
Abstract
This study evaluates the patient and disease characteristics, potential cost implications and short-term outcomes of 64 adult patients admitted with HIV-related illnesses. The majority (65.6%) were black Africans and 75% were immigrants to the UK. Of the 64 patients, 61% were unaware of their HIV status at admission; 50% had CD4 count <50 cells/μl and 48% had viral load >105 copies/ml. Thirty-eight patients had AIDS and this accounted for 66% of the total 897 inpatient days (equivalent to 16.5–30.2 patient years of highly active antiretroviral therapy (HAART) depending on the type of HAART regimen used). Fifteen (23.8%) died in hospital, and of these 11 had AIDS and a CD4 count <200 cells/μl. Immigrants from countries of high prevalence accounted for the majority of the inpatient HIV caseload. They presented late and had high in-hospital mortality. Screening programmes to allow early diagnosis and treatment should be adapted to reach migrant populations.
Introduction
It has been estimated that nearly 58,300 people were affected by HIV infection in the UK at the end of 2004 and that one-third of them would have been unaware of their infection.1In the UK, specialist care for these patients is mostly provided by dedicated HIV units based at university teaching hospitals. HIV-related morbidity and mortality have substantially decreased since the introduction of highly active antiretroviral therapy (HAART).2–4 However the administration of HAART requires medical personnel who are knowledgeable and familiar with its usage. In the 1980s and early 1990s, only homosexual men and intravenous (iv) drug users were considered to be at high risk of acquiring HIV infection. Recent reports suggest that it has become increasingly common among heterosexual men, accounting for 59% of the newly acquired infection in the UK between 2001 and 2005.1Patients who were traditionally not considered to be at high risk and not yet aware of their infection may access healthcare services in district general hospitals (DGHs) where staff may not be adequately trained to recognise or manage HIV-related illnesses. This could lead to a delay in diagnosis and possibly inadequate treatment. This study analyses the patient characteristics, clinical presentation, potential cost implications and short-term mortality of patients admitted with HIV-related illnesses and represents, to the best of the authors’ knowledge, the only report of outcome data in this group of patients in the UK admitted to a DGH without a specialised HIV/AIDS unit.
Methods
This was a retrospective study of all patients aged over 18 years admitted through the emergency medical services to the Royal Berkshire Hospital between 1 January 1999 and 31 December 2004 with either a pre-existing diagnosis of HIV infection or with a newly diagnosed HIV infection. Only the first admission per patient during the study period was included in the analyses. Patients with HIV infection who had planned admission to hospital were not included in the study. Any patients admitted under surgical teams were excluded. The study hospital provides acute emergency services to a population of 450,000 and patients who were admitted with HIV-related illnesses were all managed by general physicians working in close collaboration with the genitourinary medicine (GUM) department. The GUM department provides outpatient care for all patients diagnosed with HIV infection. The inpatient medical records were reviewed for demographic details, clinical presentation, viral load and CD4 count at the time of hospital admission. Details of previous HAART for patients diagnosed with HIV infection prior to the current admission to hospital were obtained from outpatient records. All patients were followed until discharge from hospital or death in hospital during the current admission.
Results
In total, 64 patients were admitted with an HIV-related illness during the study period. Subsequent admissions for the same patient during the study period were not included in the analyses. The mean age was 37 years (range 22–67 years) and 55% of them were males. Of the 64 patients, 63 were infected with HIV type 1 while the other patient had HIV type 2 infection. The majority (n = 39) were unaware of their HIV status prior to hospitalisation while the remaining 25 were known to have had HIV infection prior to the current admission.
Ethnicity and country of origin
Black Africans (BA) accounted for the majority (65.6%) of patients followed by White (32.8%) and Black Caribbean (BC) (1.6 %) patients. There were no Asian or Chinese patients in our study (Fig 1). The proportion of BA was higher (71%) among those who were unaware of their HIV status prior to the current admission compared to 52% among those who were known to be infected with HIV prior to the current admission (Chi-squared p = 0.01). About 75% of all patients were immigrants to the UK, predominantly coming from Southern and East African countries (Zimbabwe (n = 13), Zambia (n = 5), Kenya (n = 5), South Africa (n = 4), and one patient each from Uganda, Tanzania and Nigeria). The remaining immigrants originated from Portugal, Ghana, Burundi, Mexico, Nigeria, Rwanda, Senegal, Cameron and Sierra Leone. Only 38% of all patients had permanent resident settlement status in the UK, while the rest had temporary immigration permits: student visas (28%), asylum seekers (11%), visitor visas (8%), work permits (6%). We could not ascertain the immigration status in 9% of the patients.
