
Abstract
Older people in care homes are clinically complex and particularly vulnerable to the effects of poor care and poor medicine. They are also a group to whom the NHS seems least committed. Geriatricians have become disengaged over the past two decades, as a result of social policies rather than clinical judgements. In 2000, the Royal College of Physicians, with the Royal College of Nursing and the British Geriatrics Society, issued guidance and recommendations for improving clinical practice. This paper reports progress since then based on results of national surveys of geriatric medicine departments and primary care trusts in England. The results show that important deficiencies persist, though most respondents were in favour of greater specialist involvement. Some suggestions are made for ways to improve the shared care of residents in care homes.
- care homes
- continuing care
- comprehensive geriatric assessment
- geriatricians
- nursing homes
- old age psychiatrists
- older people
- physician's role
- specialist nurses
In 2007, there were over 350,000 people aged over 65 years resident in care homes in England.1 There are three levels of care home provision. The first is 24-hour personal care assistance without nursing which is funded by local authorities, subject to means testing, here referred to as residential care homes. The second involves 24-hour access to qualified nursing care, where the NHS funds the nursing component. This group are here referred to as care homes with nursing. The third level of care home provision is NHS continuing care, which provides more complex or intensive nursing and/or other healthcare both within care homes and specially designated long-stay institutions.2,3
People enter care homes for many reasons related to the loss of physiological, psychological, functional and social reserves. Guidance from the Royal College of Physicians (RCP), the Royal College of Nursing (RCN) and the British Geriatric Society (BGS) is that, before admission, an older person should be assessed for the presence of reversible factors, such as medical and rehabilitation needs, by a team including a physician skilled in geriatric medicine with the aim of preventing some of these placements.4–6 This recommendation is supported by evidence of effectiveness.7
Care home residents have ongoing and increasingly complex needs.8,9 A recent national census of 751 care homes revealed that 72% of residents were immobile or required assistance to mobilise, 86% had one or more diagnoses explaining the need for personal care, 54% of care need was related to dementia, stroke or Parkinsonism, and 24% had the ‘unholy trinity’ of confusion, immobility and incontinence.10
General practitioners (GPs) have principle responsibility for the medical care of care home residents and it has a major impact on their workload.11 Less than 40% of GPs have had specialist training in the health and social care needs of older people.12 NHS clinical input, as well as funding, should be appropriate to the level of need. However, government policies on healthcare provision have not been clear. As a result, the local arrangements for allocating clinical input are highly variable.5
Geriatricians are required to have training in continuing care for the Certificate of Specialist Training, however they have been increasingly less involved with continuing care over the last 20 years, even for the most complex patients, despite the fact that geriatric departmental involvement has been shown to improve patient outcomes.13–15 Concerns about this situation have grown in view of the prediction of increasing numbers of care home residents as a result of demographic change.16
In 2000, the BGS collaborated with the RCP and the RCN to produce comprehensive inter-professional guidance which recommended inter alia the participation of physicians with geriatric medicine training in all complex assessments, the development of disease management programmes, clinical governance and training of staff in care homes.4 This has been augmented by subsequent position statements.5
In this study, the opinions of geriatricians and primary care trusts (PCTs), and the services they provide, were investigated to see if they corresponded with this guidance on involvement with assessment prior to admission and ongoing healthcare provision.
Methods
Complementary surveys for PCTs and geriatric medicine departments (GDs) were designed to test concordance with the recommendations made in the RCP/RCN/BGS report. Some questions were factual, while others sought opinions of respondents, expressed on a Likert scale. The final survey instrument was produced after piloting among geriatricians in the south east of England to assess feasibility, wording and comprehension.
The questionnaires were distributed in summer/autumn 2006 to:
the lead clinician in each GD in England
the lead nurse in each PCT in England.
Recipients were asked to pass the survey on to the professional in their organisation with the most local knowledge about care homes. We suggested that this would likely be:
the GD's consultant lead for continuing care
the PCT senior nurse responsible for overseeing the process of assessments to determine the Registered Nursing Care Contribution (RNCC), for which each PCT was responsible for its local residents.
The responses were made anonymously but were numbered in a manner blinded to the investigator to allow a second mailing to non-respondents two months later. Data was analysed on SPSS software.
Results
Responses were received from 109 of the 167 (65%) GDs in England and 141 of the 303 (47%) PCTs. The findings relating to the involvement of GDs using the data from both surveys are presented below. Results are grouped under topics highlighted by the RCP report.
Involvement of geriatric departments in the care of older people in care homes
Geriatric medicine needs to be re-engaged at a number of levels, not least to provide specialist opinion and advice to GPs in the management of care home residents … with defined sessional time related to workload.4
Only 17 (15.7%) GDs specifically allocated sessions to care home work. This accounted for just 1% of the total consultant sessions available in the departments. An additional six (5.6%) gave support to care homes in ‘good will time’. Of the departments with allocated time, more were involved with care homes with nursing (n=15) than residential care homes (n=7). These figures were reflected in the PCT survey, with few (18.4%) PCTs reporting that they funded geriatricians’ involvement in care homes. In contrast 52% (n=74) of PCTs either required geriatricians’ involvement in the admissions assessment process (19.8%, n=28) or in supporting ongoing care of care home residents (40.4%, n=57).
