
Abstract
Patients with HIV are dying due to late diagnosis and physicians are being encouraged to increase HIV testing. The uptake of opt-in HIV screening for 113 lymphoma patients was audited at University College London Hospital. Of the 113 patients, 46 were not tested (41%). Previous research in the antenatal setting suggests that adopting opt-out screening would increase testing rates.
Introduction
Patients with HIV are dying unnecessarily due to late diagnosis.1In September 2007, a letter from the Chief Medical Officer encouraged clinicians in primary and secondary care to increase levels of HIV testing.2The incidence of Hodgkin's and non-Hodgkin's lymphoma (NHL) in HIV-infected persons greatly exceeds that of the general population, and physicians who treat lymphoma may be able to improve outcomes by increasing routine HIV testing.3
Awareness of HIV status is important at the time of lymphoma diagnosis for a number of reasons. HIV-infected patients are frequently co-infected by hepatitis viruses. This has important implications especially the risk of fulminant hepatitis B when rituximab is used. There are also higher risks of treatment-related complications due to drug interactions, compounded side effects, and the potential effects of chemotherapy on the CD4 cell count and HIV viral load. Awareness of HIV status may affect the choice of anti-lymphoma therapy.4Patients suffering from HIV-related lymphoma have worse outcomes compared to the non-infected patients, although the use of concurrent antiretroviral treatment improves prognosis.5The use of growth factors and prophylaxis against opportunistic infection is also recommended in published guidelines.6For all of these reasons, current European guidelines recommend HIV testing in all patients with cerebral lymphoma and aggressive NHL.7Current practice at University College London Hospital was audited with respect to HIV testing in patients treated for lymphoma.
Methods
An electronic prescribing system was used to identify all patients with lymphoma in whom a new course of chemotherapy was initiated between 1 October 2006 and 30 March 2007. Diagnoses were grouped into Hodgkin's lymphoma (HL), aggressive NHL, indolent NHL, or primary central nervous system (CNS) lymphoma.
Results
Chemotherapy for lymphoma was initiated on 113 patients during the audit period, 67 male and 46 female, with median age 53 (range 11–85). In total, 27 patients had HL, 46 had aggressive NHL, 39 had indolent NHL, and one patient had primary CNS lymphoma. Of the 113 patients, 38 received a bone-marrow transplant (seven for HL, 14 for NHL and 17 for indolent NHL). All but 14 were still alive on 1 September 2007 (one HL patient, seven NHL patients, one CNS lymphoma patient and five indolent NHL patients including three post-transplant).
Nine patients were HIV positive (8%), 58 were HIV negative (51%), and 46 were not tested (41%). Seven of the nine patients were known to be HIV positive prior to diagnosis of lymphoma, but two men were previously undiagnosed (one a 57-year-old African-born heterosexual and one a 47-year-old European-born heterosexual). Of the nine patients who were HIV positive, three were also hepatitis B positive (one of the three had been previously undiagnosed) and none were hepatitis C positive. Six of these nine patients had aggressive NHL including one Burkitt, one primary effusion lymphoma, and one plasmablastic lymphoma, and three had classical HL. One HIV-positive patient was transplanted (for HL). Seven were still alive on 1 September 2007.
HIV was more prevalent among patients with aggressive NHL or HL than patients with indolent NHL, but testing rates were similar (Table 1). HIV testing was more prevalent among the 38 patients who received autologous or allogeneic bone marrow transplants (95% tested: χ2 = 30.5; df = 1; p<0.001). There was a trend to higher testing rates for male patients (65% v 50%: χ2 = 2.4; df = 1; p = 0.1). Testing rates also varied by age: younger and older patients were less likely to be tested (Fig 1).
