
Abstract
Significant hypercalcaemia can cause electrocardiogram (ECG) changes mimicking an acute myocardial infarction. It is important to recognise that some ECG changes are due to conditions other than cardiac disease so that appropriate treatment is given, and importantly, inappropriate treatments are avoided.
Lesson
A 69-year-old woman presented to the accident and emergency department with an electrocardiogram (ECG) showing anterior ST segment elevation. She was found collapsed at home two hours prior to presentation with vague chest pain, lethargy and being non-specifically unwell. Little history was available from the patient due to consciousness level and a weak voice. Past medical history included ischaemic heart disease, previous coronary angioplasty, left ventricular failure, hypertension, hypercholestrolaemia and ongoing investigation of a thyroid goitre.
On examination she looked unwell, dehydrated, frail but haemodynamically stable. She was not sweaty, clammy or in pain. Cardiovascular system examination was unremarkable. Her initial ECG showed widespread ST segment elevation in leads V1 to V5, Q waves and poor R wave progression in inferior leads (Fig 1). She received thrombolysis on the basis of a significant cardiac history, and significant ECG changes associated with collapse.

Electrocardiogram on admission.
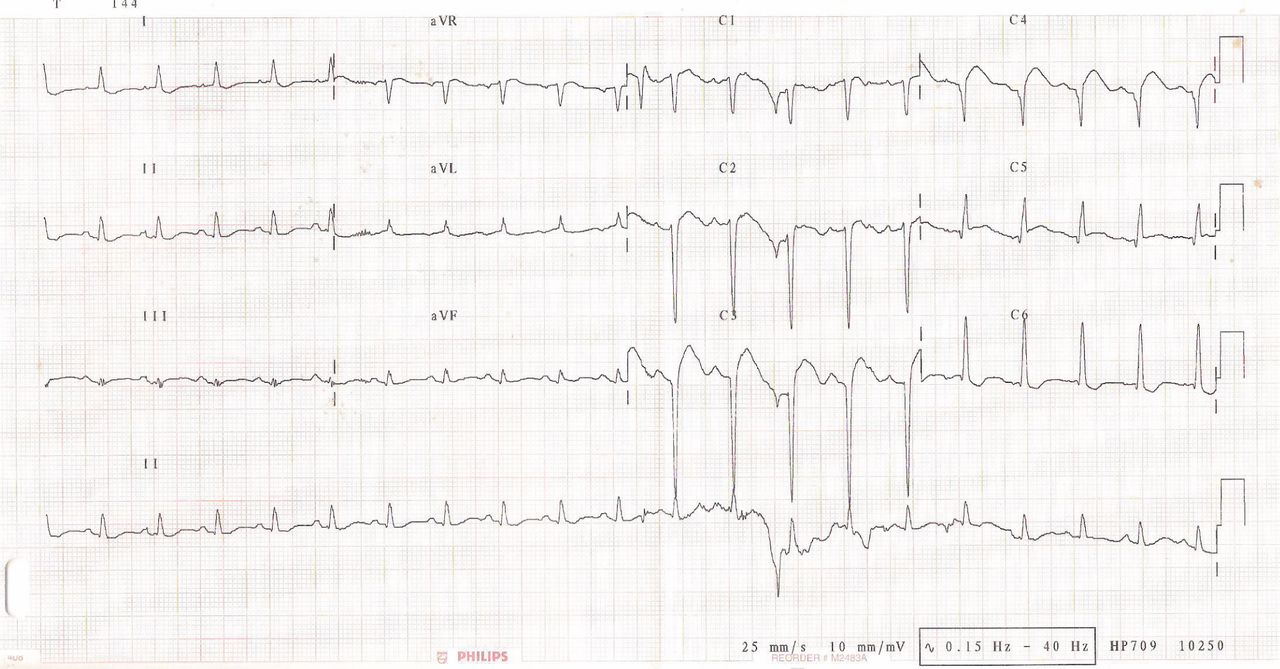
Subsequently, total creatinine kinase and troponin T values were found not to be elevated, but her corrected calcium was later found to be elevated at 5.09 mmol/l. A thyroid gland biopsy result, taken two weeks previously, revealed disseminated thyroid cancer. She rapidly deteriorated despite aggressive resuscitation and died within 36 hours of presentation with refractory hypercalcaemia. No evolutionary changes typical for ST elevation myocardial infarction (MI) were seen (Fig 2). Retrospectively, she was profoundly unwell from hypercalcaemia due to a primary thyroid malignancy on presentation, but treatment was distracted by the dramatic and unexplained ECG.
