
Lesson 1
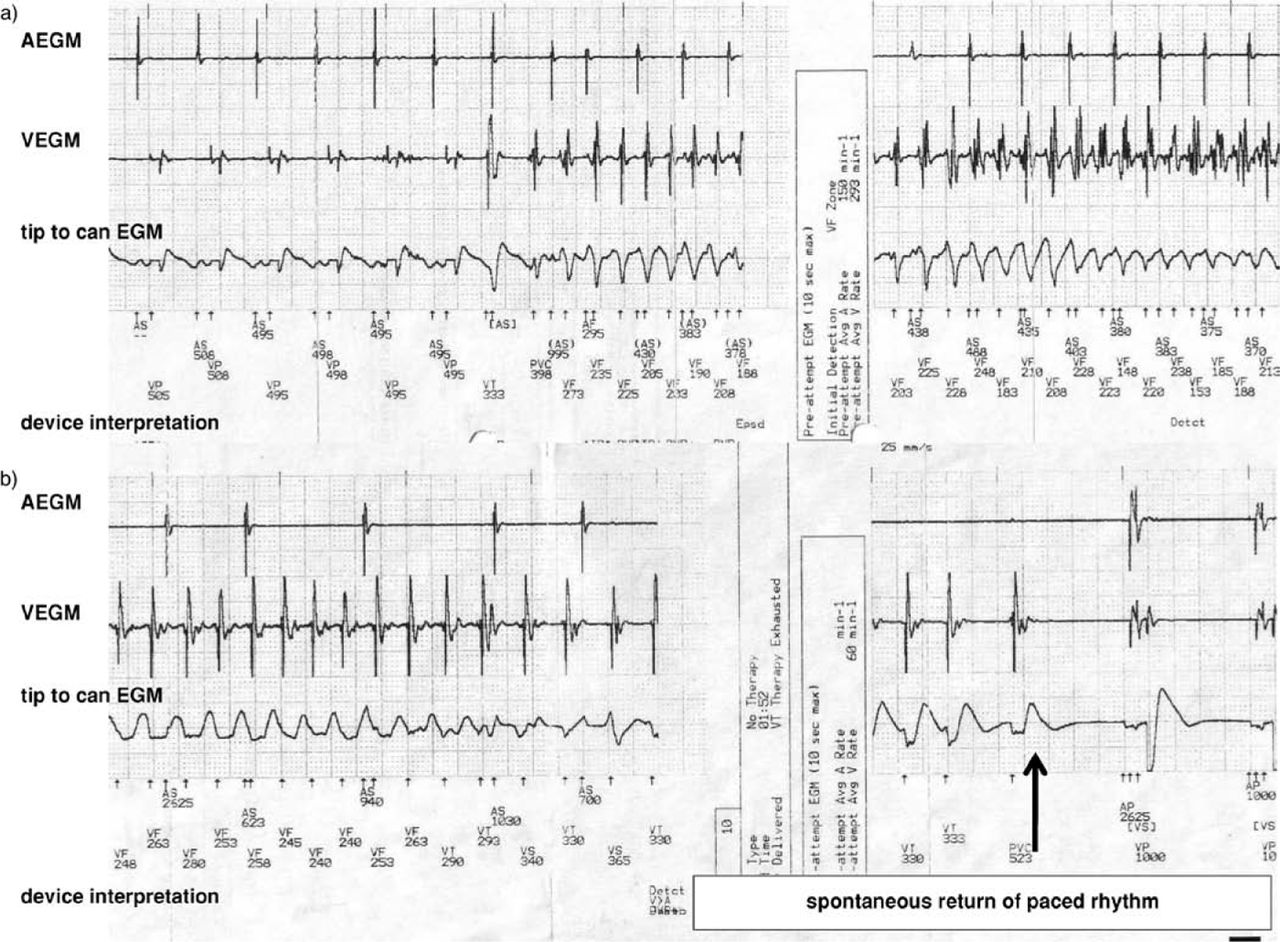
A 52-year-old man with ischaemic heart disease had a biventricular cardioverter defibrillator (CRT-D) implanted electively for symptomatic heart failure. Three months later, he presented as an acute medical emergency. He had woken confused, having apparently fallen out of bed. He could not control his hands, but was able to dial 999 using his thumb. He crawled to the door, and was taken to hospital by the ambulance service. On admission, he had a headache, but no neurological deficit. It was noted that there was a ‘pacemaker in situ’ and that there were pacing spikes on the electrocardiogram (ECG). A differential diagnosis of transient ischaemic attack or seizure was made. He quickly recovered and was discharged home the same day with an appointment to attend a ‘first seizure’ clinic, where it was felt that the episode was unlikely to be a seizure. No further investigations were arranged and he was discharged. Three months later he attended a routine defibrillator clinic appointment. Interrogation of the device revealed 2 minutes 23 seconds of ventricular fibrillation (VF) corresponding to the time of his collapse. In total, seven defibrillator discharges were delivered by his device; all failed to cardiovert him to sinus rhythm (Fig 1a). He spontaneously reverted to sinus rhythm after the last shock had been given (Fig 1b). A high defibril-lation threshold was diagnosed; his defibrillator was revised, and successfully cardioverted VF to sinus rhythm on repeated testing. The patient remains well and shock free at follow-up.
