
- adverse drug reaction
- cohort-event monitoring
- individual case safety report
- longitudinal electronic patient records
Medicines improve health and the chances of survival in a wide variety of conditions. At the same time, no substance with pharmacological effects is without hazard. Adverse drug reactions (ADRs) can be associated with the intended pharmacological effect of the medicine (eg bleeding from warfarin), mediated by other mechanisms (eg anti-cholinergic effects of tricyclic antidepressants) or can be altogether unexpected (eg hypersensitivity reactions to abacavir).
Some ADRs can be identified early in the development of a medicine, but knowledge of the adverse effects profile is provisional when the medicine is first marketed and usually changes over time. Premarketing clinical trials include too few patients and are too short to detect every outcome that will affect public health and individual patient safety. In addition, clinical trials are carried out in controlled settings that differ from real-world practice. This reduces their power to detect ADRs, for example those that are due to drug-drug interactions or that affect only susceptible subgroups (eg phocomelia due to thalidomide). Safety needs to be evaluated continuously throughout the life-cycle of a medicinal product.1,2 A key challenge is to identify emerging problems as early as possible, without generating false alarms.
Individual case safety reports
Individual case reports (technically, ‘individual case safety reports’, even though they deal with harms) include reports to national regulatory authorities, such as the yellow card system of the pharmacovigilance section of the UK Medicines and Healthcare products Regulatory Agency and anecdotal reports in medical journals. They communicate genuine concerns about real-life suspected ADRs.3 Their strength in signalling causal associations between medicinal products and adverse events depends on the skill and experience of the reporter and the documentation and characteristics of the event, including its time-course and the effect of withdrawing and/or reintroducing the suspected medication.3 Most safety alerts are based on accumulated information from several independent sources, but strong and well-documented case reports can occasionally motivate action in their own right.4,5 On the other hand, early warnings of potential ADRs are possible in the absence of convincing index cases if there is no plausible explanation for an apparently excessive reporting rate of an event.6 Case reports represent the first line of evidence and provide powerful means of recognising the unexpected.7 Their status as a cornerstone of drug safety surveillance is clear. For example, they were the most commonly cited support for regulatory action to withdraw medicinal products from the UK and US markets between 1999 and 2001.8
Clinical review of case reports
Collections of individual case reports are complex and heterogeneous. Not all reports are submitted to pharmacovigilance systems by health professionals (such as doctors, dentists, nurses and pharmacists). Some are published in journals and others emerge in association with lawsuits. Direct patient reporting provides additional opportunities and challenges. The quality of reports is variable, and some important information is available only in the form of free text, and not as structured database fields. Detailed clinical review is therefore essential for effective knowledge discovery.
At the same time, clinical review constitutes the primary bottleneck: large national and international organisations collect hundreds of thousands of reports each year, every one of which cannot possibly be reviewed by the available experts. For example, the World Health Organization (WHO) Programme for International Drug Monitoring currently holds over 4.7 million reports from 94 countries with around 300,000 added each year.