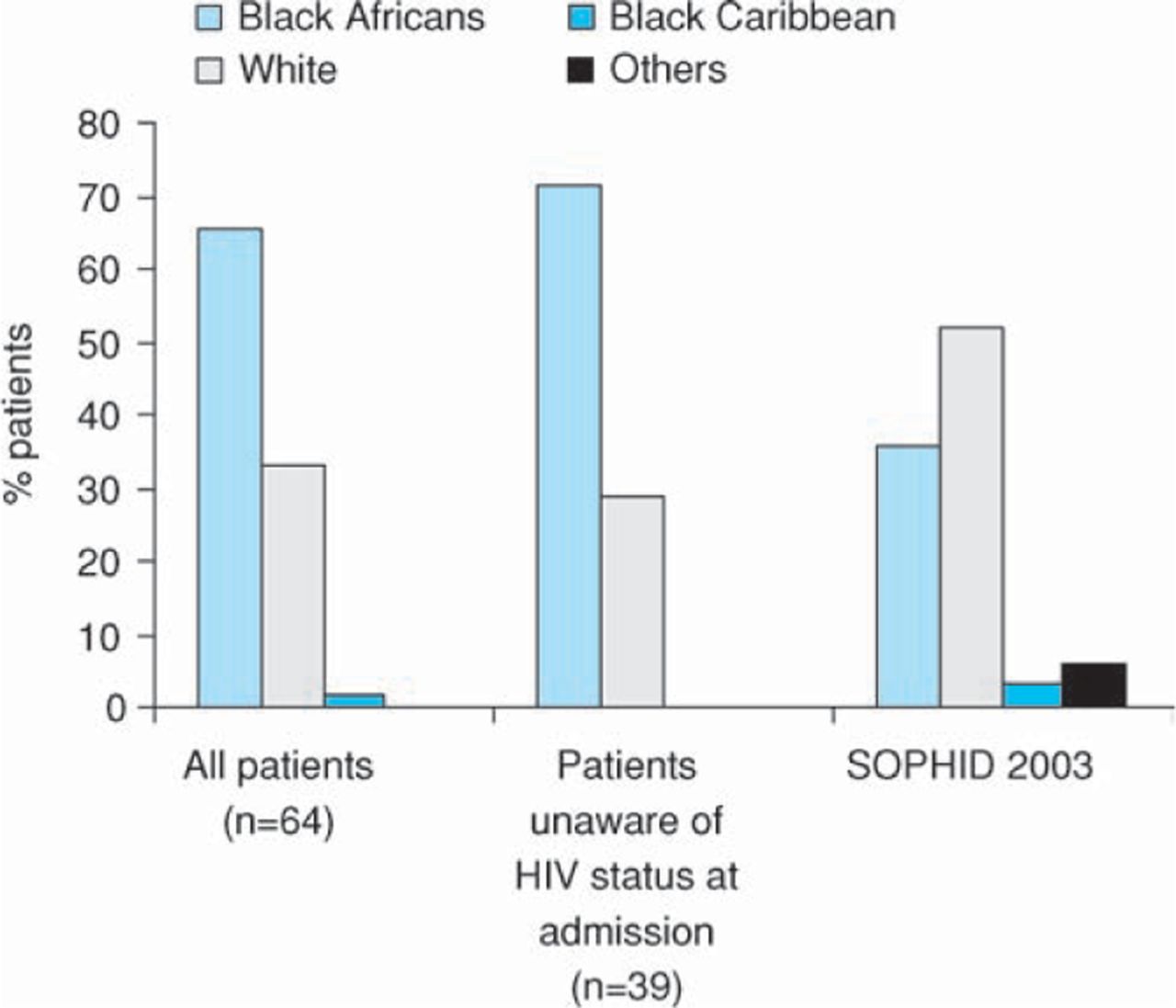
Ethnicity of study participants compared to data from a national survey (SOPHID (Survey of Prevalent HIV Diagnosed in England, Wales and Northern Ireland) 2003).7 Others included patients classed as Asian, Chinese, Black and other.
