
Abstract
The aim of this study was to analyse tuberculosis (TB) risk assessment for rheumatology patients commencing anti-tumour necrosis factor-α (anti-TNF-α) therapy using the British Thoracic Society (BTS) guidelines. Data were obtained retrospectively on 856 outpatients regionally receiving anti-TNF-α. Prior to commencing treatment, patients had the following assessments documented: respiratory examination, 47.4%; chest X-ray, 84.5%; TB history, 92.9%; and advice about TB risk, 45.8%. Of the 856 patients, 94.3% were on immunosuppressives but 27% had a tuberculin test; 12.6% had ≥1 high-risk factors for TB. In total, 3.4% were referred to a TB specialist and of these, 24.1% had no risk factors for TB. Of patients with ≥1 risk factor, 76.9% were not referred. Only 4/28 patients at high risk for TB due to ethnicity or birthplace received chemoprophylaxis. Marked inter-unit variation was demonstrated and it was evident that patients require improved screening for TB. Greater awareness is necessary of patients with risk factors, particularly ethnicity, to facilitate more appropriate targeting of chemoprophylaxis. Multi-centre audit is a valuable clinical governance tool.
Introduction
Anti-tumour necrosis factor-α (anti-TNF-α) treatments provide dramatic symptomatic and prognostic benefit for some patients with autoimmune inflammatory conditions in the fields of rheumatology, dermatology and gastroenterology. However, concerns exist about their potential side effects including reactivation of latent tuberculosis (TB) which is particularly important considering the rising incidence rates of TB in the UK.1,2 The British Society for Rheumatology Biologics Register (BSRBR) was set up in 2001 to collate the details of patients with rheumatoid arthritis (RA) receiving anti-TNF-α agents and local units report significant events, including infections, in such patients to the register.3,4
Guidelines for TB screening were established involving the British Society for Rheumatology (BSR) and the British Thoracic Society (BTS) by a committee including respiratory physicians, a rheumatologist and gastroenterologist.5,6 These guidelines recommend that all patients should have a clinical examination, a chest radiograph within three months of starting anti-TNF-α treatment, their history of prior TB checked and, if appropriate, a tuberculin skin test performed. A skin test is recommended if the patient is not taking immunosuppressants (clarified as not having taken steroids in the last month or other immunosuppressants in the preceding three months7). An abnormal chest radiograph or past history of TB or TB treatment should prompt referral to a TB specialist. Patients with a normal chest radiograph, where a skin test is not appropriate, or those with a positive (appropriate) skin test should have a risk-benefit calculation, whereby their annual risk of TB on anti-TNF-α therapy is compared to the risk of hepatitis from TB chemoprophylaxis medication. This risk assessment calculation indicates that patients of certain ethnicities (black Africans or South Asians born abroad) or for others born abroad but who moved to the UK in the last four years should be considered for chemoprophylaxis.
The Department of Health and the Royal College of Physicians are seeking currently to strengthen local and multi-centre audit; audit may also be an important component of consultant recertification. Development of robust audit tools will be crucial to this process. Regional audits allow valuable comparison between units in guideline implementation as well as increasing the numbers of patients available for study.8–11 This is particularly relevant if each individual unit has a comparatively small number of patients receiving a treatment, such as anti-TNF-α.12 The West Midlands Rheumatology Services and Training Committee (WMRSTC) has organised regional audits approximately annually since 2000. These are coordinated by specialist registrars (SpRs) under consultant supervision and have become an established component of SpR training.
The aim of this study was to assess clinical practice in relation to TB risk assessment in rheumatology patients across the West Midlands commencing anti-TNF-α therapies in relation to the BTS guidelines.
Methods
A proforma was developed to include all suggested audit criteria described in the BTS guidelines (Fig 1) as well as a recommendation that all patients should be advised about the increased risk of TB with anti-TNF-α treatment.6 The proforma also surveyed the chemoprophylaxis and treatment regimes used.