Figure 1 shows the opinions given by the GD respondents about the importance of geriatrician involvement in care homes. With current resources, few (2%) considered that their department's involvement was ‘too much’, while 73% favoured greater involvement. This increased to 85% if more resources were to be made available. The majority of PCT respondents considered the involvement of geriatricians in care homes as important (Fig 2).
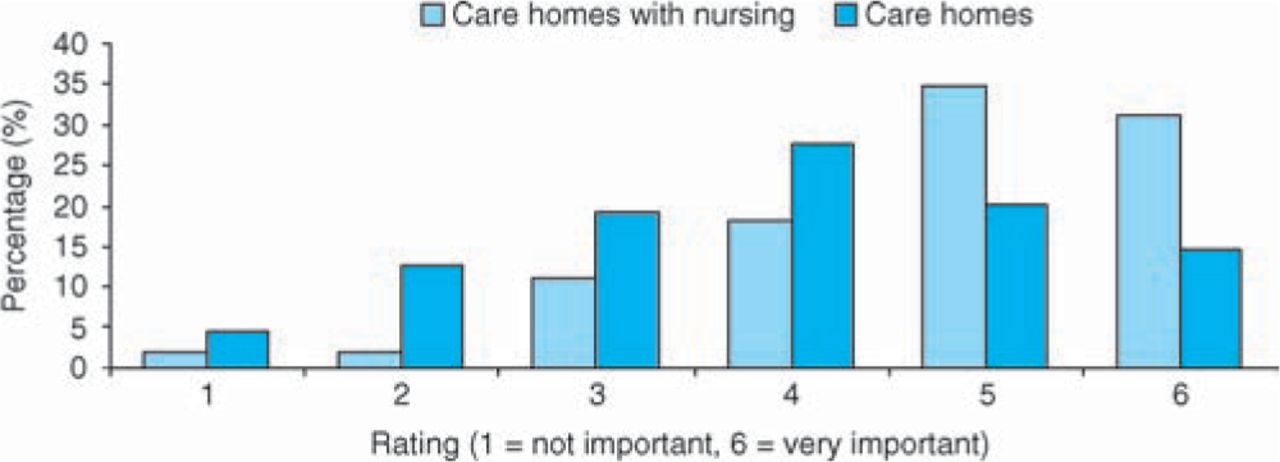
Geriatric medicine departments: how important is it that geriatricians are involved in care homes?

Primary care trusts: how important is it that geriatricians are involved in care homes?
Pre-admissions assessment
An Agreed Comprehensive Assessment Tool should be adopted that records diagnoses along with disabilities to enable commissioning, inform care planning and governance.4
Specialist geriatric and old age psychiatry departments could be strengthened by health and social care commissioners to undertake comprehensive assessment for placement.4
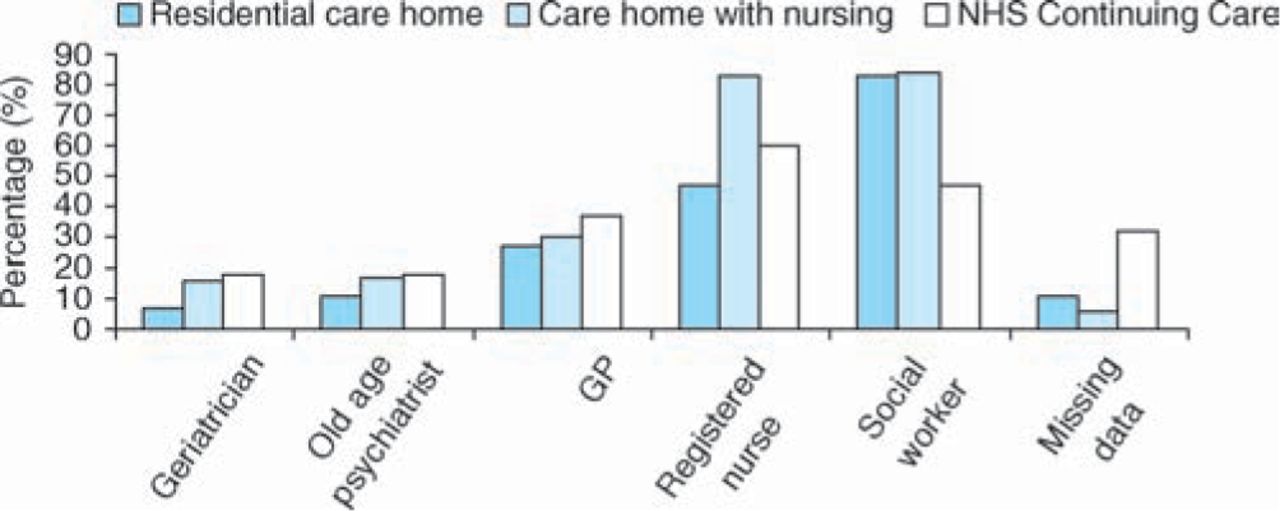
The PCT survey revealed that most (84%) had a standardised comprehensive assessment for persons being admitted into care homes with nursing. Figure 3 shows that the majority of medical and mental health assessments are completed by a social worker and/or nurse, with few PCTs having a mandatory requirement for the involvement of an old age physician (16%) or psychiatrist (17%). The questionnaire did not allow us to determine whether the professionals performing the assessments had received specific training.
