
Abstract
Endoscopic ultrasound (EUS) is an increasingly available diagnostic and therapeutic tool used within the UK. It has wide applications both in the gastrointestinal tract and mediastinum with its current main uses being in the staging of luminal malignancies and assessment of pancreatic and subepithelial lesions. The emergence of linear EUS has opened up new therapeutic avenues with fine needle aspiration, trucut biopsies, coeliac plexus blocks and transmural pseudocyst drainage all now possible. Future developments include localised brachytherapy/chemotherapy and alcohol ablation of unresectable pancreatic malignancies and EUS-guided endoscopic surgery.
Introduction
Endoscopic ultrasound (EUS) was developed in the 1980s but was rarely used within most of the UK. The advent of therapeutic EUS using linear echoendoscopes a decade later, in particular the ability to sample lymph nodes and suspected malignancies by fine needle aspiration (FNA), led to its wider uptake although service provision still remains centralised in most areas. Currently the staging of oesophageal and oesophagogastric junctional cancers in patients potentially fit for curative surgery remains the most common indication for EUS, although the increasing use of cross-sectional imaging is resulting in incidental pancreatic lesions often requiring EUS assessment. This paper aims to detail the widening applications of EUS both as a diagnostic modality and increasing therapeutic intervention so those without current access are aware of the relevant referral indications and its increasing contribution to patient care.
What is endoscopic ultrasound?
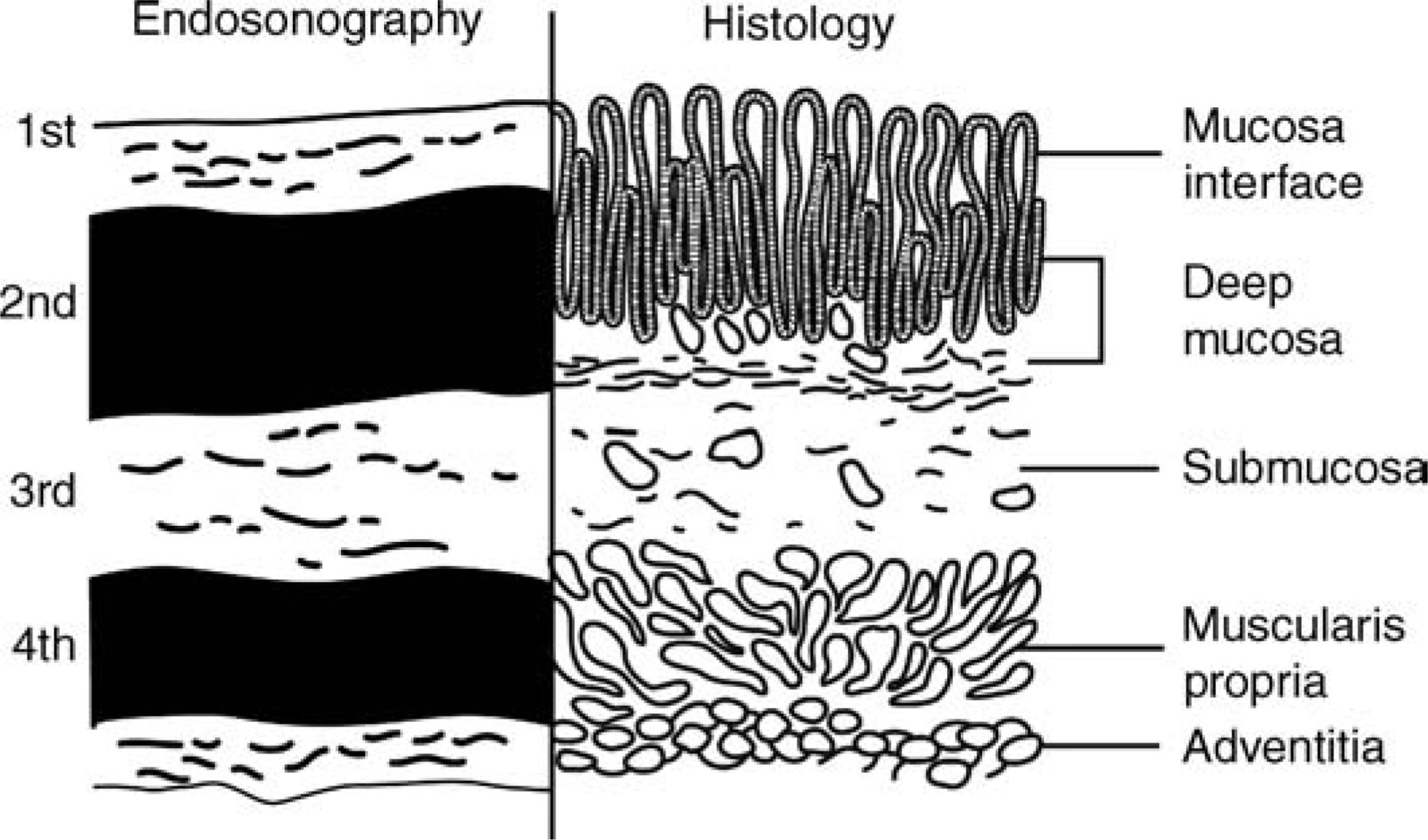
Endoscopic ultrasound combines the two modalities of endoscopic visualisation with high frequency ultrasound