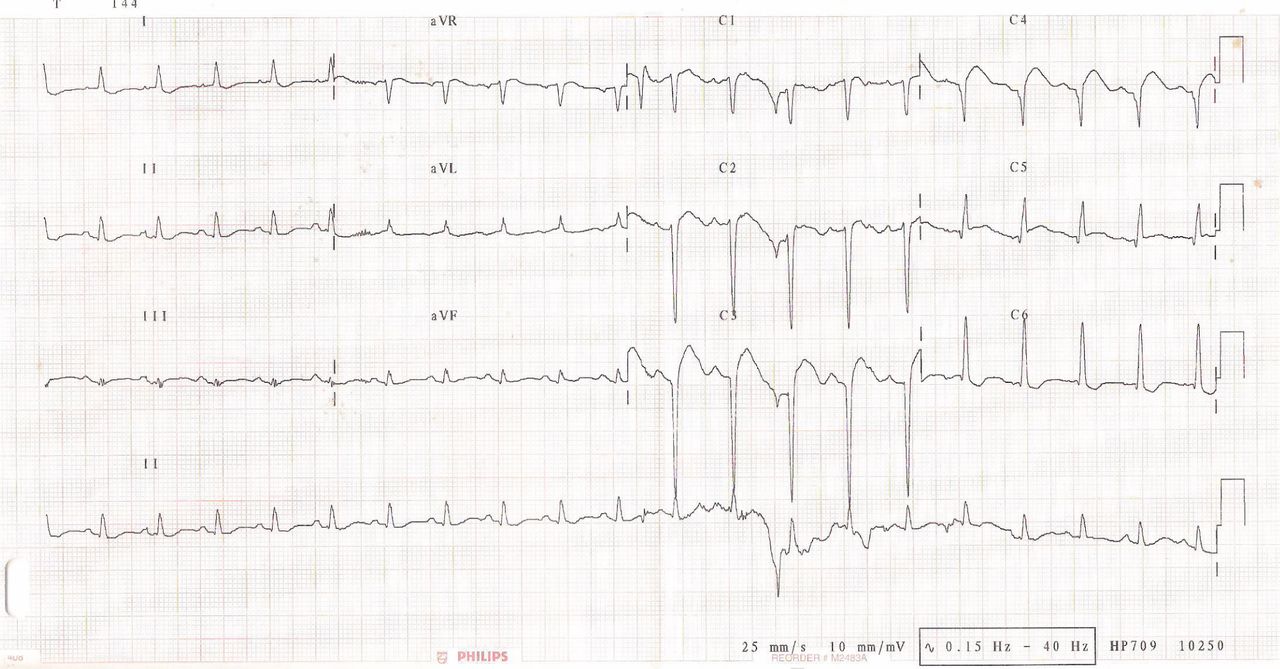
Electrocardiogram pre-terminal.
Discussion
We are aware of only two cases of hypercalcaemia causing ECG changes mimicking acute MI.1,2 The first case was due to hyperparathyroidism, and the second due to vitamin D intoxication. There is also one case, in a series of 161 fatal thyroid carcinoma cases, where the patient died of hypercalcaemia, while another nine cases had hypercalcaemia per se.3 In this series it states that malignancy associated hypercalcaemia can be due to humoral (PTH driven) hypercalcaemia or bone metastases. In this patient hypercalcaemia could be due to either mechanism.
The mechanism of how hypercalcaemia causes ST elevation is not understood, but presumably has a basis in ion concentrations mediating abnormalities in myocardial membrane potentials. To function correctly, individual myocardial cells rely on normal concentrations of biochemical parameters. Classically hypercalcaemia increases myocardial contractility and irratibility. Classical ECG features of hypercalcaemia are absent or shortened ST segment, shortened QT but lengthened T wave duration. It is hoped that this lesson with increase awareness that hypercalcaemia can also cause ECG changes mimicking acute MI. It is important to recognise that some ECG changes are due to conditions other than cardiac disease so that appropriate treatment is given early, and inappropriate thrombolysis avoided.
- © 2009 Royal College of Physicians








{kind=link}
{kind=link}