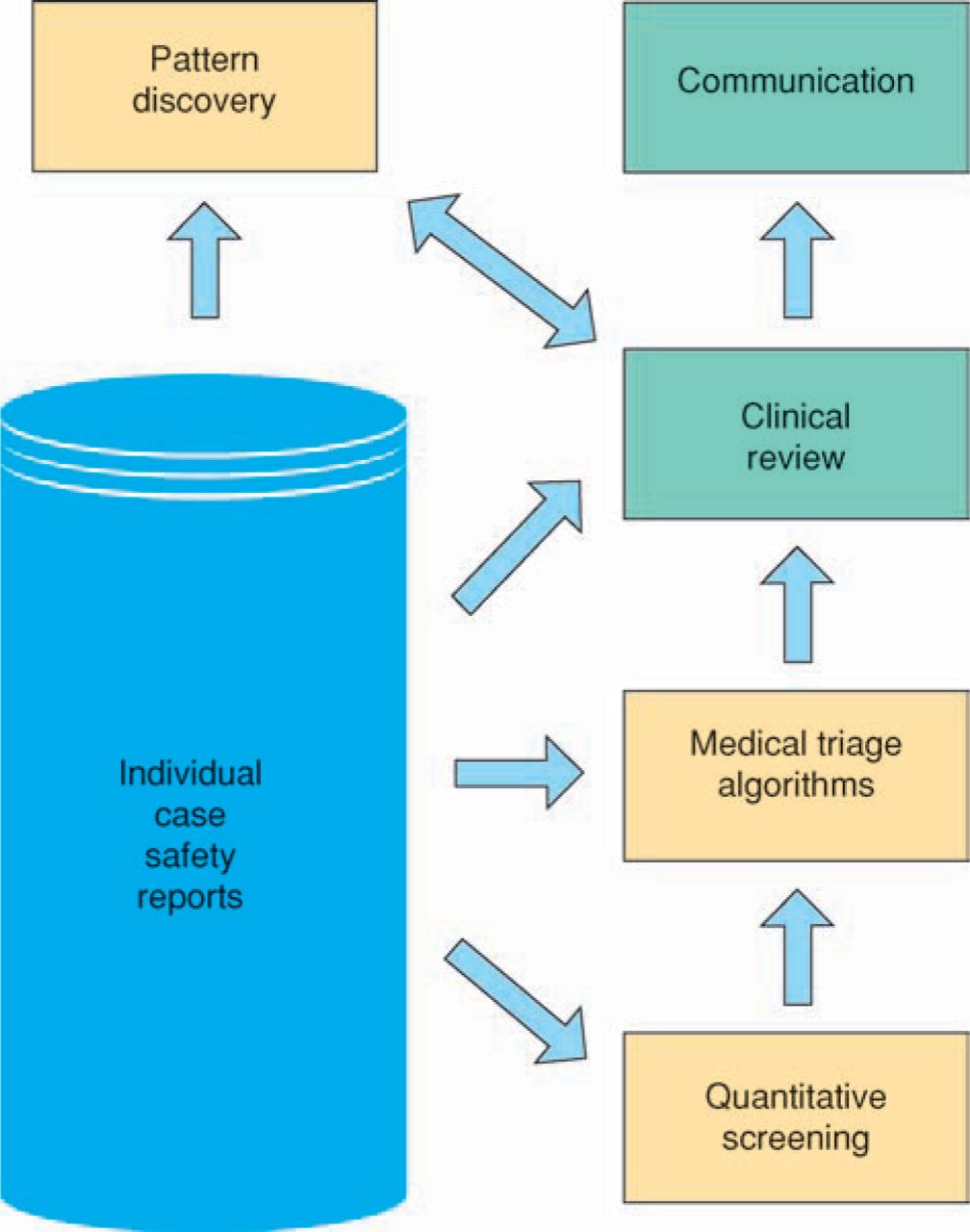
Even if each report could be reviewed, important reporting patterns would be missed in the vast amounts of data involved. Computational methods have therefore been developed to help highlight the most urgent problems for clinical review9–12 and to identify complex patterns such as those that suggest drug-drug interactions13 or clusters of related reports.14 Predefined triage helps prioritise outstanding reporting patterns based on their clinical relevance and urgency.15 Figure 1 shows a schematic overview of the process used in the WHO programme. Table 1 lists some problems highlighted prospectively by this approach.
Problems prospectively highlighted by quantitative screening of individual case reports, later communicated to national pharmacovigilance centres and relevant pharmaceutical companies, and finally supported by scientific publications or changes to the official product safety information.