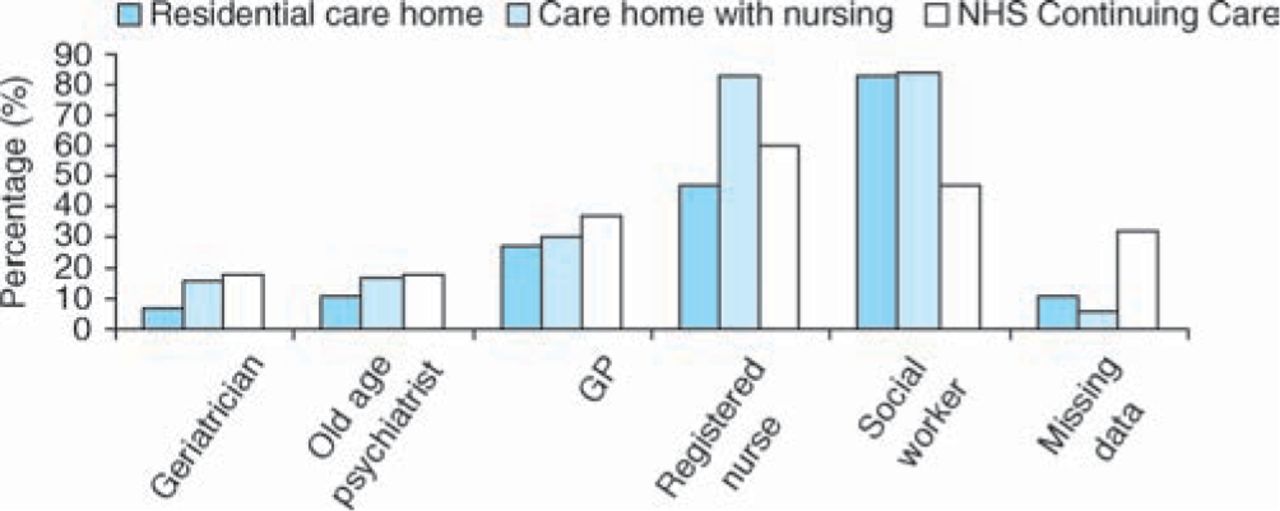
Primary care trust survey: who must assess a person before they are admitted to a care home? GP = general practitioner
Geriatricians were much more likely to be involved with admissions from hospital than admissions from home (Fig 4).17 Geriatricians assess more older people going to care homes with nursing than to residential care homes.
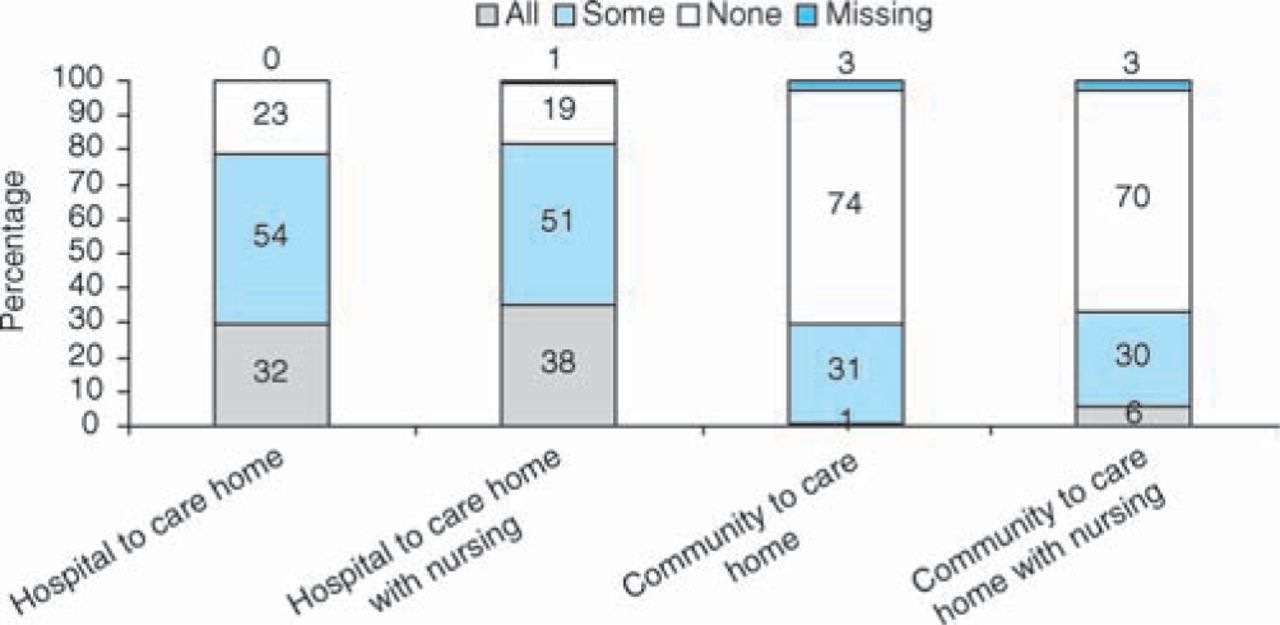
Geriatric medicine department survey: are geriatricians involved in the admission assessment to care homes in your area?