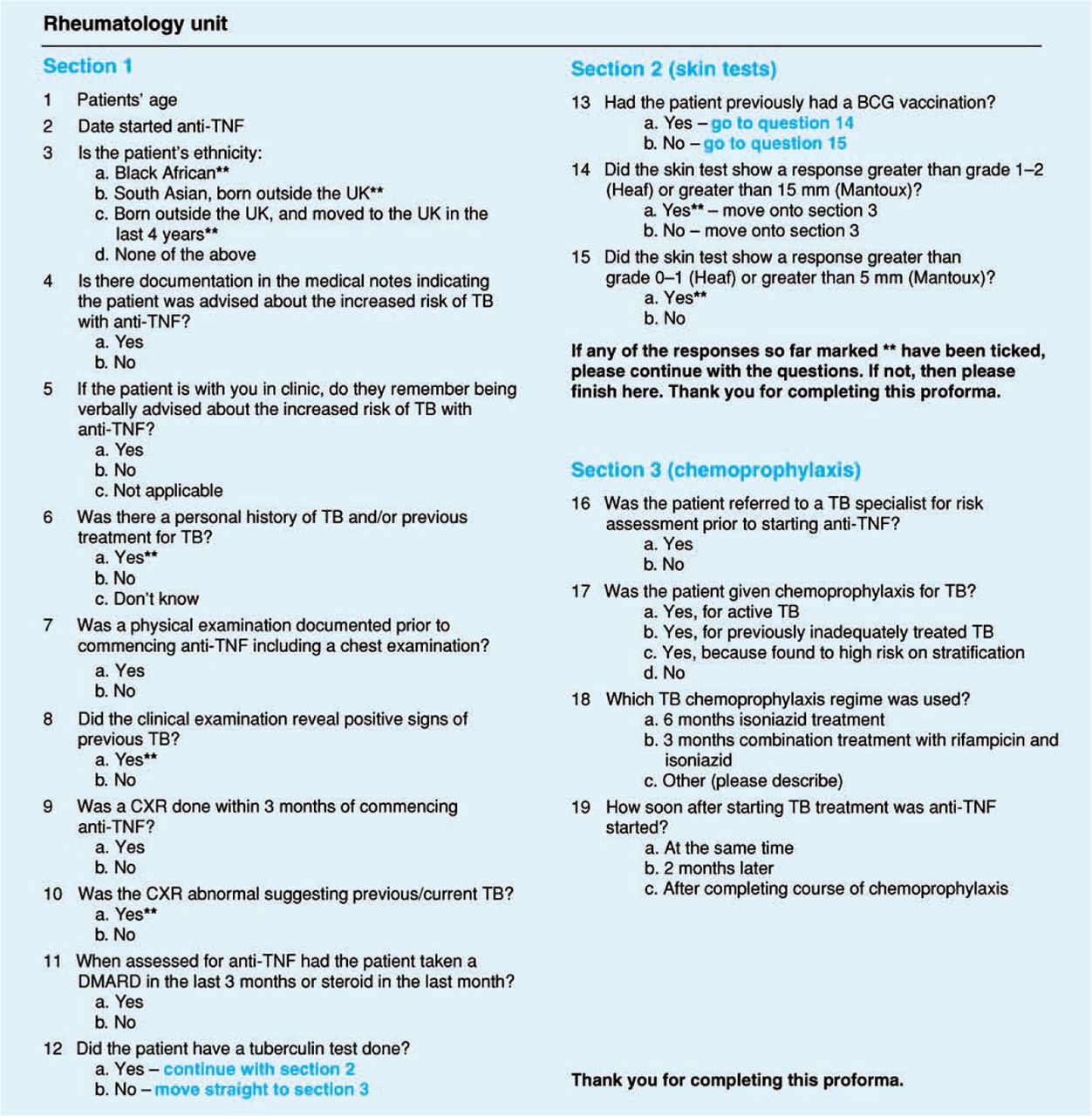
Proforma used for regional survey of tuberculosis (TB) risk assessment in patients taking anti-TNF-α treatment.
Thirteen rheumatology units in the West Midlands region retrospectively completed the proformas on patients receiving anti-TNF-α treatment attending the outpatient clinic over two months in 2006. Data from patients who were not due to attend in the two-month period were collected by review of their medical records and were supplemented in some instances by a telephone call. Descriptive statistics were performed on the data using Microsoft Excel.
Results
Data were collected from 856 patients (348 with the patient present and 508 by review of medical records). The mean duration of anti-TNF-α treatment was 1.7 years.
