
Abstract
Prescribing errors are a recognised problem on admission to acute medical wards which may be detrimental to patient care. The authors had anecdotal evidence that prescribed medicines do not always reach patients and the aim of this audit was to quantify this problem. Admission prescription charts on two separate occasions were studied in detail and all drugs prescribed but not given in the first 48 hours were recorded along with the reason given for omission. In total, 271 patient charts were analysed. Of these, 20% of prescriptions affecting 17% of patients did not reach patients. The two dominant reasons for medications not being given to patients were that the medication was not available on the ward (38% of omissions) or that the patient was nil by mouth (32% of omissions). In 10% of cases the patient refused the medication, in 19% no reason for omission was given and in only a minority (0.3%) was the patient off the ward. This audit demonstrates that even when medications are prescribed they are not always given. This may lead to increased morbidity and length of stay. Strategies need to be put in place to reduce this problem. The current system that permits omission of medications with inadequate justification must be revised.
Introduction
Patients admitted to hospital acutely under general physicians are by their very nature a diverse and unwell population. The vast majority have co-morbid conditions that are usually stable on established medication regimes. The number of medications taken is increasing with the median number taken when admitted rising from two in 1994 to four in 2004.1 Sudden cessation of these medications, whether related to the admitting condition or not, may have a negative impact on morbidity. A number of factors have been recognised which potentially lead to patients failing to get their medications:
they may be unable to recall their usual medications
previous records may not be available or if they are available on admission may not contain up-to-date information
prescribing errors may lead to omission.
The National Patient Safety Agency (NPSA) has recently published strategies to address these issues.2 However, in addition to the recognised causes the authors have observed anecdotal cases where medications have been prescribed but have not reached the patient leading to worsening of the presenting condition or of a previously stable co-morbid condition. In one case a specific nitrate, which a patient was using regularly to control angina, was prescribed but was unavailable in the hospital and the patient did not receive any oral nitrates for 48 hours despite being admitted for chest pain. In another case a patient with stable heart failure was admitted with sepsis of urinary origin and treated with antibiotics, but an angiotensin-converting enzyme inhibitor not on the hospital formulary was unavailable and he developed pulmonary oedema several days after admission as a result of the omission. A small previous audit in 2004 (unpublished) suggested that this might be a substantial problem. As a result an audit was conducted to assess the frequency of failure to receive prescribed medications (where a prescription is a single medication on the drug chart) in the first 48 hours of admission to a UK general hospital, the reasons for omission were ascertained and any potential relevance of the omission examined.
Methods
The study was carried out over two separate days in 2006/7. All the prescription charts on medical patients in hospital on the audit days were reviewed. Admission prescription charts were studied in detail and all medications prescribed but not given in the first 48 hours were recorded along with the reason given for omission. Medications were categorised according to the British National Formulary classifications. Nursing staff routinely record reasons for omissions under seven categories (patient vomiting, no cannula, patient not on ward, patient nil by mouth, patient refused, drug not on ward, and other). Patient demographics and the reasons for admission were also noted. An assessment was made of the relevance of the omitted medication to the presenting complaint and any adverse events possibly related were noted.