to enable imaging of the wall of the gastrointestinal (GI) tract and beyond into the organs and vessels in proximity. The ability to define each of the five wall layers of the GI tract corresponding with its histological counterpart and also detect localised lymph nodes forms the basis for most EUS procedures (Fig 1).
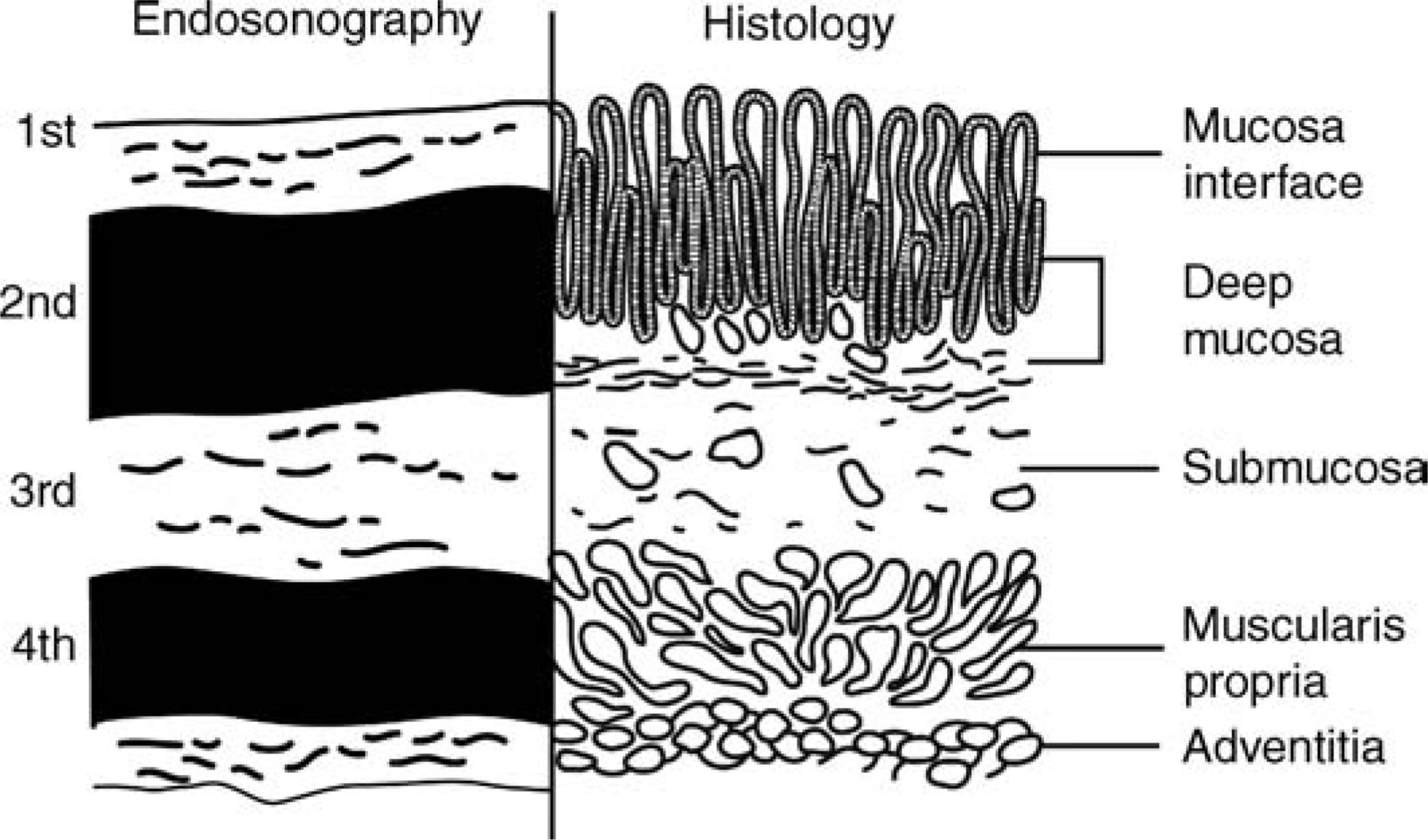
Wall layers at endoscopic ultrasound and corresponding histology.
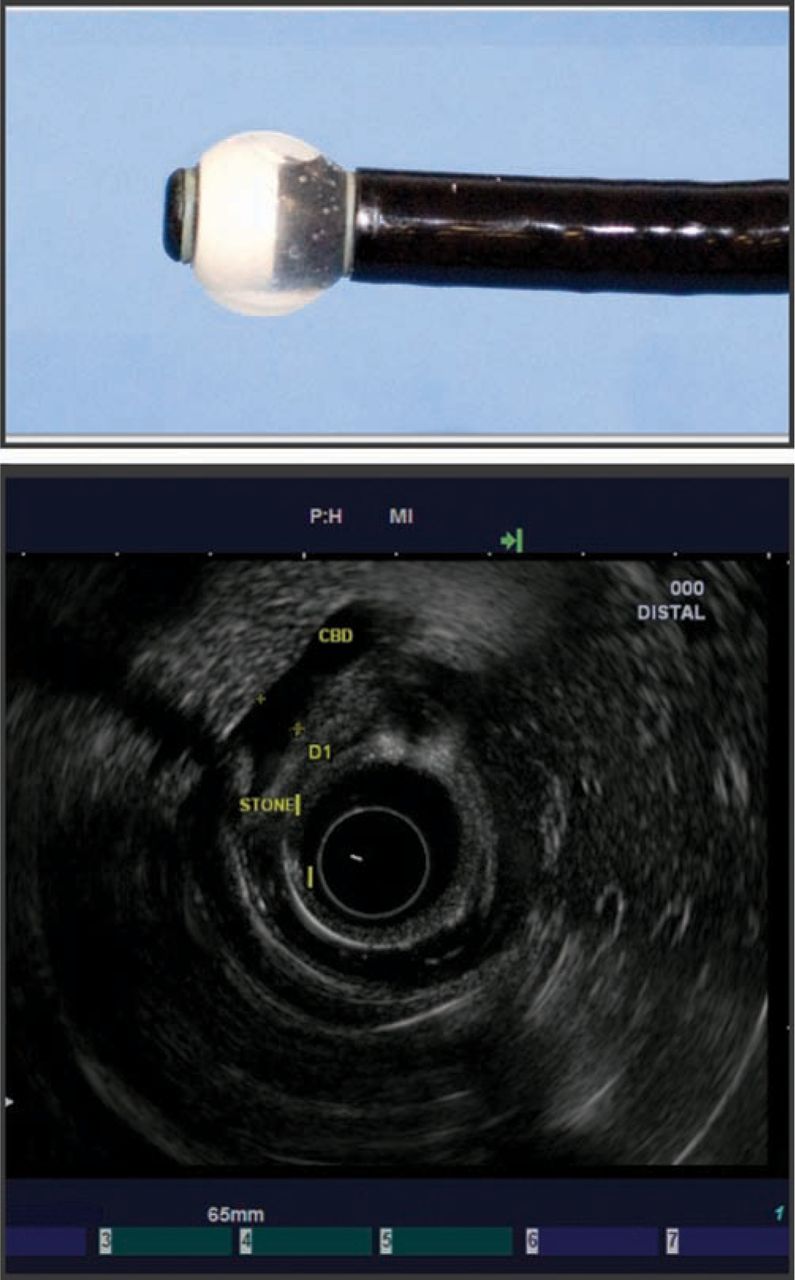
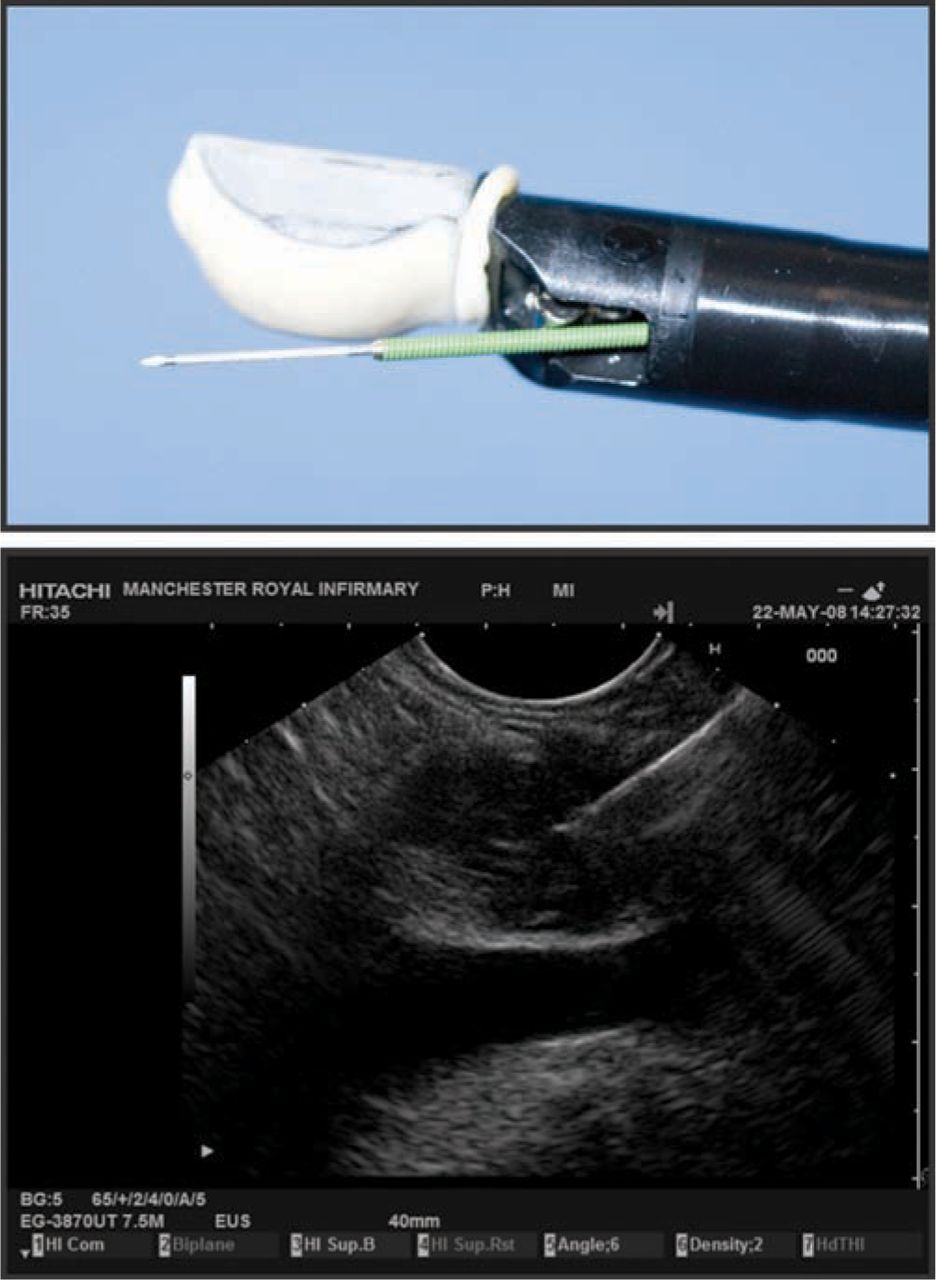
There are two types of commonly used echoendoscopes each with differing characteristics. Radial