Routes of acquiring infection
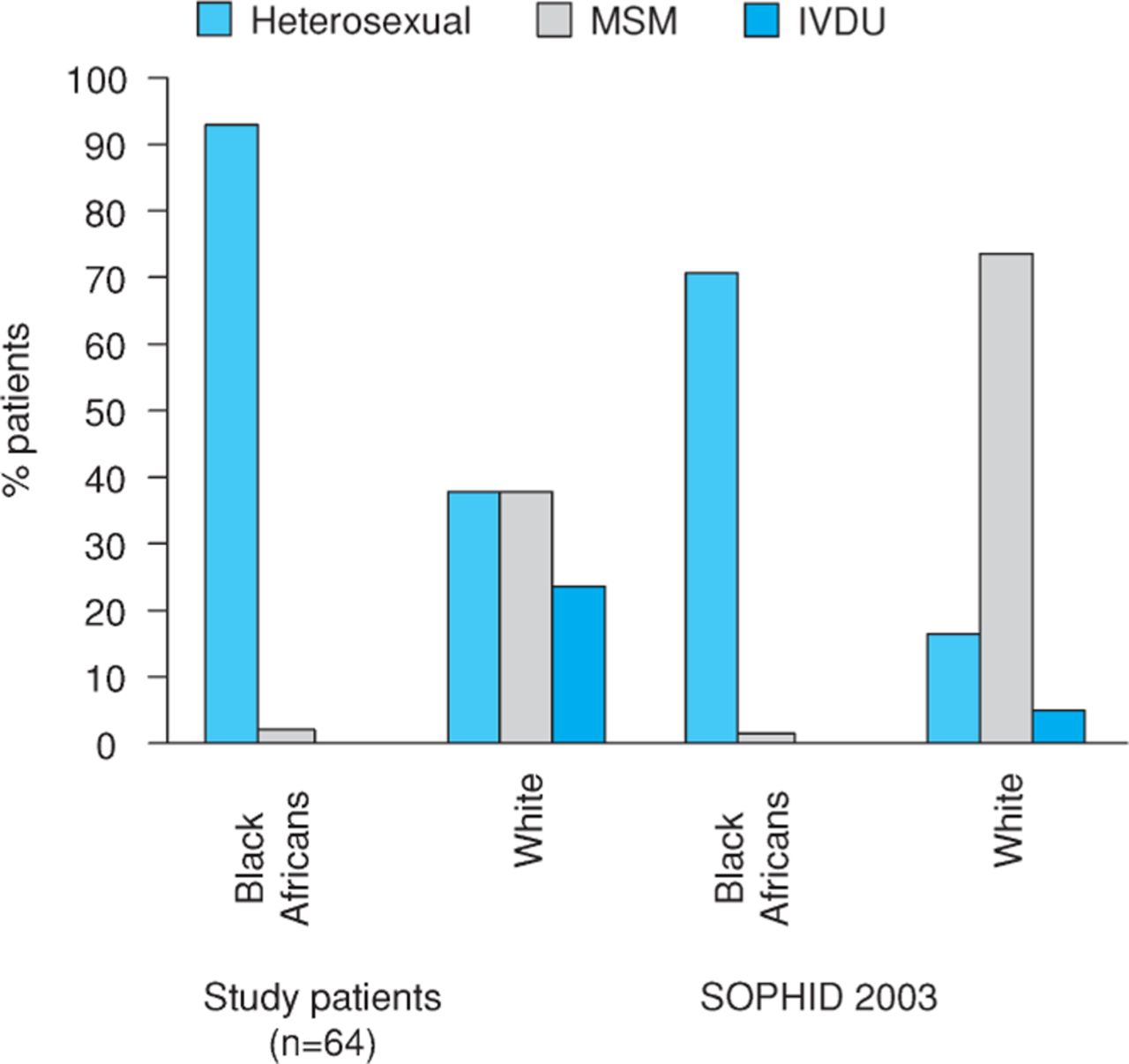
About 75% of our patients acquired the HIV infection heterosexually, while the rest acquired the infection through sex between men and men (14.1%), iv drug use (7.8%) and through an unknown route (3.1%). Heterosexual route of infection was more common among BA compared to white patients (92.8% v 38.1%, Chi-squared p<0.0001) (Fig 2) and an equal proportion of white patients acquired the HIV infection through the heterosexual route and through sex between men and men.