Of the surveyed departments 75% knew of a committee or ‘panel’ assessing patients’ needs on admission to a care home with nursing in their area (65.7% for residential care home patients), but few included representation from their department and only 10% included a consultant geriatrician.
Ongoing care for residents in care homes
Specialist geriatric and old age psychiatry departments could be strengthened by health and social care commissioners to undertake. interdisciplinary care planning and review.4
Only 24% (26/109) of GDs gave ongoing input to care homes, which was predominantly (19/26) performed by consultant geriatricians. The majority (56%) of those that did not provide ongoing care believed their involvement should be greater even within current resources, and this opinion rose to 89% if more resources were provided.
Integration of care
Integrating all the professions into an organisation designed to address the care home population needs is most likely to produce effective and efficient care.4
The organisation, application and governance of all the professionals allied to medicine may be enhanced through integration with other professionals and through institutional based care rather than individual contracting.4
Thirty-three departments (30%) reported participation in initiatives to support ongoing care in care homes. Another 20 (18%) had tried to secure funding for an initiative but had been unsuccessful. Sixteen of the 33 initiatives provided allocated time from consultant geriatricians.
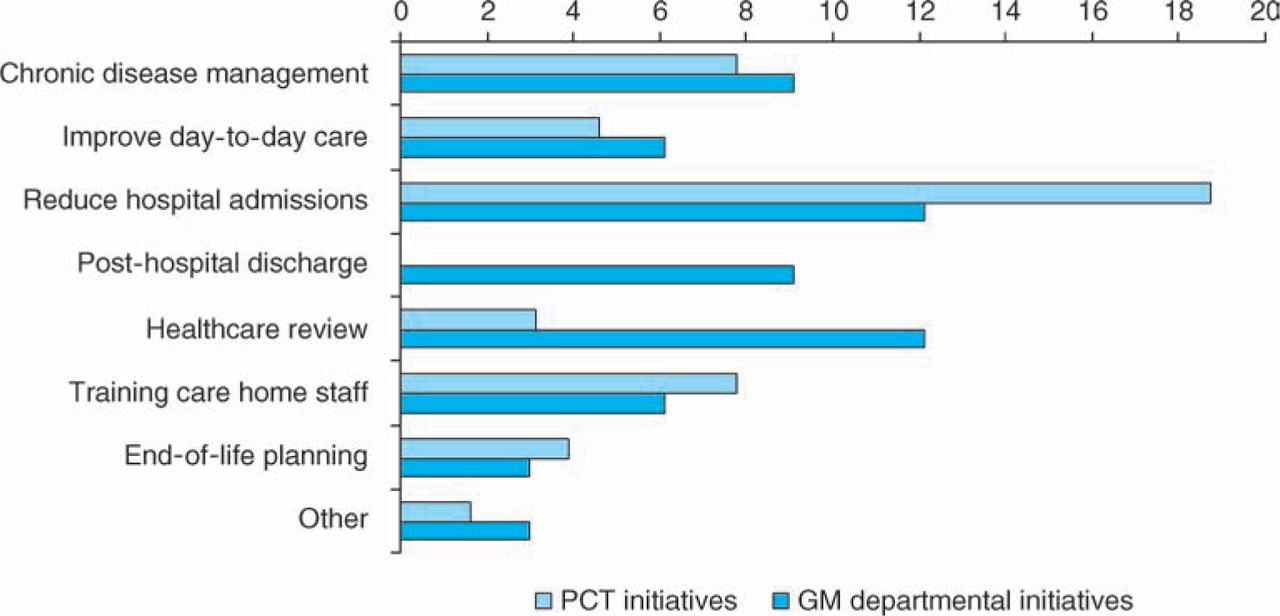
These initiatives predominantly supply support to care homes with nursing (30/33) rather than residential care homes (18/33) or NHS continuing care settings (7/33). Figure 5 shows the stated aims of the initiatives for each group. A surprisingly high number (45%) of GDs reported local PCT initiatives in which their department was not involved. Indeed, 90% (128) of PCTs reported such initiatives, most involving community matrons. Although the responses from GDs and PCTs were not necessarily co-terminous (and since they were anonymous we were not able to analyse this by region), the discrepancy between these figures suggests that there are community initiatives designed and delivered without the involvement or the knowledge of the local GD.