EUS was the first to be developed and provides a 360-degree view in a plane perpendicular to that of the scope, similar to a computed tomography (CT) image (Fig 2). Linear EUS provides a localised oblique image parallel to the scope and enables therapeutic intervention under ultrasound (Fig 3). High frequency EUS mini-probes are also available which can be passed down a standard biopsy channel of an endoscope in cases where strictures cannot be passed using a standard EUS scope.
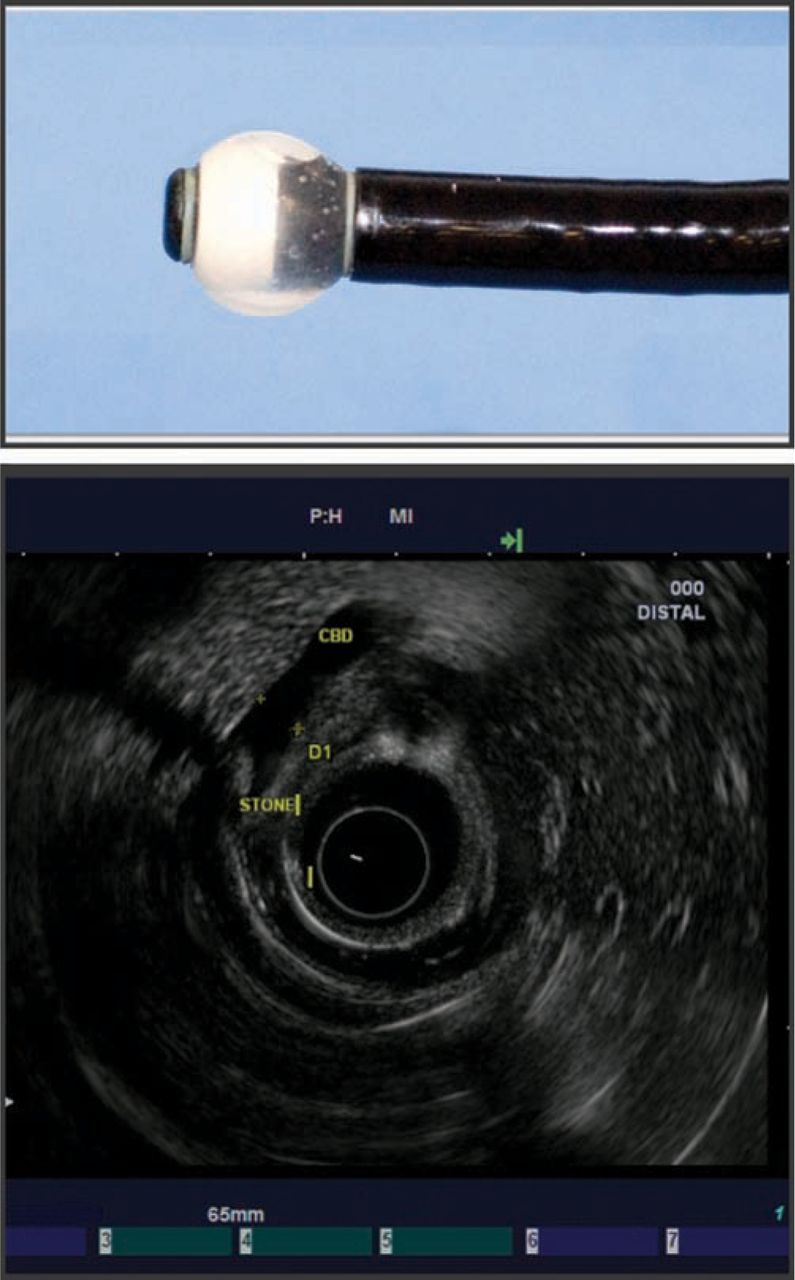
Radial endoscopic ultrasound (EUS) scope with EUS of bile duct stone.
