
Lesson
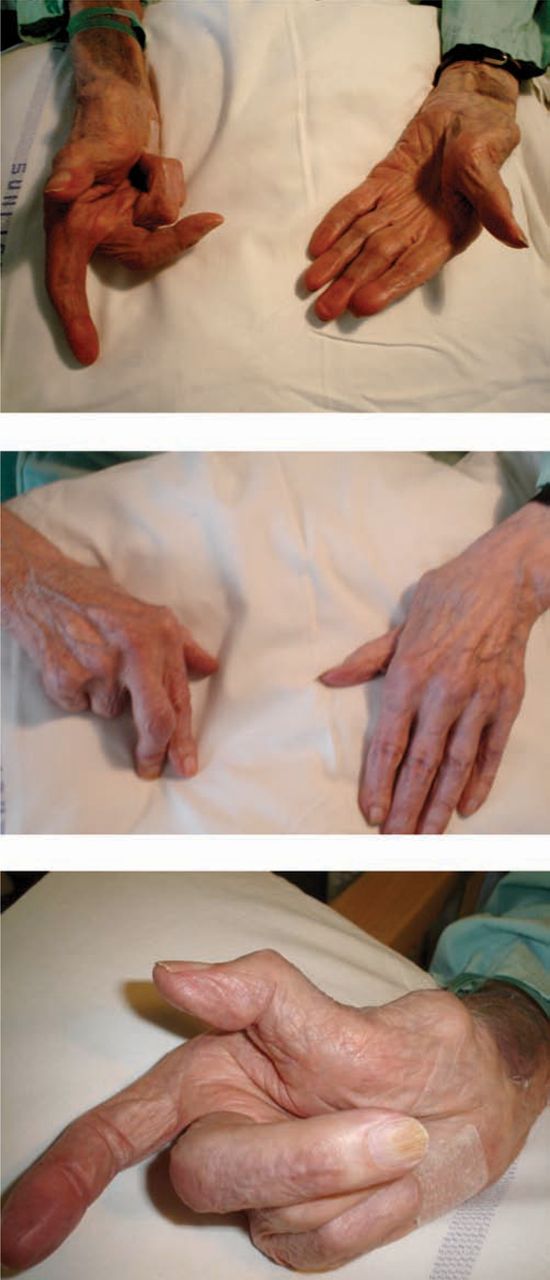
Mr AP, an 89-year-old man presented to accident and emergency with a three-day history of shortness of breath and a cough. He was diagnosed to have a severe pneumonia requiring inpatient treatment. On the ward round the following day, his hands were examined (Fig 1). They had several features of rheumatoid arthritis (RA), although on close questioning Mr AP denied any history of arthritis. Rheumatoid-looking hands feature commonly in clinical examinations. Symptoms and signs of this condition were first described in 1800 by Landre-Beauvaise.1 The photographs show some of the classical hand deformities present in a patient with rheumatoid arthritis: ulnar deviation, Z finger deformity of the thumb and swan neck deformities.

Mr AP's hands at presentation.
Apart from clinical history (symmetrical polyarthropathy presenting classically with early morning stiffness) and examination findings, there are several laboratory and radiological investigations that help consolidate the diagnosis of RA. Mr AP was negative for rheumatoid factor (RF) (sensitivity 69% and specificity 85%).2 X-ray and better still magnetic resonance imaging (MRI) scans of rheumatoid hands reveal synovitis, tenosynovitis, erosions and bone marrow oedema as diagnostic features.3 Mr AP's MRI scan was negative for these features. So what are the other differentials for these rheumatoid-looking hands?
Tuberculous (TB) tenosynovitis has been found to exhibit many typical signs of RA which improve with anti-TB treatment.4 The diagnosis is usually made from microscopy and culture of synovial fluid. Erosive osteoarthritis (OA) can also clinically exhibit features of RA.5 However, OA in contrast to RA is usually associated with asymmetrical joint involvement, symptoms worsening as the day progresses and Heberden's nodes present on the hands. Typical radiological findings of OA include osteophytes, joint space narrowing and subarticular sclerosis.
Among its many manifestations, psoriatic arthropathy can present as a symmetrical deforming arthritis affecting mainly the distal joints of the body (hands, feet, wrists and ankles). Clinically, it shares several corresponding features of RA but also has its own distinctive manifestations (dactylitis, enthesis, distalinterphalengeal or sacroiliac joint involvement). It is RF negative and may display characteristic nail changes. Radiological features demonstrate a combination of joint erosion and bone growth (unlike RA).
Jaccoud's arthropathy (JA) is another chronic joint deformity characterised by ulnar deviation of the second to fifth fingers and subluxation of the metacarpophalangeal (MCP) joints. It was initially described as a complication of rheumatic fever but was later found to be associated with other connective tissue disorders chief of which being systemic lupus erythematous.6 In its early stages, many of the joint deformities can be voluntarily corrected by patients. JA may also affect toes and rheumatoid nodules are frequently present. Fibrosis of the periarticular tissues with abnormal synovium is the principal pathologic feature.
Case reports have also described clinical signs such as ulnar deviation, flexion of the MCP joints and hyperextension of the interphalangial joints in non-rheumatoid patients with Parkinson's disease.7
Mr AP did not have any of the above causes of rheumatoid hands. His MRI scan, while excluding RA, did however demonstrate multiple tendon ruptures. We were unable to determine the aetiology of these tendon ruptures, however, he worked as a tool maker for many years and this may have contributed to the hand deformities. Multiple tendon ruptures can lead to clinical features of RA.
- © 2009 Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.