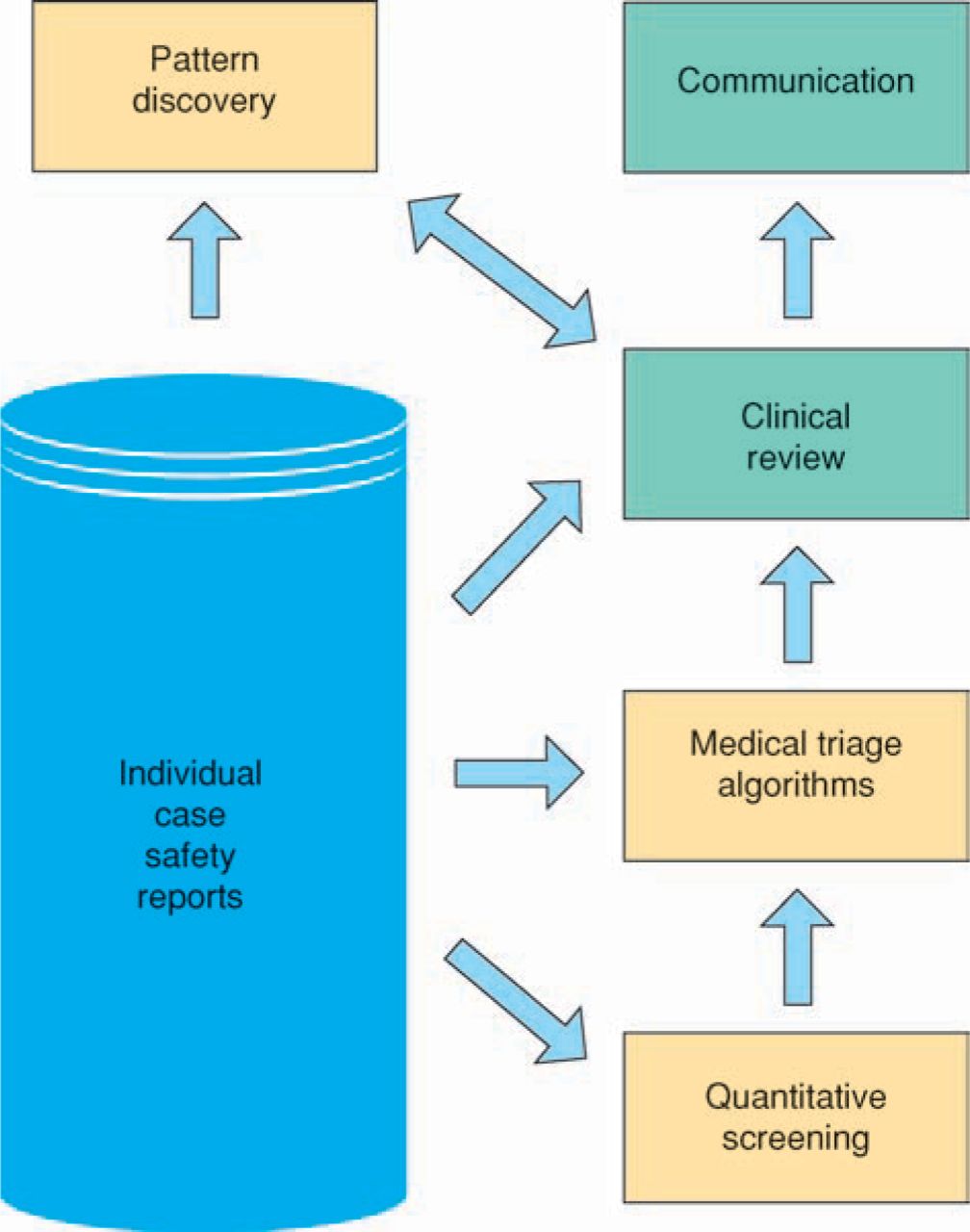
Schematic overview of the knowledge discovery process for individual case reports of suspected adverse drug reactions used in the World Health Organization Programme for International Drug Monitoring.
Key points
Safety needs to be continuously evaluated through the lifecycle of a medicine
No single method can be relied upon exclusively in global adverse drug reaction surveillance
Individual case reports represent the first line of evidence and provide powerful means of recognising the unexpected
Cohort-event monitoring allows quantification of adverse event rates and solicits information on events that may not otherwise be reported
The analysis of longitudinal patient records can detect a wide variety of temporal patterns relating medical diagnoses to drug prescriptions
Individual case reports bring health professionals and consumers into the process of regulating the medicines they use and also encourage individual educational feedback and sharing of important observations. Recurrent reports of known ADRs may convey an important message about how much prescribing physicians know about a given ADR.