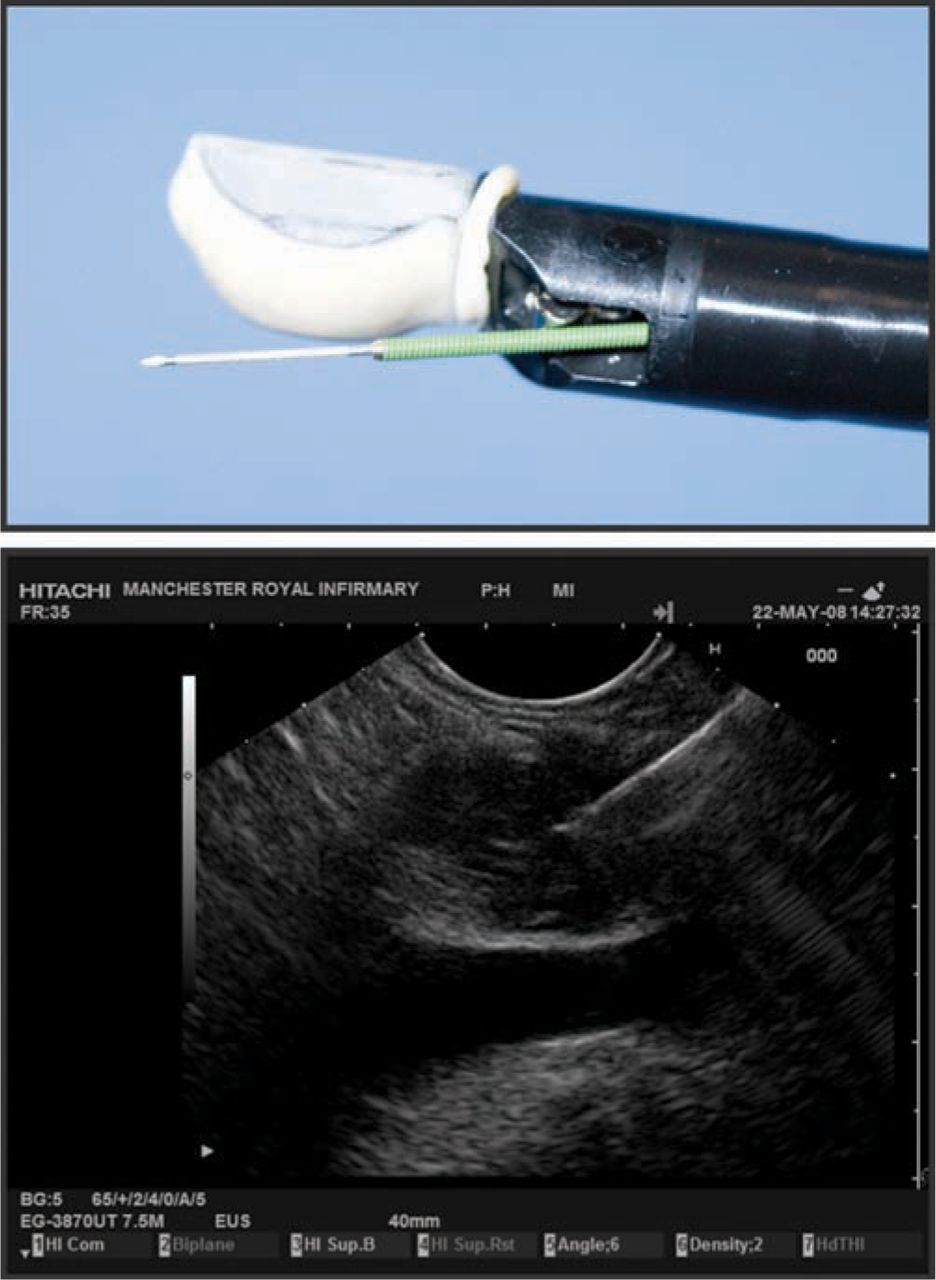
Linear endoscopic ultrasound scope with fine needle aspiration (FNA) and pancreatic mass FNA.