Results
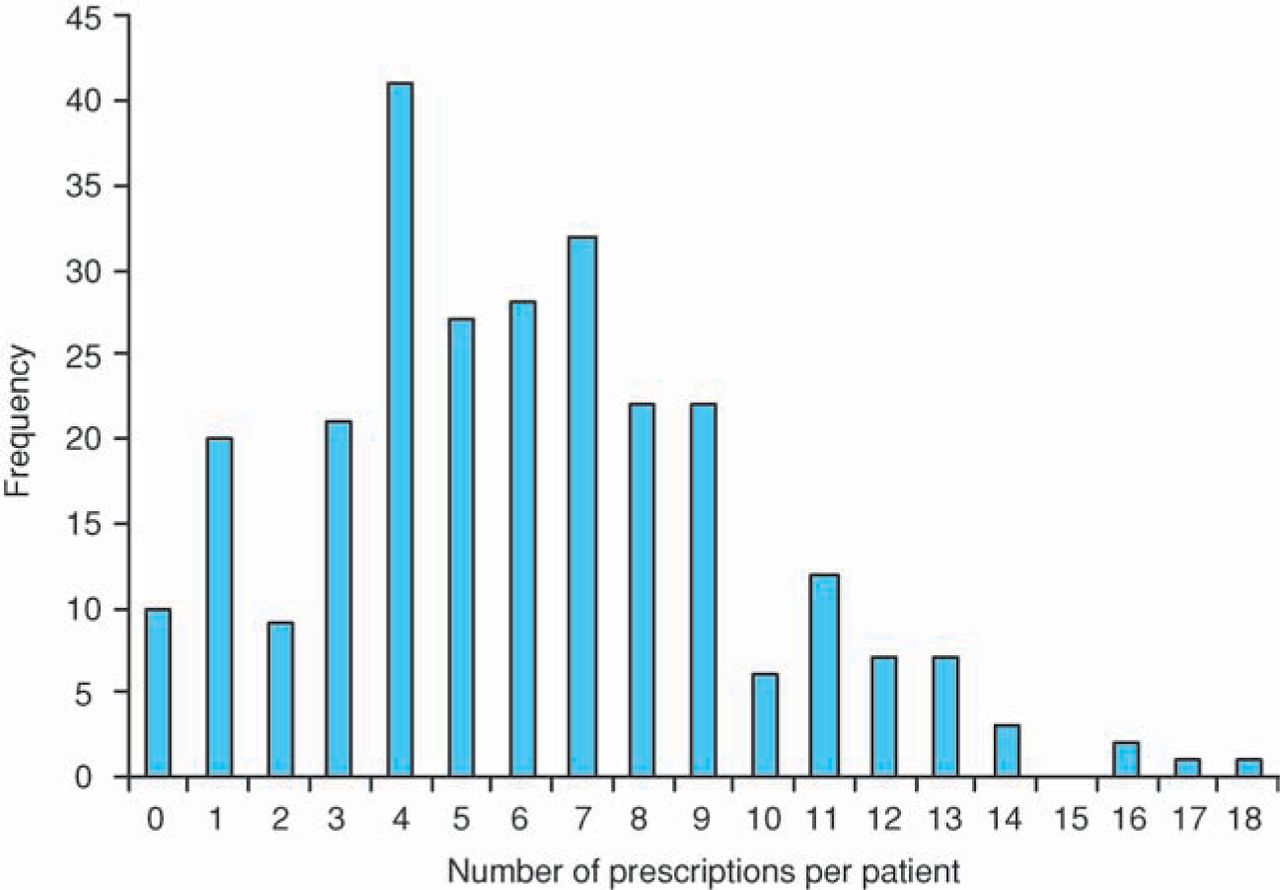
One hundred and fifty-seven patient files were assessed on a day in December 2006 and 128 patient files were assessed on a day in February 2007. Complete data were not available on 14 patients and these were excluded from analysis. In total, 271 patients were included and analysed. Diagnoses and clinical conditions were varied as expected for an acute medical admissions unit of a district general hospital in the UK. The median age of patients was 78 (range 18–99) years. Fifty-three per cent were male. A total of 1,642 items were prescribed with the median of six (range 0–18) per patient (Fig 1). The range of medications prescribed was broad (Table 1). Of the prescriptions 329 (20%) had at least one dose omitted in the first 48 hours of admission. This affected 147 patients (17%). The maximum number of doses omitted in one patient was 18 comprising eight medications consisting of four doses of beclomethasone and two doses of aspirin, lisinopril, metformin, simvastatin, glibenclamide, frusemide and rosiglitazone.

Number of prescriptions per patient.
Omitted medications by British National Formulary (BNF) category.
