
Abstract
The objective of this study was to assess the increasing number of patients with positive biopsies yet negative serology at Medway Hospital, Kent, through a retrospective data collection. All coeliac serology undertaken between 2003–5 (n = 3,056) with coeliac positive duodenal biopsy results (n = 26) were compared. From the total number of patients with positive duodenal biopsies 10 (38.5%), 13 (50%) and 12 (46.2%) had negative anti-tTg, IgA anti-gliadin and IgG anti-gliadin serology respectively. When combining anti-tTG, IgG and IgA anti-gliadin to improve sensitivity, five patients (19.2%) had completely negative and six (23%) had equivocal serology results. This study shows that a small but significant number of cases of coeliac disease will be missed by relying on serology alone. As the diagnosis and management of disease shifts further towards general physicians and primary care, it is important that the limitations of serological testing are recognised.
- coeliac disease
- coeliac serology
- gluten
- IgA anti-endomysial antibodies
- IgA anti-gliadin antibodies
- IgA ani-tissue transglutaminase antibodies
Background
Coeliac disease is an inflammatory disorder of the small bowel which is a result of protein-rich amines (prolamines) that are found in wheat, barley and rye interacting with the bowel mucosa. This ‘gluten-sensitive enteropathy’ results in atrophy of the villi causing malabsorption with symptoms of diarrhoea, steatorrhoea, weight loss and anaemia. Abdominal pain, distension and other vague, non-specific symptoms such as fatigue are also common. Long-term health consequences associated with untreated coeliac disease include osteoporosis and an increased incidence of malignancy. Associated conditions include autoimmune thyroid disease, diabetes and dermatitis herpetiformis.1The prevalence of coeliac disease has been estimated to be as high as 1:100 in the UK and Ireland.1
Patients can present at any age. ‘Adult’ coeliac disease often presents with iron deficiency anaemia and non-specific symptoms mimicking irritable bowel syndrome (IBS). The gold standard method for diagnosing coeliac disease is by identifying characteristic histopathological changes from an adequate small bowel biopsy based on the modified Marsh criteria.2In 1989, serological testing was included in the criteria for the diagnosis of coeliac disease.3Serology has progressed from the use of anti-reticulin antibodies to testing for IgA anti-gliadin antibodies, IgA anti-endomysial antibodies and more recently to ELISA for IgA anti-tissue transglutaminase antibodies.4Published data on the serological testing of coeliac disease indicate both high sensitivity and specificity of these antibodies with the sensitivity and specificity of IgA anti-tissue transglutaminase antibodies being much higher (99% and >90%) than IgA anti-gliadin (46–100% and 86–100%) and IgA anti-endomysium (74–100% and 91–100%)5. Duodenal biopsy is still recommended as it helps stage the severity of the disease and differentiates latent disease, but there is now increasing reliance on non-invasive testing.
Pitfalls in serological testing include false negative results in the 3% of coeliac patients who are IgA deficient. In such cases, those with negative serology yet strong clinical suspicion should have their IgA status assessed and undergo IgG-based serological testing.6,7
Most hospitals around the UK rely on serology and often combine tests to improve the sensitivity and specificity to near 100%. At the Medway Hospital, Kent, however, a number of patients with positive biopsies but negative serology were recorded and so a retrospective analysis of serological and histological testing for this condition was performed.
Methods and aims
The results of all coeliac serology performed between 2003 and 2005 (3,056 patients) were collected and correlated with the results of duodenal biopsies (42 patients) which fulfilled the histological criteria for coeliac disease.
At Medway Hospital three ELISA tests were performed as standard during the three years studied:
IgA anti-gliadin antibodies
IgG anti-gliadin antibodies
IgA anti-tissue transglutaminase (tTG) antibodies.
Any positive anti-tTG antibodies were confirmed with immuno-fluorescent staining of monkey oesophagus for IgA anti-endomysial antibody. The ELISA tests were recorded in U/ml and the anti-endomysial tests recorded as an end-point titre. The reference ranges for results were < 10 U negative, 10–15 U equivocal and > 15 U positive.