Cohort-event monitoring
To complement individual case reports, some countries have implemented cohort-event monitoring (CEM) systems for intensified follow-up of selected medicinal products. Examples include New Zealand's Intensive Medicines Monitoring Programme16 and prescription-event monitoring in the UK.17 CEM encourages health professionals to report adverse events and solicits information about events that may not otherwise be reported. The cohort sizes typically range from a few thousand to tens of thousands of patients. The well-specified cohorts, together with encouragement to report all events, ideally allow incidence rates to be estimated and compared across medicinal products. The main limitations of CEM are its restriction to a small subset of medicinal products, the relatively small fraction (globally) of the population covered and the lack of data from unexposed patients. It may be especially valuable for ADR surveillance in places where there is no established pharmacovigilance system and the collection of individual case reports is not practicable, such as for major public health programmes in developing countries.
Longitudinal electronic patient records
Collections of longitudinal electronic patient records are extremely valuable but underused in analysing real-world use of medicines. They cover large populations, provide detailed information on extended parts of medical histories and include information on both exposed and unexposed patients. The range of clinical information available may include prescriptions, laboratory test results, hospital referrals and admissions, and notes on symptoms, signs and diagnoses. Ideally, anonymised information is extracted directly from the computer systems in which physicians store patients’ data, so that no extra effort is required to provide the information and the risk of omissions is minimised. Privacy protection for patients and physicians is of the utmost importance and needs to be carefully controlled. In the UK, general practitioners’ records provide an important source of information and have formed the basis of the General Practice Research Database,18 the IMS Disease Analyzer and the Health