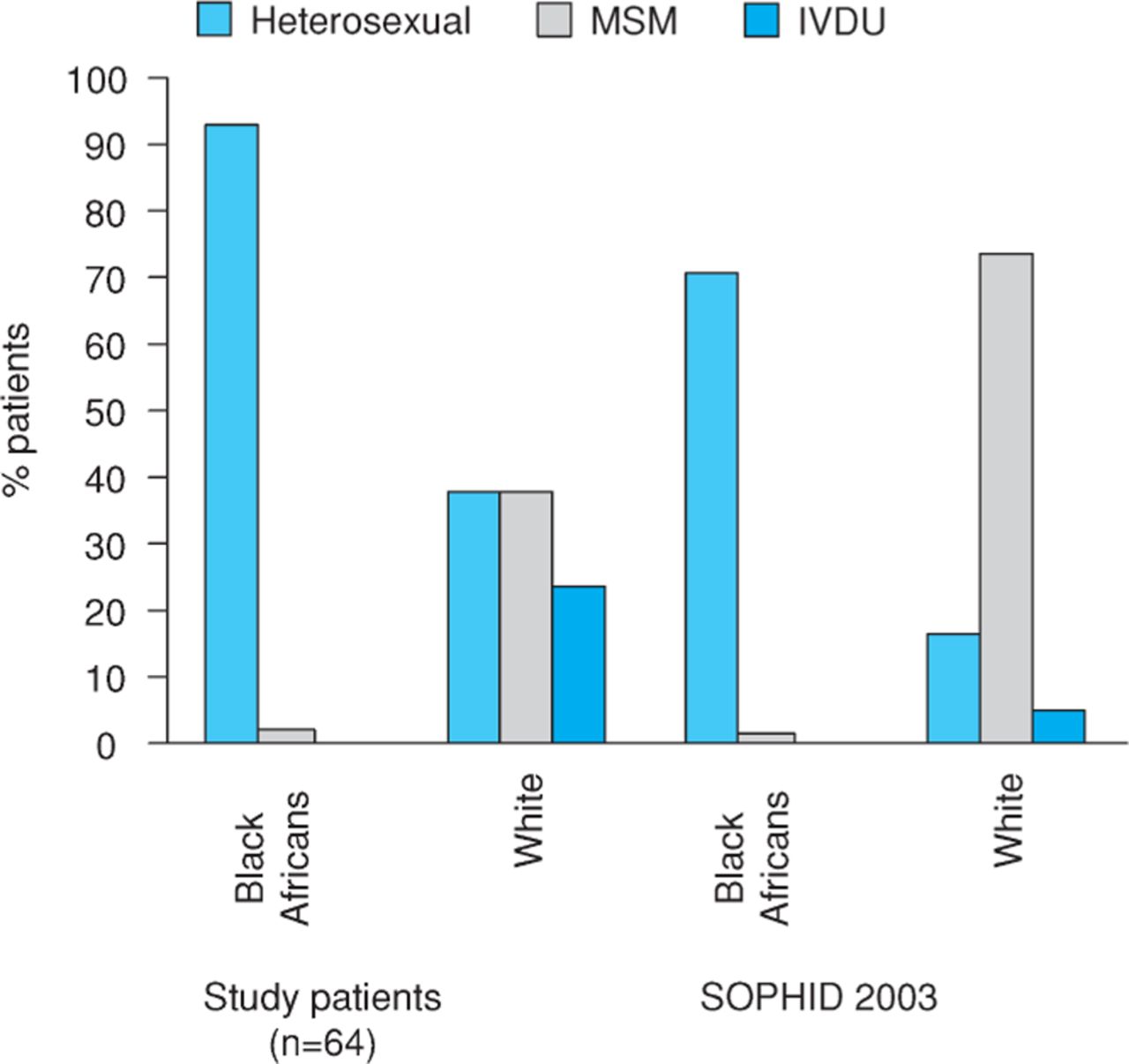
Routes of acquiring HIV infection in study participants compared to data from a national survey (SOPHID (Survey of Prevalent HIV Diagnosed in England, Wales and Northern Ireland) 2003).7 IVDU = intravenous drug use; MSM = sex between men and men.
Clinical manifestations
A diagnosis of an AIDS-defining illness was made in 38 patients and this was interestingly more common among those who were known to be infected with HIV prior to the current episode of hospitalisation compared to those who were unaware of their HIV status at the time of admission (68% v 54%, Chi-squared p = 0.001) (Table 1). Mycobacterium tuberculosis (TB) (21.8%) was the most common AIDS-defining illness followed by pneumocystis jeroveci pneumonia (PCP) (20.3%). Pulmonary disease was the most common form for TB (50%). Extra pulmonary sites of TB involvement included liver, lymph nodes and central nervous system. There were two cases of atypical mycobacterial (MAI) infection. Bacterial pneumonia was the single most common non-AIDS-defining illness seen in seven patients.
