
Lesson
A 49-year-old known alcoholic was admitted to hospital after being found collapsed with a witnessed minor haematemesis and melaena. The patient had multiple admissions to hospital with seizures that had been attributed to either alcohol intoxication or withdrawal. An emergency endoscopy revealed oesophageal ulcers. He suffered a seizure on admission and while recovering carpopedal spasm was noted and Chvostek's sign was positive. Initial blood investigations included potassium 2.9 mmol/l and calcium of 1.2 mmol/l treated with intravenous (iv) calcium gluconate. Blood tests revealed consistently low calcium levels (Fig 1) and a normal parathyroid hormone, compatible with primary hypoparathyroidism. He was noted to be anaemic and gave a history of diarrhoea. His serological tests for coeliac disease were positive and duodenal biopsy and histology confirmed inflammation and villous atrophy. He was advised to follow a gluten-free diet in addition to standard management for alcohol dependency. The patient re-presented to accident and emergency a few months later with a further seizure and died shortly after admission.
Discussion
Seizures are a frequent reason for admission to emergency departments and can occur on withdrawal as well as during acute intoxication. Hypocalcaemia causes neural hyperexitability leading in the periphery to muscle spasms (Chvostek's sign and Trousseau sign) up to tetany. Changes to the central nervous system include irritability, confusion and in severe cases seizures which require rapid iv calcium gluconate to minimise
risk of laryngeal spasm and cardiac arrhythmias. The effects of alcohol ingestion on electrolyte balance are only partly understood but several mechanisms of hypocalcaemia have been implied (Table 1).1–3
Coeliac disease is a common condition (prevalence 1:300) with sensitivity to dietary gluten resulting in immune-mediated destruction of small bowel villi, villous atrophy, reduced surface area and malabsorption of calcium and vitamin D.4 Although detection of tissue transglutimase IgA is a highly sensitive and specific test, the gold standard for diagnosis currently remains duodenal biopsy. Treatment consists of complete avoidance of gluten with restoration of normal mucosa with reversal of malabsorption. Coeliac disease is associated with other autoimmune diseases including idiopathic hypoparathyroidism, which can contribute to hypocalcaemia.
In this case reduced dietary calcium and vitamin intake as well as alcohol-induced metabolic changes might have played a role in the patient's chronic hypocalcaemia, however, it is believed that the main cause of the fits was his addiction to alcoholic beverages containing gluten, maintaining mucosal inflammation and villous atrophy.

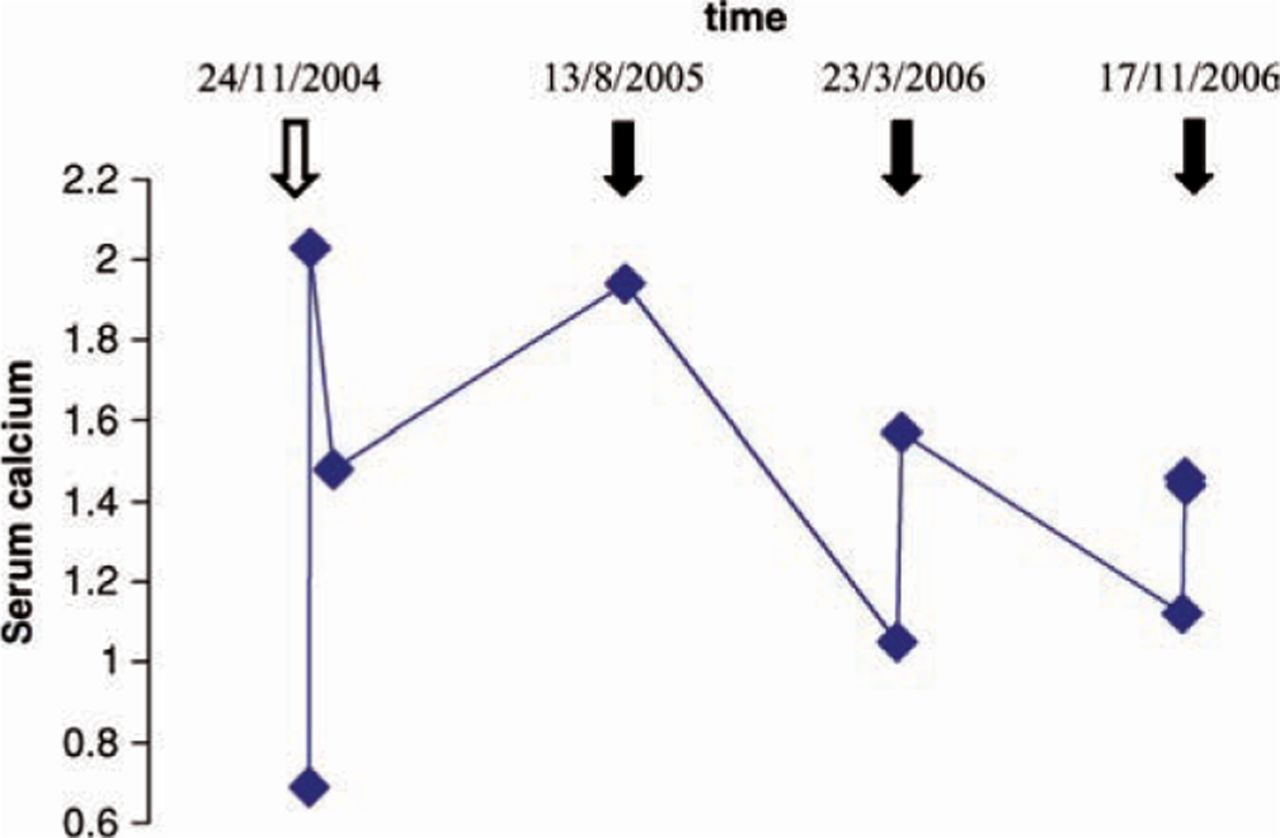
The patient's serum calcium (corrected for albumin). The open arrow indicates a hospital admission for confusion, the closed arrows indicate admissions with presumed ‘alcoholic fits’.
Possible mechanisms for hypocalcaemia in alcoholics.
In summary:
metabolic causes of fits, such as hypocalcaemia, have to be considered and treated even when more common causes are apparent triggers
alcohol influences calcium metabolism leading to hypocalcaemia
coeliac disease is a frequent and well-established cause of hypocalcaemia
in alcoholics with coeliac disease, poor compliance, consumption of beer and other gluten containing beverages as well as generally poor nutrition may all contribute to hypocalcaemia.
- © 2009 Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.