Adherence to recommendations prior to commencement of anti-TNF-α therapy
Of patients surveyed 47.5% (404/850) had a documented clinical respiratory examination; 84.5% (712/843) had a chest radiograph within three months of commencing anti-TNF-α therapy; 93% (795/856) were questioned about past history of TB or TB treatment. Although documented advice about the increased risk of TB occurred in only 45.8% (378/826) of cases, where data were collected with the patient present, 62.4% (217/348) recalled verbal advice.
Skin tuberculin testing
At the time of anti-TNF-α assessment, 94.3% (795/843) patients were taking immunosuppressants; a tuberculin test would therefore only have been appropriate in 5.6% (48 patients). Despite this, 27.0% (226/837) of patients had a tuberculin test performed. Of the 48 patients in whom testing would have been appropriate, it was performed on only 45.8% (22/48).
Identification of high-risk patients
Due to their ethnicity or birth place 3.3% (28/847) of patients were at high risk of TB. Clinical examination in 1.2% (5/404) of patients and 2.3% (16/708) of patients’ chest X-rays revealed positive signs suggesting previous or current TB. A personal history of TB or previous treatment for TB was documented in 2.4% (19/795) of patients. Of the tuberculin tests performed, 24.3% (55/226) of patients had a positive test result (adjusted for previous BCG vaccination). In total, 12.6% (108/856) of all patients surveyed had one or more high-risk factors, requiring risk stratification and chemoprophylaxis consideration prior to anti-TNF-α treatment.
Referral to a TB specialist
Of patients surveyed 3.4% (29/856) were referred to a TB specialist. Of those referred, 75.9% (22/29 patients) had one or more risk factors for TB, and 24.1% (7/29 patients) had no risk factors. However, 79.6% (86/108) of patients with one or more high-risk factors were not referred to a TB specialist.
Chemoprophylaxis/treatment
Tuberculosis chemoprophylaxis was given to 2.9% (25/856) of patients (23 patients were high risk when stratified and two had previously inadequately treated TB). Only one patient was treated for active TB. Of the 26 patients receiving chemoprophylaxis/treatment, the number of risk factors each individual patient had ranged from zero to three; the median number of risk factors was one. The patient treated for active TB had only one risk factor, namely an abnormal chest X-ray suggestive of TB. Of those receiving chemoprophylaxis/treatment, 14 patients had seen a TB specialist whereas 12 had not.
Only 4/28 patients who were high risk for TB due to their ethnicity or birthplace (where a risk-benefit calculation would suggest they are considered for chemoprophylaxis) were given chemoprophylaxis.
Comparison of patients pre-assessment for anti-TNF-α therapy pre- and post-publication of the British Thoracic Society guidelines.
Pre- and post-guideline publication
Table 1 compares performance before and after the publication of the BTS guidelines.
Variation in practice between units within the West Midlands region
Table 2 shows the marked variation in practice between the 13 units (anonymised) within the region in all aspects of this survey.
Comparison of clinical practice prior to commencing anti-TNF-α treatment between the units in the West Midlands.
Discussion
This survey revealed a broad failure to meet minimum standards in baseline respiratory system assessment and to record that patients were counselled about the increased risk of TB. However, a greater percentage of patients could recall this advice than was documented in their notes; this reflects a failure of documentation rather than deficient practice. Even so, one third of patients could not recollect such advice, therefore possibly not being alert to the early symptoms of TB. There was a wide range of inter-unit variability with regard to adherence to the BTS recommendations prior to anti-TNF-α commencement; units need to address individual practice and record-keeping to meet guideline standards.
Although there is a predominantly Caucasian population in this region, and hence the number of patients at risk of reactivation of latent TB is generally perceived to be low, this survey showed that 12.6% of the surveyed population had at least one risk factor for reactivation of latent TB.13 The majority of at-risk patients were not referred to TB specialists and chemoprophylaxis for high-risk patients was done independent of a TB specialist in just under half of cases. British Thoracic Society guidelines for chemotherapy for TB in the UK state that treatment should be supervised by TB physicians with access to TB nurse specialists.14 These findings have significant resource as well as clinical implications. Although decreasing inappropriate referrals would improve capacity, the increased use of anti-TNF-α agents, not only within rheumatology but also in the fields of dermatology and gastroenterology, could generate increased workload for TB specialists and relevant support specialties.