Clinical manifestations in patients diagnosed with HIV prior to hospitalisation compared to those who were unaware of HIV status at admission.
CD4 counts and viral load at admission
CD4 count was less than 350 cells/μl in 56 patients, of whom 32 had counts of less than 50 cells/µl and a further 16 had counts between 50 and 200 cells/µl. The CD4 count was not available in one patient. There was no difference in CD4 counts between those who were known to have had HIV infection and those who were unaware of their HIV status at admission (52% v48%, Chi-squared p = 0.8). The viral load was not available in two patients. Viral load was more than 105 copies/ml in 31 of the remaining 62 patients. The proportion of patients with high viral loads of >105 copies/ml was significantly more among those who were unaware of their HIV status at admission compared to those who were known to be HIV positive prior to admission (59% and 32% respectively, Chi squared p = 0.01).
HIV diagnosis and duration of HAART in relation to hospital admission
HIV seropositivity was established within a week of admission in 36 of the 39 patients who were unaware of their HIV status at admission. Of these 36 patients, 32 were diagnosed within the first three days. Of the 25 patients who were known to have had HIV infection prior to admission, only eight had a diagnosis established more than a year previously. Of the remaining 17 patients, 15 (12 black, three whites) were diagnosed with HIV less than three months before admission and two were diagnosed three to 12 months prior to admission. Only 12 of these 25 patients were prescribed HAART prior to hospitalisation. Five out of the 12 patients who had been prescribed HAART prior to admission were noncompliant with treatment.
Duration of hospital stay and potential cost implications
The total number of inpatient days for all patients was 897 (mean of 14 days per patient; range 1–85 days). The total inpatient stay for patients with known HIV infection prior to hospitalisation was 272 days (mean of 10.8 days per patient) and was 625 days (mean of 16 days per patient) for those diagnosed with HIV infection after hospitalisation. Majority of the inpatient stay (596 days) was related to admissions with an AIDS-defining illness. The median cost of HAART per patient year in the UK has been estimated to vary between $12,000 to $22,000 (£6,000 to £11,000) according to the HAART regimens prescribed (regimens containing protease inhibitors being more expensive).5A report published in the UK in 2004 estimated the average inpatient cost per day to be $610 (£308).6The total inpatient costs incurred by all patients in our study for a total inpatient stay of 897 days would be $547,170 (£275,000). This would be equivalent of 24.8–45.5 patient years of HAART depending on the HAART regimen used. The total cost incurred by 596 inpatient days due to an AIDS-defining illness would be $363,560 (£183,610) which is equivalent to 16.5–30.2 patient years of HAART depending on the HAART regimens used.
Inpatient mortality
Fifteen patients (23.4%) died while in hospital during the admission period. Deaths were due to disseminated Kaposi's sarcoma (n = 3), non-Hodgkin's lymphoma (n = 2), extra pulmonary TB (n = 2), PCP (n = 2), bacterial pneumonia (n = 3), HIV-associated nephropathy (n = 2) and cervical cancer (n = 1). Eleven out of these 15 patients were diagnosed with HIV either shortly before (<3 months) or after admission and had CD4 counts less than 200 cells/μl.
Discussion
The majority of patients admitted with HIV-related illnesses in this study were unaware of their HIV status at admission, were of BA origin and were immigrants to the UK from countries with a high prevalence of HIV. CD4 counts were less than 50 cells/μl at admission in 50% and an AIDS-defining illness was diagnosed in about 60%. Total estimated costs relating to these admissions were equivalent to 24.5–45.5 HAART patient years depending on the type of HAART regimen used. Admissions relating to AIDS accounted for two-thirds of these costs. Short-term mortality was high with nearly 24% of patients dying during the current admission.