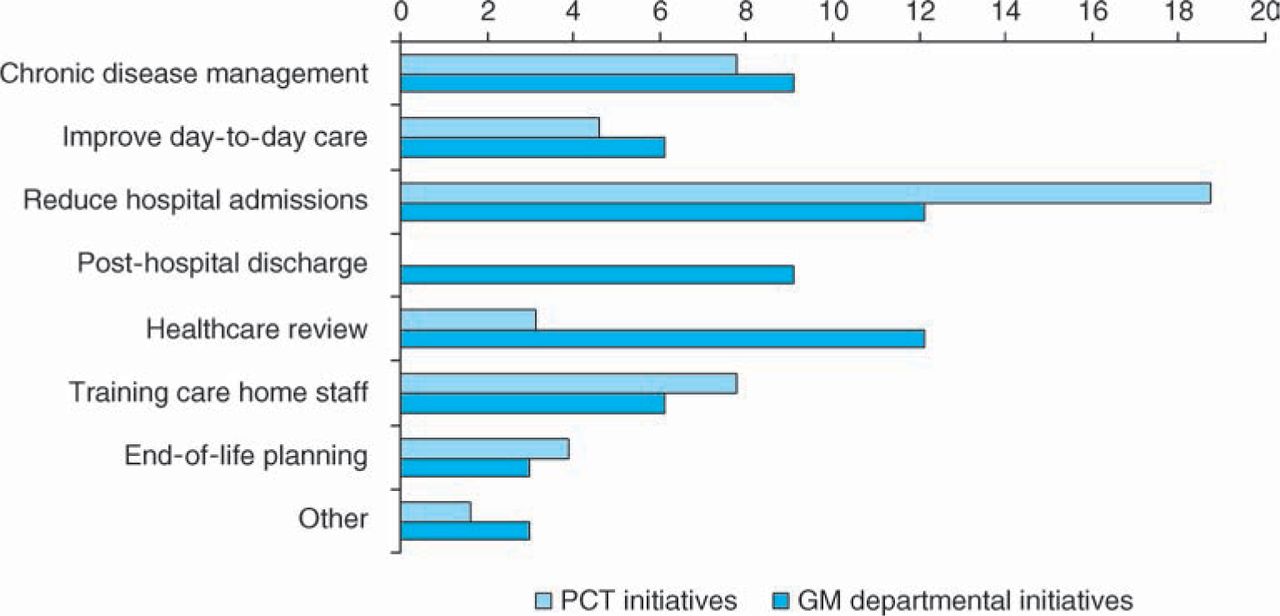
What were the primary aims of your initiative in care homes? GM = general medicine; PCT = primary care trust.
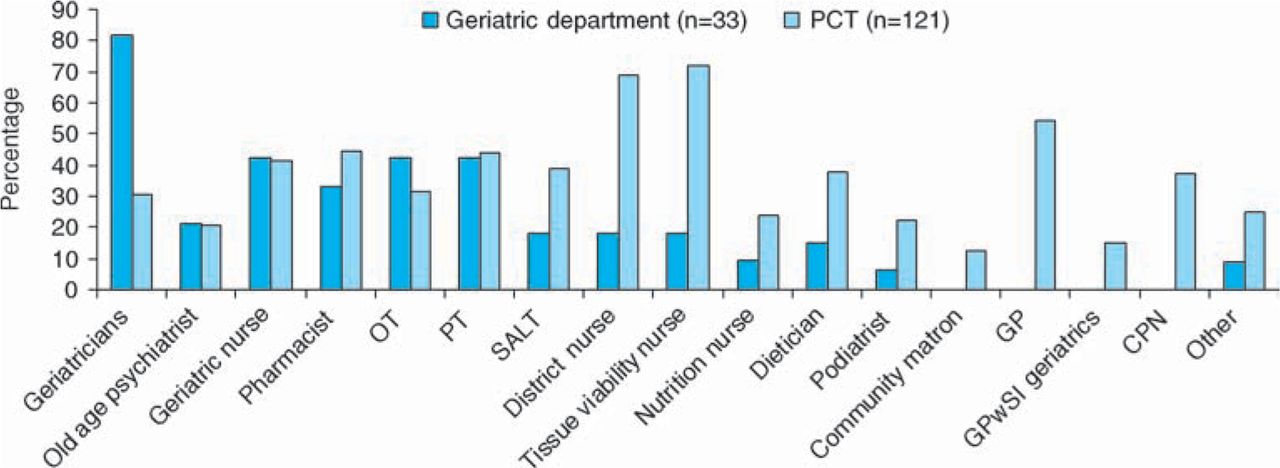
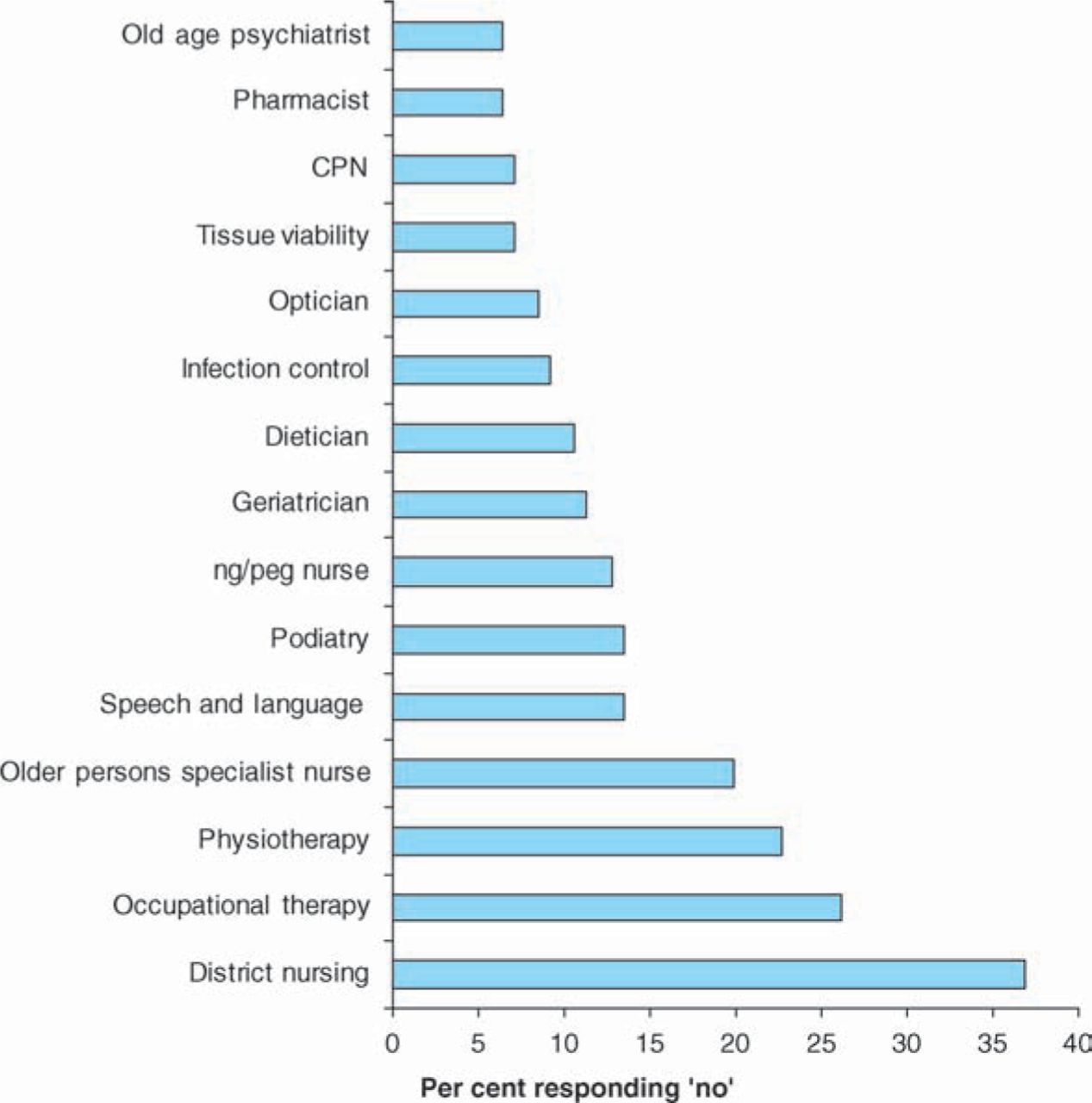
Figure 6 shows the disciplines involved in the initiatives described by GDs and PCTs. In total, 81% of PCT initiatives and 64% of GD initiatives involved four or more professionals. However, a large minority of PCTs reported that persons living in care homes had