Improvement Network datasets. Relative to individual case reports, patient records carry more complete information on the medical history, potential susceptibility factors and other medications taken before and after the event of interest. They do not usually communicate explicit clinical concerns (although suspected ADRs are sometimes identified) so associations must be inferred from the time-course of events.
Screening patient records
Patient records are already an important resource for confirmatory pharmacoepidemiological studies. In recent years interest has increased in extending their use to exploratory analysis and routine drug surveillance.19–21 Many methods focus exclusively on one specific aspect of the drug-event association, such as the time from first exposure to the medicine to the first occurrence of the event19 or differences in the frequencies of the event in the same patients when exposed and unexposed.21 However, there is great variation in temporal patterns of potential interest, including those related to:
suspected ADRs22
potential beneficial effects of medicines
events related to the underlying disease
periodic patterns and trends, and
medical events that are generally common in exposed patients.
Graphical presentation of temporal associations
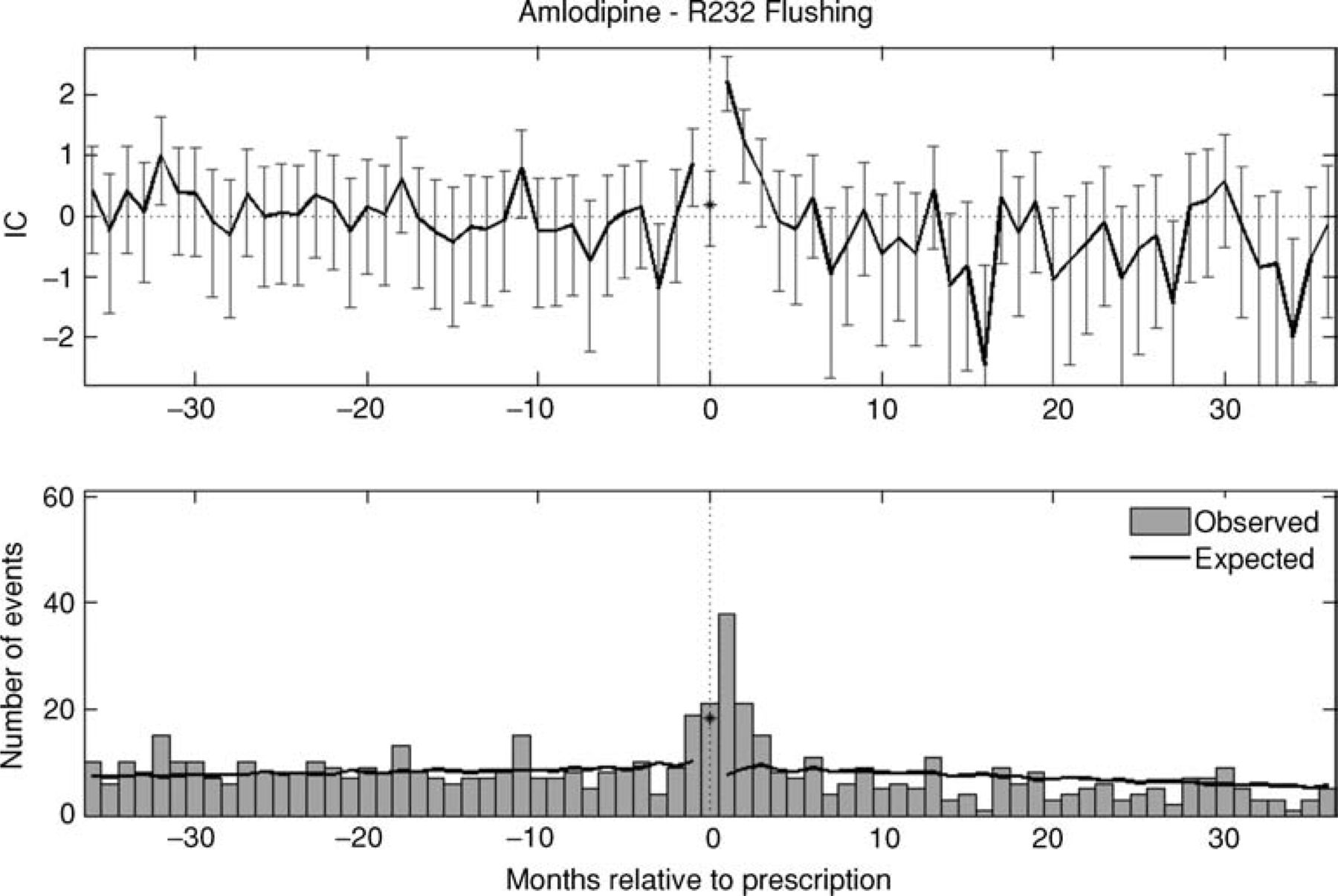
For true open-ended pattern discovery, extended parts of the underlying patient histories need to be studied simultaneously; it may be useful to present results graphically.20 As an illustration, Figs 2 and 3 present examples of a transient and a persistent temporal association, respectively, identified in a large collection of UK electronic patient records. The graphs indicate the recording rates of the medical event in different time frames relative to first prescriptions of the medicine (at time zero). The bottom graph in each figure displays observed and expected numbers of events, where the expected value accounts for the finite length of patient histories and the tendency of doctors’ visits to cluster in time.20 The top graph displays the logarithm of the ratio between the observed and expected number of events (with a variance-stabilising transformation) so that positive values correspond to higher than expected registration rates and vice versa. In the same spirit as the self-controlled case series design,21 patients are used as their own controls to isolate temporal associations from underlying characteristics of those receiving the medicine, such as the indication for treatment.