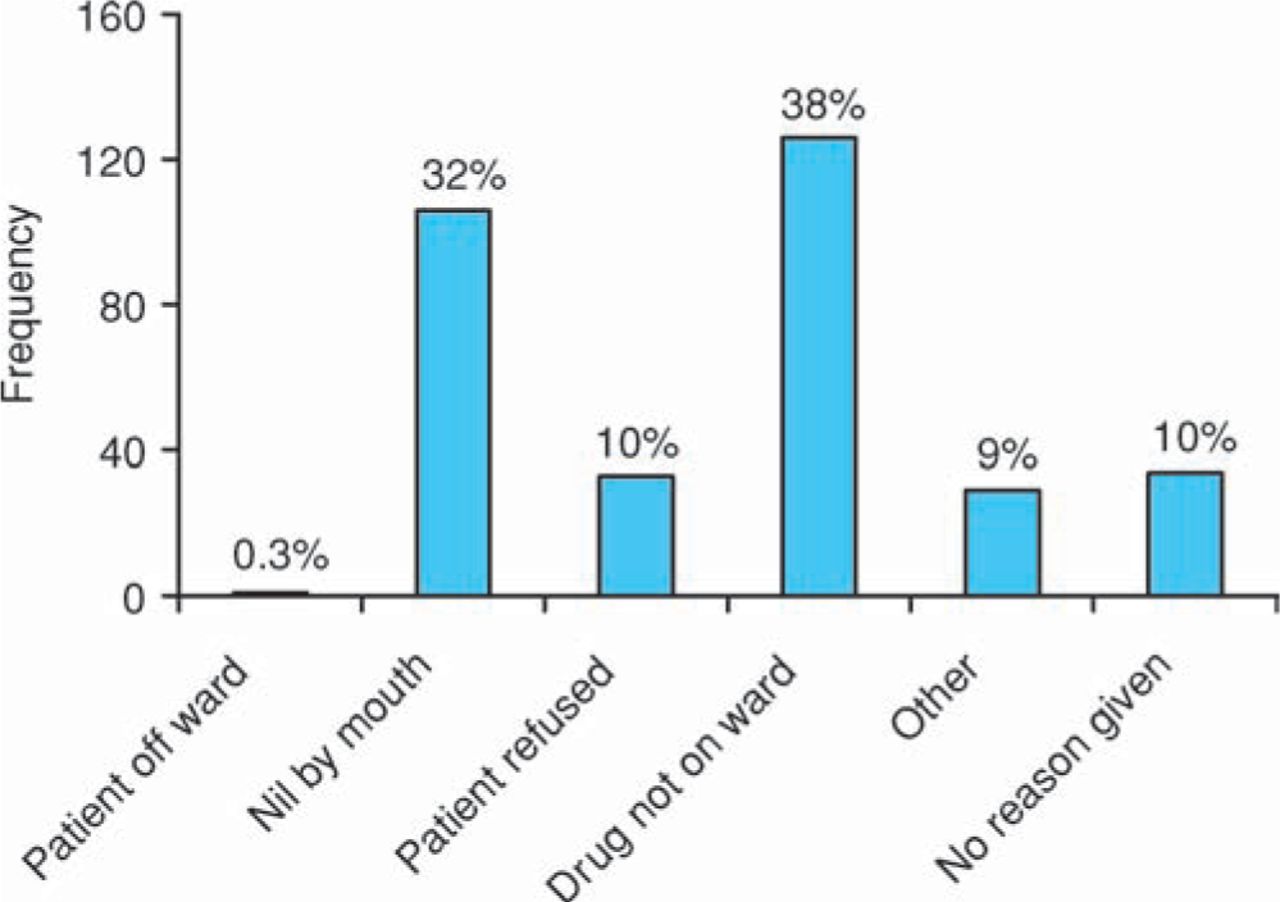
The two dominant reasons for medications not being given to patients were that the medication was not available on the ward (38% of omissions) or that the patient was nil by mouth (32% of omissions) (Fig 2). In 10% of cases the patient refused the medication, in 19% no reason for omission was given and in only a minority (0.3%) was the patient off the ward. There was no correlation between the day of the week admitted and the number of omissions of medication related to drug unavailability on the ward. In particular, weekends, when the pharmacy runs a minimal service, were no different from weekdays, when the pharmacy was fully staffed.