restricted access to various professionals in comparison to community dwelling persons – in particular to occupational and physical therapists (Fig 7).
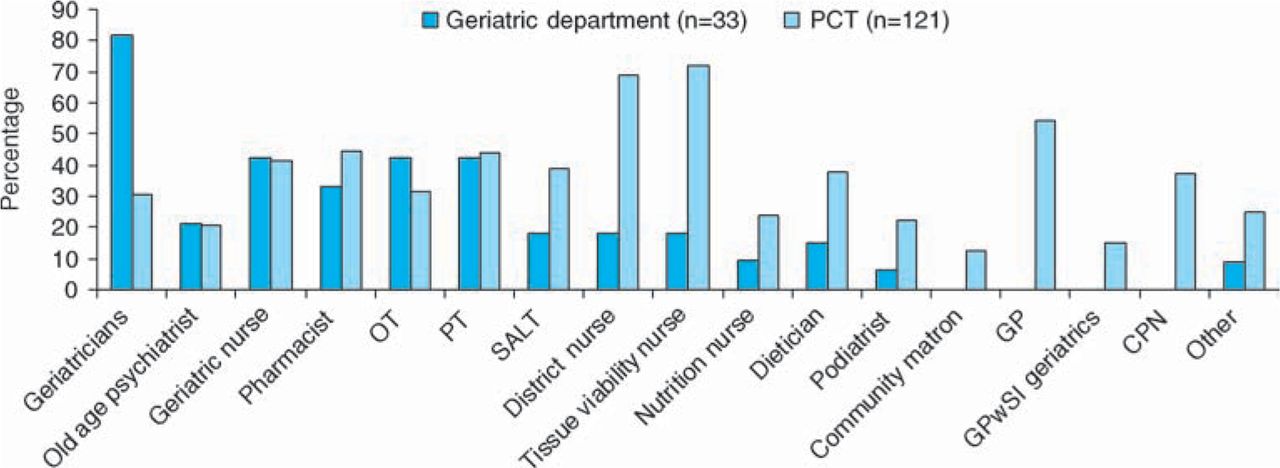
Which of these professionals are involved in your initiative to support care in care homes? CPN = community psychiatric nurse; GP = general practitioner; GPwSI = GP with special interests; OT = occupational therapist; PCT = primary care trust; PT = physiotherapist, SALT = speech and language therapist.