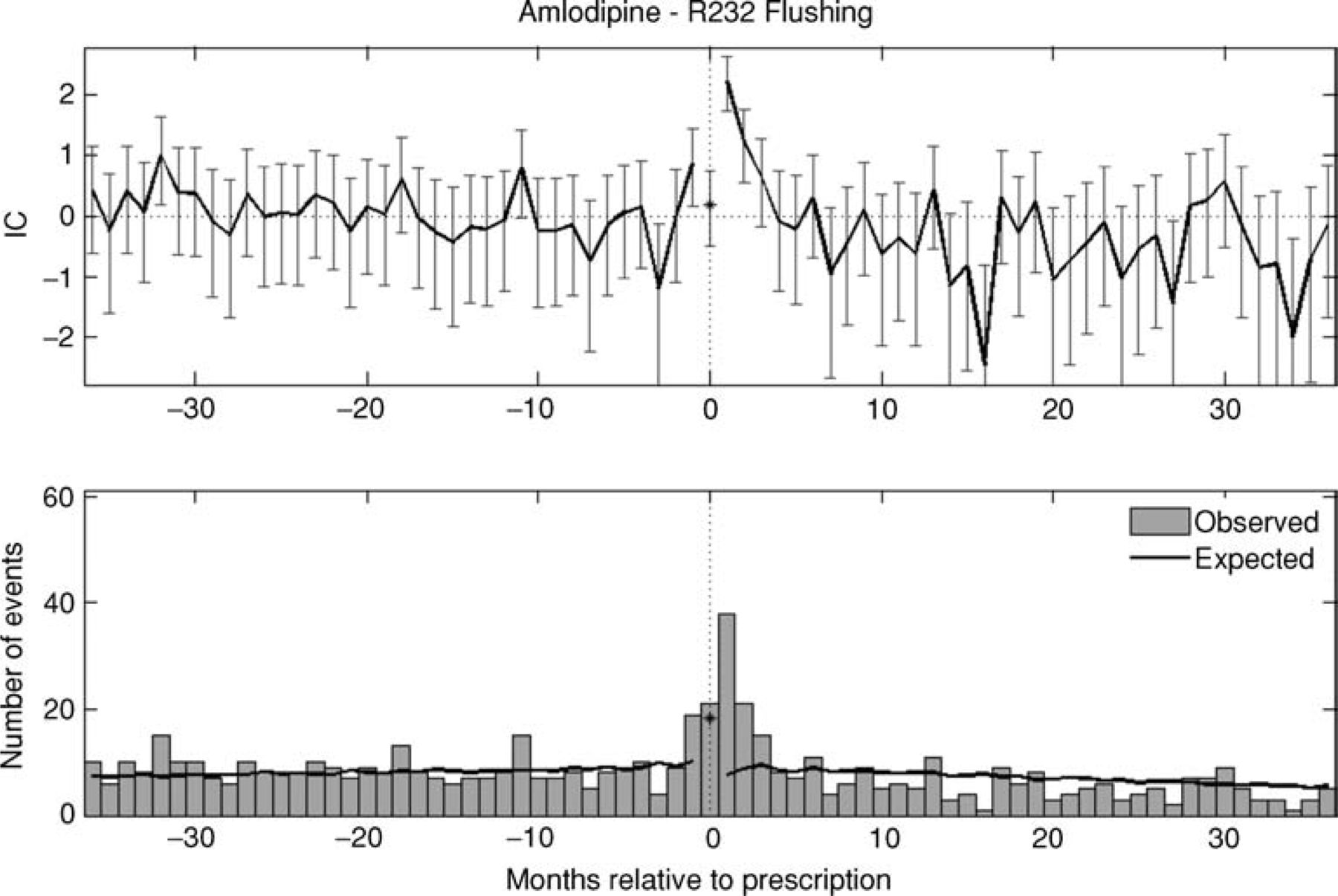
Example of a transient increase in the recording of a medical event subsequent to prescription in longitudinal electronic patient records; flushing subsequent to nifedipine is a transient effect. The upper graph displays a smoothed version of the logarithm of the ration of the observed to expected number of events. IC = information component.

Example of a persistent increase in the recording of a medical event subsequent to prescription in longitudinal electronic patient records; peripheral oedema subsequent to nifedipine persists. The upper graph displays a smoothed version of the logarithm of the ratio of the observed to expected number of events. IC = information component.
Conclusions
No single method can be relied on exclusively for global ADR surveillance. Individual case reports have considerable value in eliciting the observations of those who use medicines in their daily lives, including information on medication errors, drug-drug and drug-food interactions, and susceptibility factors. CEM allows quantification of adverse event rates and is better than individual case reports in detecting ADRs which might not be obvious to health professionals or patients. Longitudinal patient records allow comparisons of cohorts of exposed patients with themselves as controls when they were not exposed to the medicine (particularly before treatment). Together, these three sources of information allow hazards to be detected at an early stage. Further evaluation may require specifically targeted and powered observational or experimental studies.
- © 2009 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}