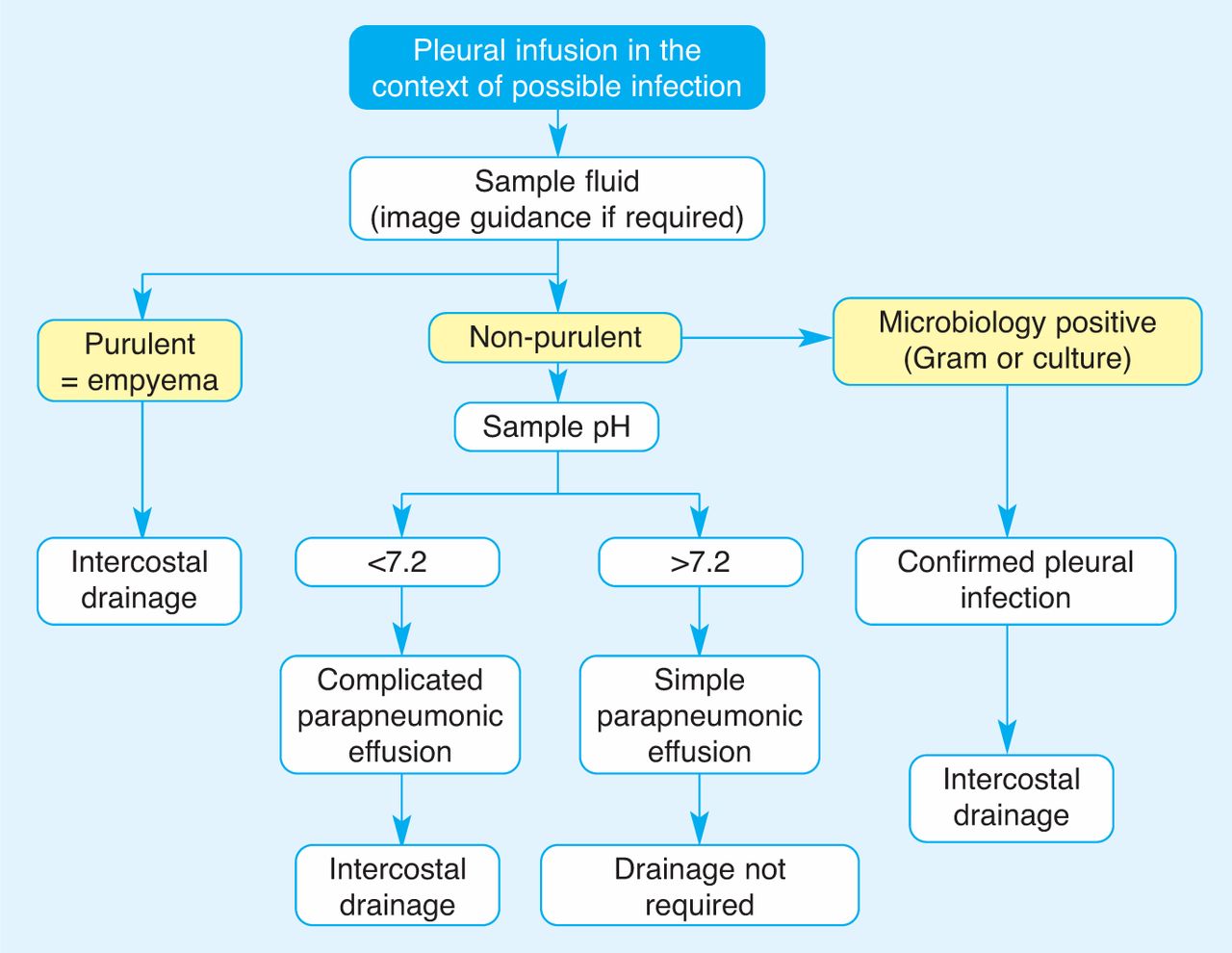
A suggested diagnostic algorithm for suspected infected pleural infection is shown in Fig 3.10 A combination of pleural fluid appearance, pH and microbiological analysis is required to assess the need for intercostal drainage. Frankly purulent fluid is diagnostic of empyema (pleural fluid pH is not required in this circumstance). In cases of non-purulent fluid in the context of an infective illness, accurate pleural fluid pH guides further management. Meta-analysis has demonstrated that acidic pH (<7.2) is associated with a ‘complicated’ clinical course and hence requires chest drainage.12 In contrast, non-acidic pH is associated with an uncomplicated course and therefore appropriate antibiotic treatment for the pneumonia alone is usually sufficient.