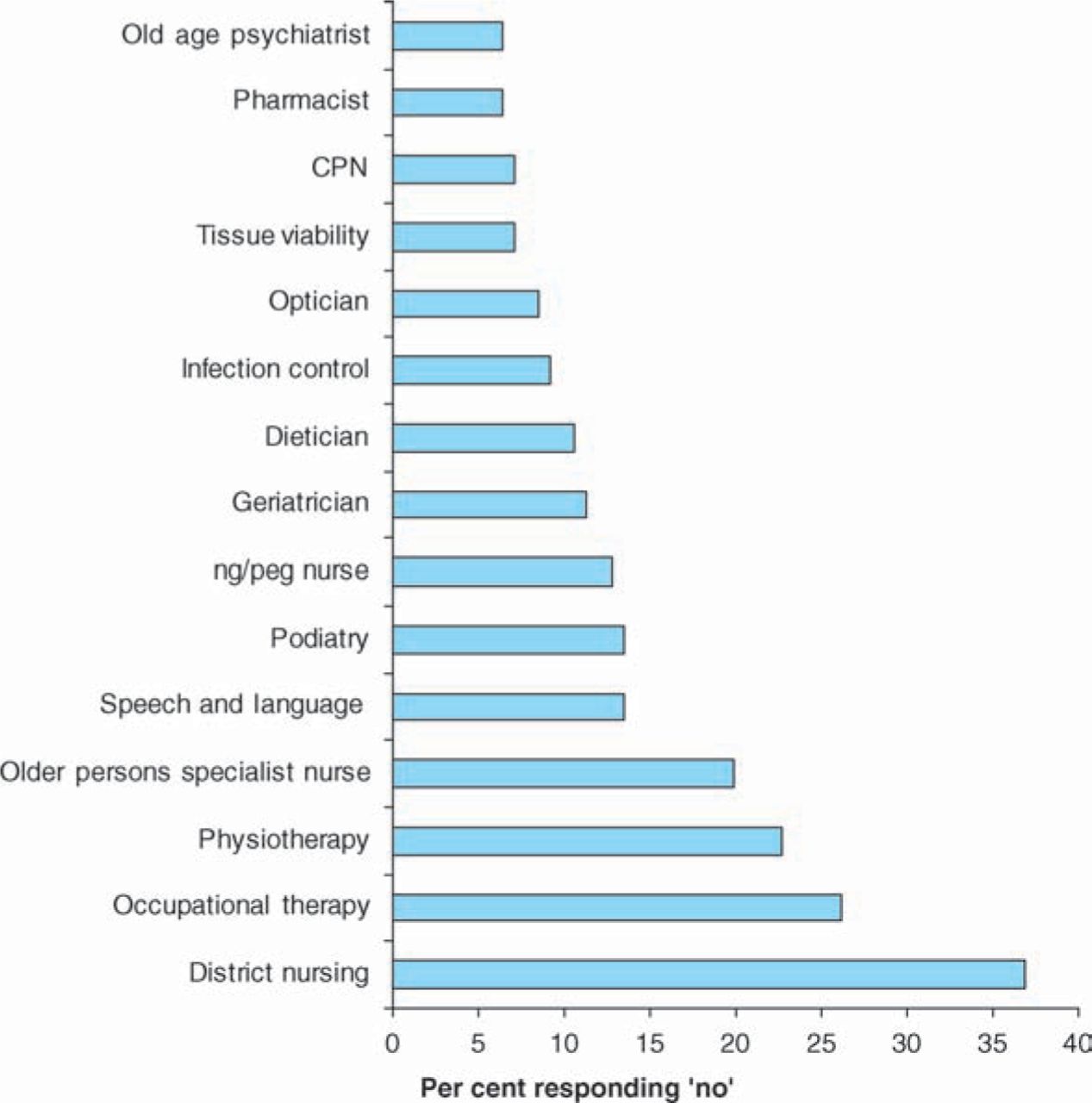
Do care home residents have equitable access to the following services? CPN = community psychiatric nurse, ng/peg nurse = nasogastric/percutaneous gastrostomy feeding nurse.
Despite the recognised need for specialist support for GPs and care home nurses, only 14% of GDs reported a regular forum by which GPs and nurses could discuss challenging patients, a low rate confirmed by PCTs (11%).
Discussion
The response rate of 65% means that this survey gives a reasonable indication of the opinions and involvement of GDs and geriatricians with care home residents in England. The result for PCTs (n=141/303, 45%) is less representative, and may reflect the fact that the PCTs merged during autumn 2006 to form 152. For both groups of respondents there is likely to be a significant selection bias in favour of those with greater interest or involvement with care homes. Thus the actual overall situation in England is unlikely to be ‘better’ than the picture painted by this survey. This survey reflects the opinions and knowledge of professionals in each institution with regard to care homes, rather than the institutions as a whole. PCT responses may reflect commissioning policy rather than clinical experience of the respondents.