The BTS guidelines place particular emphasis on the increased TB risk associated with ethnicity and birthplace when considering chemoprophylaxis. It is noteworthy therefore that only 4/28 patients at high risk for these reasons were given prophylaxis, and suggests that perhaps greater awareness of these factors is required by clinicians.
The tuberculin skin testing results raise several issues. This was a retrospective study; many patients commenced anti-TNF-α prior to publication of the guidelines and the number of skin tests performed did decrease following guidance publication. The policy regarding skin testing varies throughout the region, with the majority of skin tests being done in two units, which may reflect local protocols, or possibly local ethnic variations. Although widely (but not uniformly) available and considered helpful when positive, there are caveats to skin test interpretation.15 False negative results may be due not only to immunosuppressive medication but also autoimmunity15; it is well recognised that due to deficient cell-mediated immunity there is an inadequate delayed type hypersensitivity reaction in RA patients.16 False positive skin test results may be due to previous vaccination with BCG (although childhood BCG may not explain a positive skin test in an adult), or interobserver variability as expertise is required in the actual reading of results.15,17,18 Novel T cell-based blood tests for TB should become generally available and their role should be considered in future algorithms. These measure T cell interferon-gamma release in response to antigens which are highly specific for Mycobacterium tuberculosis, so identifying patients with latent TB, and have been shown to be more specific and as sensitive or more so when compared to tuberculin skin tests.17 A survey of consultant rheumatologists in the UK revealed that 9% are already using such serological and immunological tests as part of their TB screening programme.12
As with previous regional audits, organised by the WMRSTC, this survey has allowed us to collect a greater amount of data than would be possible by auditing an individual unit and to allow comparison between departments.8–11 The results have been presented widely regionally; individual unit results being made available to the local team while anonymising results of other centres. Regional audits are perceived locally to be a valuable clinical governance tool and to provide trainees with useful opportunities to design, undertake, analyse and publish quality audit data. Other regions and specialties may consider such an audit model which, unlike national ones, has not required external funding. Production of quality audits facilitates review of guidelines, may be valuable in individual professional development and may improve clinical care.
Acknowledgements
We would like to thank the following for their help in the data collection: Drs Al-Allaf, H Ali, M Allen, R Amarasena, S Arthanari, N Barkham, S Baskar, J Bateman, S Bowman, R Butler, C Cardy, D Carruthers, V Chalam, K Chaudhuri, J Coppock, P Dawes, J Delamere, J Dixey, C Dowson, R Duncan, N Dunn, A Faizal, A Filer, K Grindulis, A Hassell, P Jobanputra, A Jordan, R Jubb, E Justice, S Kamath, S Khan, F Khattak, R Klocke, C Marguerie, A Menon, D Mulherin, P Newton, M Nisar, A Pace, J Packham, R Palmer, Z Paskins, A Paul, P Perkins, T Potter, A Prabu, T Price, A Price-Forbes, A Rai, E Rankin, J Ravindran, K Raza, D Rees, S Rigby, S Ryan, R Sandhu, S Saravana, M Shadforth, T Sheeran, A Sinha, D Situnayake, G Struthers, T Toms, A Whallett, R Williams, P Wong and K Yein; Ms K Blunn, Ms J Brewin, Ms A Brownfield, Ms S Butler, Ms F Chilton, Mrs S Collins, Ms M De La Cruz, Ms A Deeming, Mrs S Dunn, Ms K Edwards, Ms P Fraser, Mrs S Giles, Ms R Harper, Mrs D Homer, Ms K Jago, Mrs C James, Mrs S Kular, Ms D Lane, Ms J Lennon, Mrs D Lloyd, Ms S Logan, Ms J McDowell, Mrs J McPeake, Ms J Morrey, Mrs P Mountford, Mrs S Petford, Ms H Robinson, Ms S Roskell, Ms G Saldhana, Ms M Sheepy, Ms C Webb, Mrs E Wells, Mrs A Whitehead, Mrs A Wild; and Professors C Buckley, C Gordon, E Hay and G Kitas.
- © 2009 Royal College of Physicians








{kind=link}