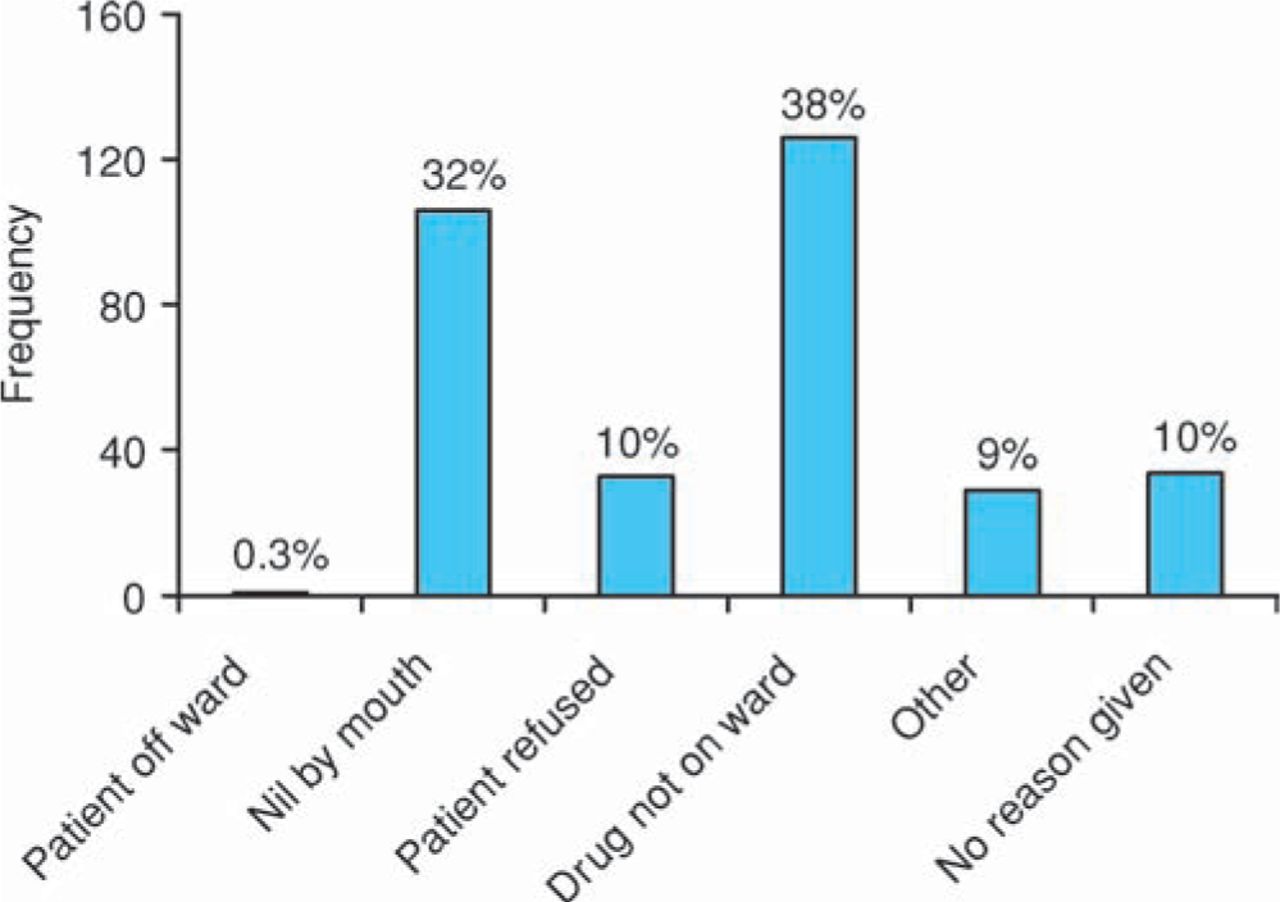
Reason for drug omission.