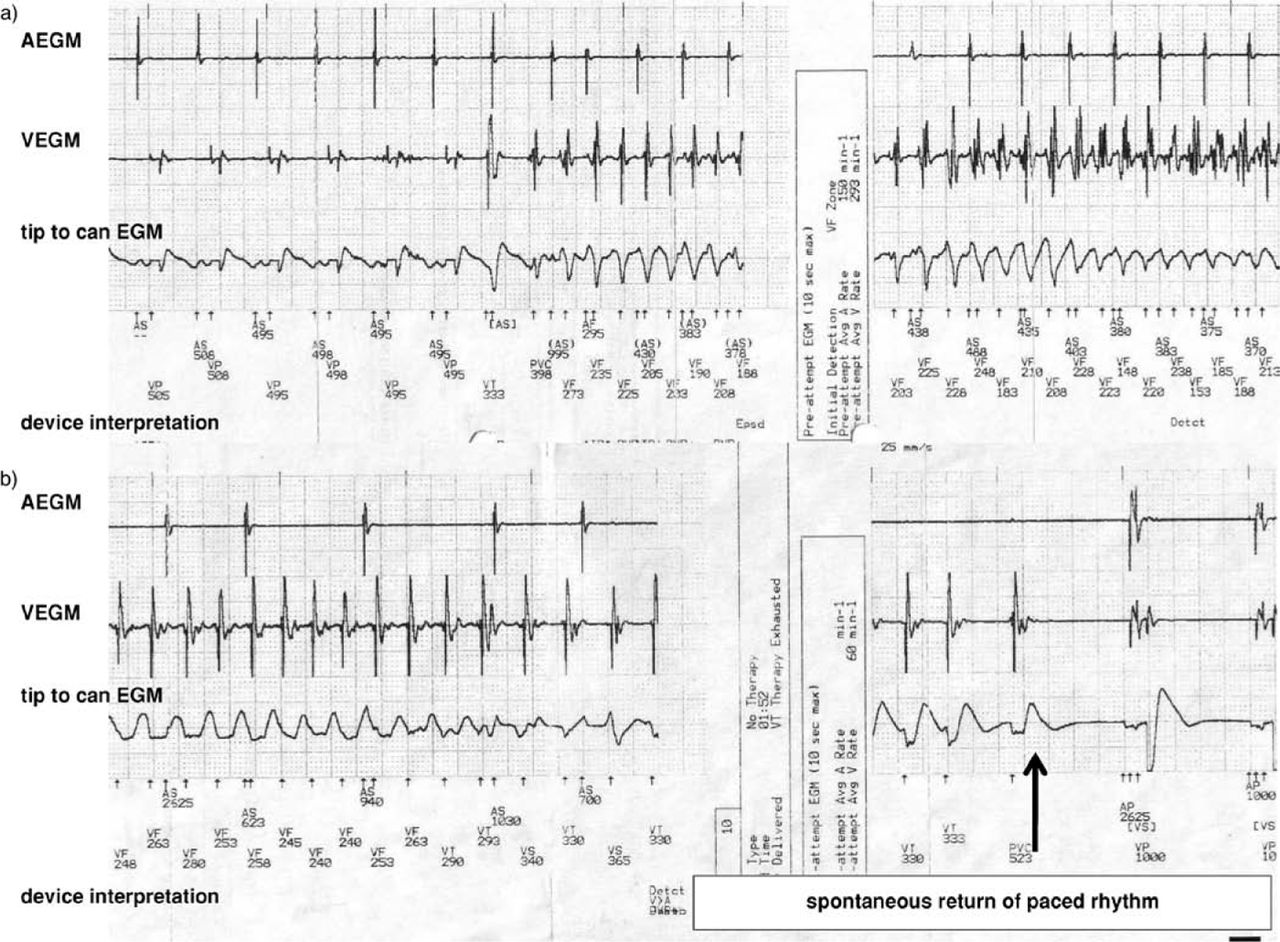
(a) the CRT-D tracing and a 31 Joule device discharge that failed to cardiovert the ventricular fibrillation (VF). The letters indicate the device readings: AEGM = atrial electrogram; VEGD = ventricular electrogram; with the device interpretation of the atrial and ventricular activity ‘AS’ indicates the device sensing atrial activity, ‘VP’ indicates ventricular pacing and ‘VF’ indicates sensing of ventricular fibrillation from the ventricular lead. (b) the spontaneous return of paced rhythm after 2 minutes 23 seconds of VF. The device records atrial activity from the atrial electrogram, VF in the ventricular electrogram then spontaneous atrial pacing (AP for the device interpretation) and ventricular pacing (VP in the device interpretation) after the failed delivery of a seventh attempt at cardioversion.
Lesson 2
A 64-year-old man who had had a heart transplant 16 years previously, followed by permanent pacemaker implantation for atrioventricular block, presented to his general practitioner after three apparent seizures in one day. He was admitted later that night as an acute medical emergency, following a fourth seizure and a 999 call; at least two of the seizures being preceded by a feeling of faintness. An ECG was recorded, and noted to show a paced rhythm. A head computed tomography scan was requested. A further seizure was witnessed 48 hours later during which it was recorded that a pulse could not be palpated. Telemetry was commenced. Thirty minutes later he had a further seizure preceded by a feeling of faintness, during which pacemaker spikes without capture were noted. A diagnosis of pacemaker failure, subsequently shown to be due to a high ventricular pacing threshold, was made. After revision of his pacemaker, he remains well and seizure free.
Discussion
Syncope may be accompanied by convulsive movements, when cerebral hypoxia occurs.1,2 This can lead to confusion with epilepsy.3Diagnosis of the precise cause of syncope may be difficult, but cardiac causes are more common than epilepsy.4It has been suggested that a patient with syncope and either preceding faintness or palpitation, an abnormal ECG, a history of structural heart disease, or a family history of sudden cardiac death should be referred initially to a cardiologist for investigation.1
Both patients were initially referred for neurological investigation, despite both having a significant cardiac history and implanted devices. The correct diagnosis was made by either telemetry or interrogation of the device. These cases highlight how careful history taking and investigation, with device interrogation if necessary, is vital in patients with a history of cardiac disease, who present with a sudden loss of consciousness. Modern pacemakers provide sophisticated diagnostic capabilities and interrogation may reveal the diagnosis.
- © 2009 Royal College of Physicians








{kind=link}