Results
Of the 3,056 patients, 42 had positive biopsies and 16 of these were diagnosed on biopsy without serology. Of the 26 remaining patients, 10 (38.5%, 95% confidence interval (CI) 20.3 to 57.8%) had negative tissue transglutaminase (anti-tTG), 13 (50%, 95% CI 30.8 to 69.2%) had negative IgA anti-gliadin and 12 (46.2%, 95% CI 26.8 to 65.2%) had negative IgG anti-gliadin. Even when combining anti-tTG with IgG and IgA anti-gliadin antibodies to improve sensitivity, five patients (19.2%, 95% CI 3.9 to 34.1%) had completely negative serology and six (23.1%, 95% CI 6.8 to 39.2%) had equivocal serology results (Table 1). None of the patients had been placed on a gluten-free diet prior to serology testing.
Serology results in patients with positive biopsies (n = 26).
Discussion
A recent prospective study showed that of 2,000 patients with suspected coeliac disease, 0.4% (7/2,000) had anti-tTG negative coeliac disease, and of those diagnosed with coeliac disease on histological criteria, 9.1% (7/77) had negative anti-tTG serology.8The laboratory techniques used at this hospital are standardised and similar to those used in most hospitals in the country. The retrospective study demonstrates that some cases of coeliac disease will be missed by relying on serological tests alone (see case history), and suggests that there may be an even more significant discrepancy between serology and histology, even when serological test are combined.
Some explanations for the discrepancies seen between the serological and histological results in this study might be:
the results are based on only a small number of positive biopsies
anti-gliadin antibody is a better marker of adherence to a gluten free diet than for the diagnosis of coeliac disease
there may have been laboratory errors
the published predictive values of the antibody tests quoted above may be those of tertiary centres that specialise in coeliac disease and are not representative of results produced by laboratories in district general hospitals.
However, we think it is unlikely that these factors would account for more than a small portion of the discrepancy seen.
Clinicians have grown increasingly to rely on serology for the diagnosis, and more importantly for the exclusion of coeliac disease. This study shows that a small but significant number of cases will be missed by relying on serology alone. If these findings are replicated across the UK a sizeable number of patients will continue to suffer the consequences of untreated coeliac disease (as demonstrated by the case history). Gastroenterologists are familiar with the more protean symptoms of coeliac disease but general physicians and primary care doctors may be less familiar with the varied presentations of the condition or the pitfalls in diagnosis. As the diagnosis and management of disease shifts ever further towards general medicine and primary care, it is important that the limitations of serological testing are recognised by all physicians. Where there is doubt about the diagnosis it is recommended that the opinion of a gastroenterologist be sought and duodenal biopsies be performed.
Case history
A 51-year-old taxi driver had attended outpatient clinics for many years with symptoms interpreted as IBS characterised by intermittent bouts of abdominal pain and diarrhoea. He had had these symptoms for over 25 years. He had previously been referred to the surgical outpatients in 1999 and a gastroscopy, flexible sigmoidoscopy, barium enema and abdominal ultrasound scan were unremarkable. More recently he had lost a stone in weight and developed iron deficiency anaemia and was referred to the gastroenterology clinic. His coeliac antibodies (anti-gliadin IgA/IgG and anti-tTG IgA) performed on 17 May 2005 were negative. A repeat endoscopy on 3 June 2005 showed grossly abnormal duodenal mucosa with a mosaic pattern and duodenal biopsies confirmed the presence of coeliac disease (Fig 1). A gluten free diet resulted in the resolution of his anaemia and symptoms and a weight gain of 15 kg.