Relevance of omission
The auditing doctors assessed the relevance of the omitted medication to the admitting complaint. In 7% (19) of these patients the omission was deemed to be highly relevant (Table 2). The most outstanding examples include a patient with Clostridium difficile missing the first two doses of vancomycin, a patient with diarrhoea missing three doses of metronidazole for C. difficile treatment, and two patients with acute coronary syndrome missing enoxaparin. These medications are first line treatments and the omission of them might adversely affect outcome and length of stay. Not all omitted medications would have had an adverse effect on patient outcome. Examples of these include omission of Movicol® in an admission with falls and omission of amlodipine for hypertension in a patient with urinary tract infection.
Important drug omissions during first 48 hours of admission (drugs considered highly relevant by the auditing doctors).
Discussion
Patients admitted acutely to medical wards are a complex group with an acute problem and often multiple co-morbidities. Continuation of pre-existing medication is often essential to maintain control of these conditions.
Doctors are known to have difficulty gaining an accurate medication history on admission to hospital with discrepancies between actual and prescribed medications affecting between 10% and 67% of hospital admissions.3 The NPSA has recently addressed this problem and advised that policies should be in place for medication reconciliation on admission and that this should involve a pharmacist as soon as possible.2 The trust in this study has introduced a pharmacist to reconcile medications in newly admitted patients since the audit was completed. This study was not designed to assess the reconciliation process but to identify and quantify an alternative source of medication omission. The problem of reconciliation and prescribing is becoming increasingly difficult as the number of medications taken by patients increases, rising from two on admission in 1994 to four in 2004.1 This current study did not ascertain the number of drugs on admission but the mean number of prescriptions once admitted was six suggesting the trend continues. This is not surprising when one considers the ageing population.
This study sought to identify and quantify a previously rarely reported source of omission of prescribed medications. We have demonstrated that even when medications are prescribed they are not always given. Of the patients in this study 17% did not receive all of their prescribed medications in the first 48 hours (20% of prescriptions). In 7% highly relevant medications were omitted despite having been prescribed by the admitting doctors and this may have had serious consequences. A previous audit in 2004 (unpublished) revealed the same finding of 20% of prescriptions not being given. Dose omission from drug charts has previously been identified as a problem, affecting 12.6% of patients,4 in a study on electronic prescribing. The results of this audit, in a hospital that does not use electronic prescribing, reveal even worse omission rates, perhaps understandably since it related to the first and most difficult 48 hours of admissions.
The reasons for prescribed medications not being given to patients are multifactorial. In this hospital the nursing staff have a series of reasons available to them to record why they have not given prescribed medications. The most common reason being that it was not available on the ward and was the cause for 38% of omissions. The medication stocks held on wards have become more limited for a variety of reasons. During the day items can be ordered from pharmacy but this can take several hours during which time doses may be missed. Pharmacy ward rounds tend to occur in the morning and so seldom help patients admitted after noon. At night drugs on the hospital formulary are available from an emergency pharmacy store that can be accessed by senior nursing staff or doctors. However, the low number of nursing and medical staff on duty overnight means this system is seldom used. All this is probably compounded by lack of knowledge of the hospital formulary (which has become increasingly constrained over the last decade) by doctors who frequently rotate between hospitals with different formularies. The educational challenge to resolve this problem is enormous. Optimising the alignment of community and hospital formularies would lessen the risk of several of these causes of omission. It is to be hoped that in the future electronic prescribing might at least be able to flag up medications not readily available and offer potential alternatives. In the meantime, it may be prudent to provide a list of suitable alternative medications to simplify and encourage front line doctors to make safe changes. The problem is not solely related to doctors’ knowledge since some medications that were stated to be unavailable are in routine stock on wards suggesting a lack of nursing familiarity. The pharmacy in this study is addressing this issue by carrying out stock reviews on all wards.