There was an overrepresentation of ethnic minority in our study compared to SOPHID 2003 (Survey of Prevalent HIV Infections Diagnosed) in England, Wales and Northern Ireland and this could be due to a large proportion of ethnic minority patients in the catchment area (Berkshire) of the hospital −11.3% compared to 7.9 % in the UK.7,8 Equally it is possible that BA present late with severe illnesses leading to increased hospital admission. In our study there were more BA diagnosed with HIV after hospitalisation (Fig 1) and they represented the majority of patients with a CD4 count <200 cells/µl. Late presentation with CD4 count below 200 cells/µl was similarly more common in BA than whites in a recent study of newly diagnosed HIV infection in the UK and Republic of Ireland.9In 2004, there were 778 individuals diagnosed with AIDS in England, Wales and Northern Ireland of whom 69% were black or from ethnic minority groups.1
Of the patients in this study, 75 acquired infection heterosexually compared to 59% from reports in the UK conducted in the same period.1,7 The majority of our patients were BA in whom the heterosexual mode has been reported to be the predominant route (87.2%) of acquiring HIV infection in the UK.1However the majority of whites in our study had also acquired HIV infection heterosexually in contrast to that reported in SOPHID 2003 (Fig 2). Patients who acquire the infection heterosexually have been reported to present late with CD4 counts of <200 cells/µl.9The majority (75%) of our patients were late presenters with CD4 count <200 cells/µl and it is likely that late presentation was also associated with the heterosexual mode of transmissions in whites.
Of patients known to have HIV infection at admission, 52% presented with CD4 counts <200 cells/µl. Only four out of the 25 patients diagnosed before admission were receiving HAART for more than three months and were compliant with their treatment. The remaining either had inadequate treatment or insufficient time for immune reconstitution to occur with antiretroviral therapy. This might explain why a significant proportion of the patients presented with an AIDS-defining illness despite being diagnosed with HIV infection prior to admission. Of the patients in whom the HIV status was unknown prior to admission, 54% presented with an AIDS-defining illness. Another 13% were admitted due to other HIV-related illnesses (HIV-associated nephropathy, seroconversion). Serological testing for HIV was considered in 82% of these patients within the first three days of admission. This would imply a low threshold for HIV testing in ill patients especially from ‘high risk’ countries such as Zimbabwe admitted to the DGH and reflects an increased awareness among medical staff of the global HIV pandemic and the impact of the African HIV epidemic on admission to some UK hospitals of patients from African countries.
The in-hospital mortality was nearly 24% compared to 12% reported by Sherer and colleagues.10A Canadian study demonstrated an inverse relationship between the hospital HIV caseload and in-hospital mortality suggesting that high volume hospitals are better equipped to recognise and effectively deal with seriously ill HIV-infected patients.11The study hospital does not have a dedicated HIV/infectious diseases unit and patients with HIV-related illnesses have previously been managed in a medical ward by general physicians working in close conjunction with the GUM department. The high mortality in this study could also be due to a high proportion (74%) of deaths among late presenters (CD4 count <200 cells/µl) with AIDS. It has been previously reported that between one quarter and one third of HIV-related deaths occur in patients in whom the diagnosis of HIV infection and AIDS are made simultaneously or within three months of each other.12All of the 39 patients who were unaware of their HIV status at admission in our study either presented directly to emergency medical services, not having been assessed by their general practitioner (GP) or could not recollect being offered a HIV test by their GP prior to admission. An HIV risk assessment using an ‘opt-out’ policy, carried out in all patients particularly from the African subcontinent presenting with symptoms that could be explained by undiagnosed HIV infection might allow early diagnosis and treatment of the disease.
The total annual costs of providing care for HIV-infected patients is directly related to the severity of disease.13The increased expenditure on HAART might be offset to some extent by improved survival and cost savings associated with decreased hospital admission.14Early diagnosis in our patients prior to admission and improved compliance with treatment could have prevented AIDS-related hospital admissions with a cost saving for the NHS of up to 45 patient years of HAART. The Department of Health has agreed free NHS treatment for people with temporary immigration documents, if they are legally resident in this country for more than a year.15Only 38% of the patients in this study had permanent resident status in the UK. It would be unethical to deny hospital admission or treatment to those individuals who are acutely unwell based on their immigration status and the British HIV Association supports the notion of clinicians treating patients on clinical grounds, and not acting as gatekeepers of eligibility to NHS care.
In conclusion, immigrants from countries of high prevalence account for a significant proportion of the HIV inpatient caseload. The majority of them present late with low CD4 counts and AIDS-defining illnesses which result in high mortality and which have significant cost implications to the NHS. Screening programmes to allow early diagnosis, treatment and care should be adapted to reach this migrant population.
Note
The conversion rates used in the ‘Duration of hospital stay and potential cost implications’ section were correct in October 2005.
- © 2009 Royal College of Physicians








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.