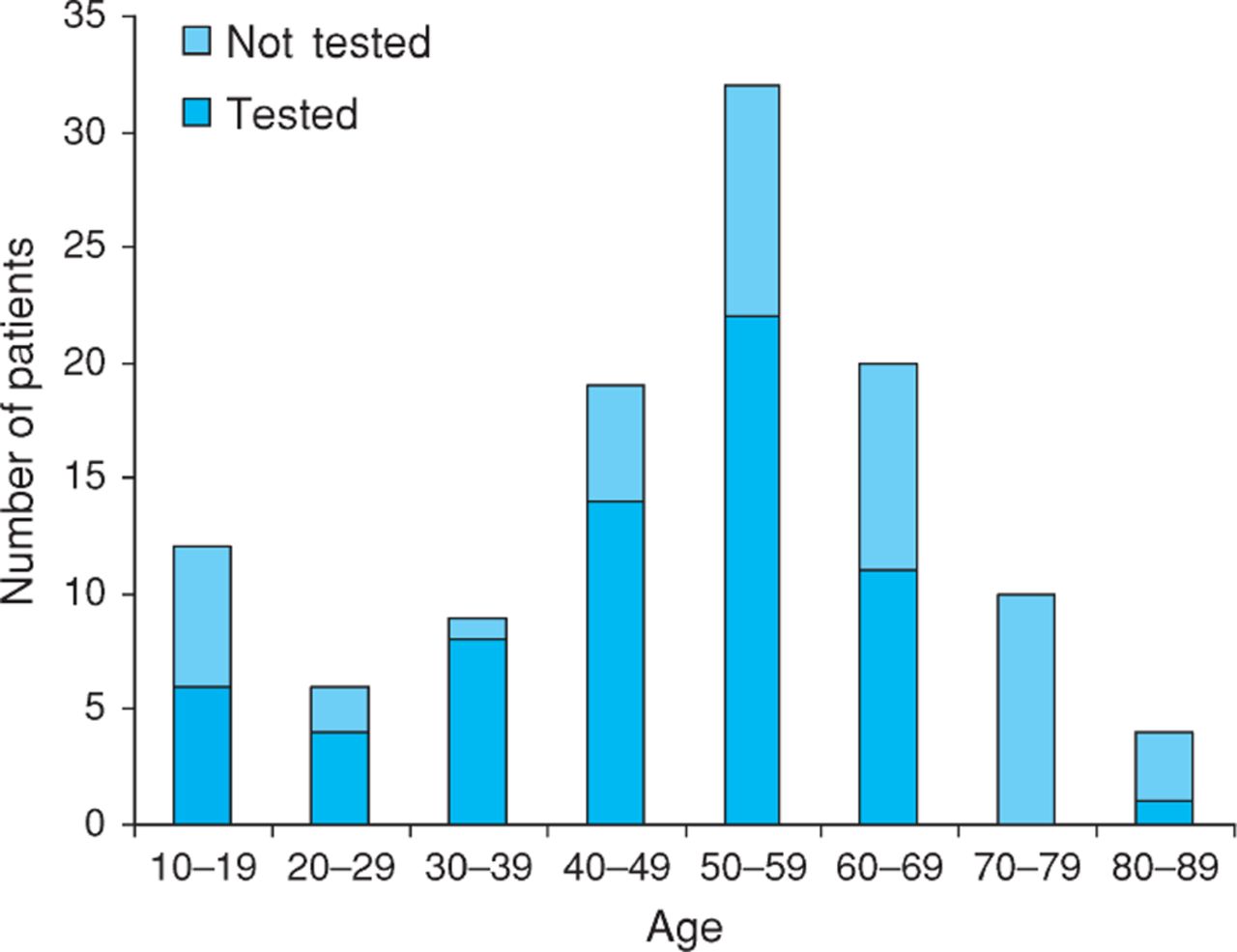
HIV testing by age.
HIV testing by diagnosis.
Retrospective case note review of the patients who did not undergo HIV testing showed that HIV was not raised as an issue by clinicians.
Discussion
In our cohort of lymphoma patients, we found a high prevalence of HIV co-infection (8%), supporting the implementation of screening for HIV infection in lymphoma. HIV screening is in fact recommended as part of the routine work up for lymphoma patients in the unit, but a relatively high proportion (41%) were not tested.
Testing lymphoma patients for HIV carries some similarities to HIV testing in pregnancy: the majority of patients are HIV negative and low risk, but a small group are positive and will benefit from this information being known. Three ways of organising HIV testing have been investigated in the antenatal setting: risk assessment, opt-in or opt-out. Risk assessment involves clinicians identifying individuals felt to be ‘at risk’ and offering them tests. Opt-in testing involves clinicians offering patients a test, and the patient choosing whether to give consent. Uptake levels are around 35% with opt-in testing during pregnancy, and are unaffected by the level of counselling and patient information given.8Opt-out testing involves informing patients that HIV testing is routine, for example by giving them a leaflet, but with no obligation on the physician to obtain individual consent. The patients of course have the right to opt-out. Opt-out testing has resulted in 81–88% uptake in pregnancy in the published literature, and approaches 100% at our trust (SG Edwards, personal communication).9
The policy adopted for lymphoma testing in our unit during the audit period was an opt-in policy. Our uptake level of 59% was relatively high compared to opt-in testing in the antenatal setting. The data collected suggest there was an element of risk assessment involved in the testing strategy at the unit, with men tested more frequently than women, and testing rates varying by age. The Centers for Disease Control and Prevention (CDC) has argued against risk assessment in their recommendations on HIV testing, however, because the changing demographics have rendered risk assessment ineffective: HIV is now increasingly prevalent among those aged under 20 and among heterosexual men and women.10
Screening for HIV at the unit was adequate during the audit period as there were no mid- or post-chemotherapy diagnoses. However, because the epidemiology of HIV is evolving and because physicians are being encouraged to increase HIV testing in order to reduce late diagnoses, it is essential to increase the testing rate to close to 100%. HIV testing in all newly diagnosed lymphoma patients is recommended and previous research in the antenatal setting suggests an opt-out approach would be the most successful way of achieving this policy.
Acknowledgements
Thanks to Professors A Goldstone and D Linch for their support.
- © 2009 Royal College of Physicians








{kind=link}