Investigation pathway for suspected infected pleural effusion.
Although pH is a sensitive and specific marker of patients requiring intercostal drainage, decisions to initiate drainage must not be based solely on pH. Repeat sampling should be considered in non-acidic effusion if there is clinical deterioration. It should also be noted that a number of conditions (which do not mandate prompt intercostal drainage) may result in a low pleural fluid pH, including tuberculous pleural effusion, rheumatoid arthritis, oesophageal perforation and some malignant pleural effusions.13
Recent data demonstrate that accurate pleural fluid pH measurement requires analysis by blood gas analyser (not litmus paper) within one hour of collection, with care taken to exclude all heparin, local anaesthetic and air from the sampling syringe.14 If pleural fluid is Gram- or culture-positive, intercostal drainage is required regardless of pleural fluid appearance and pH.
Even with frankly purulent fluid, microbiological analysis will be positive in only about 60% of cases.15 Therefore, a substantial number of patients will require empirical antibiotic regimens for the duration of treatment (Table 2).10
Causative organisms and suggested empirical antibiotic regimens for pleural infection.
Malignant pleural effusion
Accurate diagnosis of tissue type is essential in further management of malignant pleural effusion. Although its presence (in non-mesothelioma) implies metastatic disease most commonly from lung, breast, bowel and lymphoma,16 the advent of more focused oncological therapies means that accurate diagnosis often alters management or provides prognostic information.
Cytological analysis
Pleural fluid should be sent for cytological analysis on diagnostic aspiration. A small amount (10 ml) is sufficient in most circumstances, although local pathology preferences should be checked. Even with the use of modern immunostaining techniques, pleural fluid cytology has a diagnostic sensitivity of only 60% and a substantially lower sensitivity (ca 20%) in mesothelioma.16 A second, separate pleural fluid aspirate increases diagnostic yield modestly (by ca 10%), but there is no further increase with a third sample.17 About 40% of cases of pleural malignancy will therefore remain undiagnosed after cytological sampling. Further tests are needed in this patient group.
Contrast-enhanced computed tomography
The next step is often contrast-enhanced CT which has a sensitivity of 90% for malignant pleural disease.9 Pleural tissue will be required for definitive diagnosis. The most widely available technique is ‘blind’ pleural biopsy (eg Abram's or Cope's needle) in which pleural tissue is obtained without image guidance. However, this technique provides only an additional 20% diagnostic sensitivity and substantially less in mesothelioma.
Pleural biopsy under image guidance
Pleural biopsy performed under image guidance (in general CT) was superior to ‘blind’ pleural biopsy in a randomised trial.18 The diagnostic yield of CT-guided biopsy approaches 90% in cytology negative cases.18 An alternative approach is local anaesthetic or ‘physician-based’ thoracoscopy in which endoscopes are entered into the pleural space under sedation and local anaesthesia. This procedure permits full drainage of the pleural space, pleural biopsy and, if required, therapy for recurrent effusion (talc poudrage pleurodesis) in the same sitting. There are no randomised trials of the diagnostic yield of thoracoscopy but large cohort studies suggest a sensitivity for malignancy in excess of 90%.19 CT-guided and thoracoscopic techniques are complementary, in that large effusions can be diagnosed and treated simultaneously using thoracoscopy, whereas smaller effusions can be safely diagnosed using CT-guided biopsy.
- © 2009 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}