Nursing staff need better protocols for when they are unable to give medications. This should involve giving the medication as soon as it does become available or informing the doctor or pharmacist if this fails. Medication being unavailable should not be a reason for omission, but should result in physician review to consider alternative prescribing. This may result in an increase in workload for junior doctors who are already busy.
The second reason for medication omission (32% of patients) was because the patient was flagged as being nil by mouth. ‘Nil by mouth’ is highly appropriate in some patients and prescribed medication should be by non-oral means or possibly via a nasogastric feeding tube. However, it appeared that many patients were placed nil by mouth for weak or temporary reasons and in most circumstances this should not prevent the giving of essential oral medication. Recent surgical evidence suggests that prolonged fasting (greater than two hours for fluids) is not necessary and omission of medications (especially cardiac medications) may be detrimental to outcome.5 Perhaps a new concept of ‘clear fluids and oral medications’ should be introduced for those who do not need to be strictly nil by mouth.
A patient refusing the medication resulted in 10% of omissions. This is obviously within the patients’ rights if they are not confused but staff must, whenever possible, ensure that these patients are making informed choices. Under the new Mental Capacity Act 2005 recording that a patient refused medication should perhaps be qualified by their fitness to make such a decision.6 For those who are unfit to make such a decision, their temporary lack of competence should be noted and nurses should do all they reasonable can to encourage compliance. Where capacity to make an informed decision is truly lacking a review of whether and how medications might be given (eg parenterally) should be undertaken by the medical team.
As in many hospitals the prescription charts in this audit permit an option of ‘no reason’ to be used as a reason for not giving a patient a medication. This accounted for 10% of omissions in this study. A reason should always be given and this option is unacceptable and should be removed. Similarly the option of ‘other’ is available as a reason and accounted for 9% of omissions. When accompanied by a reason this is acceptable but all too often nothing is documented and this is unacceptable.
‘Patient not on ward’ accounted for 0.3% of omissions and ‘patient vomiting’ was not recorded as a reason in this study. Both of these options should be removed. In general patients should be offered treatment on their return to the ward (for example after tests) or when vomiting has eased. The timing of medication taking, particularly of medication for co-morbid conditions is seldom critical to within an hour or two though there are exceptions eg anti-Parkinsonian medication. It is highly illogical to omit medications prescribed for the acute condition that caused the admission. Timings should not be solely dictated by the timing of the nursing drug round. Some education will be required to ensure this is applied safely since some medications might reach toxic levels if one dose is delayed and then given too close to a planned later dose (eg gentamicin).
Outcomes from omission can vary from insignificant to severe depending on the medication and the patients’ co-morbid and presenting conditions. There may be decompensation of the co-morbid condition and suboptimal treatment of the presenting complaint. Either could lead to an increased length of stay and though this may be small for an individual the frequency of omission suggests it may lead to significant organisational inefficiency. It is also noted that clinical incident forms are seldom if ever completed for medication omission. Perhaps omission of a prescribed medication alone, whatever the reason, should be flagged as a clinical incident though this would over-report on some acceptable practice. Conversely if only omissions which lead to patient deterioration are recorded under-reporting of this common problem is likely.
The problem of medication omission is common and compounds the problems of reconciliation discrepancies. They are likely to affect patient outcome measures and length of stay. Good solutions are likely to be multifactorial.
- © 2009 Royal College of Physicians








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Impact of a policy to improve the management of oral medications when patients are fasting before a procedure: an interrupted time series analysis
- Improving the supply of critical medicines from pharmacy to reduce the delay in medicines administration on wards
- Prevalence, nature and risk factors for medication administration omissions in English NHS hospital inpatients: a retrospective multicentre study using Medication Safety Thermometer data
- Efficiency analysis of a barcode-enabled and integrated medication-tracking system
- Omitted medications: a continuing problem