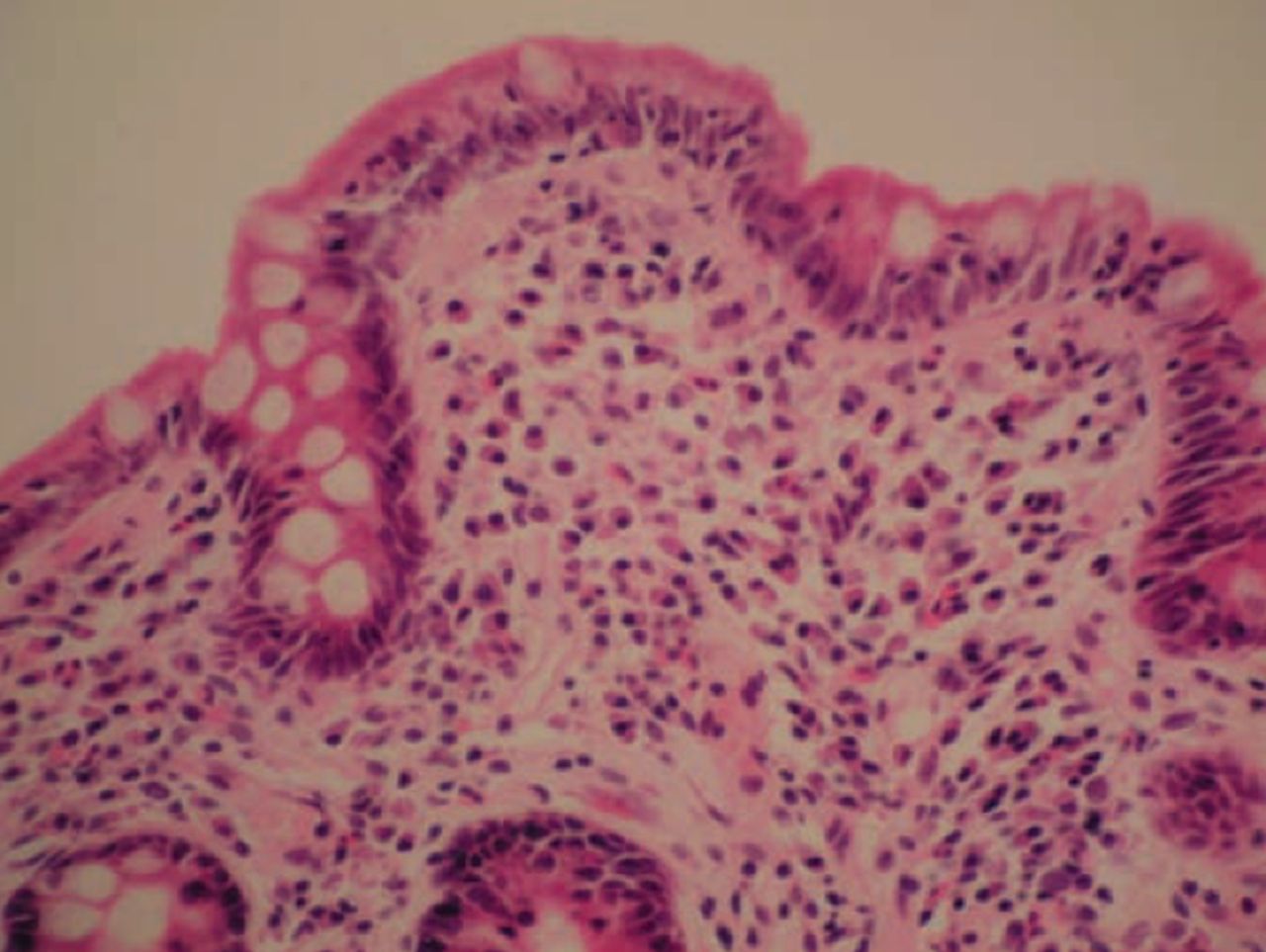
Haematoxylin-eosin stained celiac epithelium showing the characteristic infiltration of intraepithelial lymphocytes and flattened villi.
Acknowledgements
We would like to thank Dr Matthew Johnson, Consultant in Gastroenterology, Luton and Dunstable Hospital and George Taylor, Lead Lab Manager in Immunology and Histology, Medway Hospital, for their help and advice.
- © 2009 Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.