These professionals reported considerable support for the recommendations made in the inter-professional guidance. Some localities had well developed, multidisciplinary, funded and resourced teams of professionals, using integrated working between primary and secondary care to meet specific patient-centred goals. This at least shows that this high standard is possible in England. Unfortunately the majority of localities did not report this kind of working. In particular, geriatric medicine has not systematically re-engaged in the care of elders in care homes and there is indication of lack of linkage between community care and hospital-based services for older people.
Although over half of PCTs said they had geriatrician involvement either in admission assessment or ongoing care, only one third of these had funded the necessary sessions from local services and overall there are very few dedicated job plan sessions for this work. GDs considered that additional funding would enable this work to be given greater priority. The lesson for PCTs seems clear: commission the service that you want.
Local requirements for involvement of some of the necessary specialists, particularly geriatricians and old age psychiatrists, were very low, even for decisions about NHS-funded continuing healthcare. This is not consistent with DH guidance in force at the time of the survey and strengthened subsequently.3 Specialist involvement in admission assessment was particularly low for those entering care homes from the community. It is these people who are most likely to miss out on treatment for reversible aspects of their disability. Our survey did not ask specifically about the involvement of palliative care teams, but it is likely that these form an important specialist input to this group.
Do these residents need specialist care from geriatricians?
There is evidence showing the benefit of specialist preadmission assessment in identifying unmet need, and averting admission to institutions.7,18,19 The ongoing care initiatives described in this survey placed a high priority on effective acute care and reducing hospital admissions from care homes, in line with the National Service Framework for Older People (2001). Clearly, for this frail group, giving timely, high quality and multispecialty care in the care home setting could benefit patients and reduce the burden on acute settings. Until recently there were few studies of effectiveness of the involvement of geriatricians in ongoing care. A recent study of geriatrician-led multidisciplinary intervention in 100 older adults in residential care showed trends towards decreasing mortality and hospitalisation, a finding which needs to be supported by larger studies which may reach significance.20
Over the last decade there has been increasing interest in models of geriatric nurse specialist input to enhance ongoing care in care homes and reduce hospitalisations, such as the Evercare model.21 It is worth noting that such evidence-based models had geriatric physician support, and the validity of applying them without multidisciplinary backup has not been tested.
Despite the fact that bodies such as the RCP, BGS and RCN support enhanced input from specialist physicians, the relative lack of empirical work to support their involvement in ongoing care is a major barrier to commissioning services.
What are the reasons for limited involvement of specialists?
The lack of specific commissioning for specialists in care homes may indicate this is a low priority for PCTs. Alternatively, PCTs may be unclear what is needed, or how to commission it. Of the GDs surveyed, 18% reported provider-initiated bids for services to support care home residents had been turned down by commissioners.
There are historical factors at play here. In previous decades, the specialty of geriatric medicine was focused on persons living in long-stay wards but who might now be resident in care homes.22 During the 1980s, the widespread closure of these wards combined with massive expansion of the independent care home sector separated geriatricians from this category of patients. These changes happened as a result of changes in social policy, not because of a re-assessment of the clinical needs of these patients or the skills needed to meet them.
An additional factor limiting care home involvement lies in the relationship between geriatricians and other medical specialties. Geriatricians are the largest specialty of physicians in England and are heavily involved in acute general medicine, as other specialties have become more specialised and interventional. Fourteen of the 109 GD respondents felt driven to write spontaneously that their involvement in care home work was precluded by their acute medicine commitments: ‘Our role as specialist physicians for older people with complex needs is at odds with our ‘acute’ role in acute assessment units where we are often deployed’. Care home residents may have lost out in this restructuring of acute medicine. With the advent of acute physicians there is now the potential to redress this balance.
Finally, in terms of policy, the government has indicated its intention to address standards in this sector, as demonstrated by the Commission for Social Care Inspection. However, this has been done in the current social policy climate of arms-length devolvement. Clinical leadership, through direct engagement of caring professionals and with residents and carers, might be more likely to result in patient-centred improvements in care.
Where do we go from here?
Several steps for the future are outlined below:
share experience from existing service models
share information to support successful bids for PCT or interagency funding
encourage funding bodies such as the National Institute for Health Research to support health service research in this area
develop clinical and academic partnerships to develop an evidence base
collaborate with other clinical professionals, such as palliative care teams, old age psychiatrists and community matrons, as well as service managers to achieve these aims.
Improving care for elders in care homes is both an academic and a clinical challenge for the RCP and other specialist clinical societies, requiring research on the most effective ways to support the health of our elders and leadership in standard setting and guiding the delivery of specialist care as this population grows. It is through joint health and social care commitment that progress can be sustained. Thus, there is also a challenge for service leaders and policy makers to improve the access to care for this vulnerable group of older people.
Acknowledgement
This survey was supported by a specialist registrar grant from the British Geriatrics Society.
- © 2009 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.