Indications for endoscopic ultrasound
The indications for EUS can be divided into several categories:
staging of GI malignancies
evaluating pancreaticobiliary disease
evaluating subepithelial abnormalities
evaluating extraluminal abnormalities
staging of lung cancer
therapeutic EUS.
Staging of gastrointestinal cancers
Accurate staging of upper GI malignancy is vital for appropriate treatment selection for the patient. Because of its ability to delineate the different layers of the GI tract wall, EUS has now become an integral component in classifying GI cancers by the widely accepted TNM classification.
Oesophageal cancer
In oesophageal cancer, EUS has been proven to be superior to CT scanning for accurate local staging.1 EUS is more accurate at evaluating the coeliac axis lymph nodes and is usually performed when the CT staging has not shown distant metastasis. This helps in appropriate patient selection for neoadjuvant chemoradiation therapy. Patients with very early oesophageal cancer may also benefit from less invasive procedures such as endoscopic mucosal resection. Meta-analysis comparing CT and EUS in oesophageal cancer have shown T staging accuracy of 50–80% and 85–90% respectively.2 The NHS health technology assessment systematic review of endoscopic ultrasound in gastro-oesophageal cancer confirms the high accuracy of EUS for T and N staging of oesophageal cancer.3
Gastric cancer
The accuracy of EUS in staging gastric cancer is not comparable to oesophageal cancer because of difficulty in differentiating between the subserosa and serosal layers. However, many studies have demonstrated superiority of EUS over conventional CT scanning in staging accuracy, ranging from 71% to 88% (T stage) and 77% to 80% (N stage).4,5 Both imaging modalities are complimentary in the staging process with EUS being particularly useful in staging localised early gastric cancer to assess for endoscopic resectability.
Pancreatic cancer
The high resolution images of EUS in visualising the pancreatic duct and parenchyma make it highly sensitive in the detection of small tumours, cysts and vascular invasion.6 EUS is superior to spiral CT, magnetic resonance imaging (MRI), or positron emission tomography (PET) in the detection of small pancreatic tumours with a staging sensitivity greater than 90%.6,7 It is also the most sensitive modality for detecting pancreatic neuroendocrine tumours and can distinguish structures as small as 2–3 mm.8
Pancreaticobiliary disease
Cystic lesions of the pancreas
With the increasing availability of CT scans there has been a steady rise in the number of incidental cystic lesions of the pancreas and although the majority of these lesions are small and benign up to 10% may represent malignant or premalignant neoplasms.9 Despite advances in CT and MRI, the ability to differentiate between benign and malignant cysts remains limited. EUS not only provides high resolution images but also has the added advantage of sampling the cyst content and any local lymph nodes. EUS-FNA with cytology in such cystic lesions can improve the diagnostic accuracy.10
Chronic pancreatitis
Endoscopic ultrasound is a very sensitive imaging modality for the detection of structural changes of chronic pancreatitis which may be absent on transabdominal ultrasound, CT, MRI or endoscopic retrograde cholangiopancreatography (ERCP).11 Care must be taken, however, not to over diagnose normal age-related pancreatic changes as early chronic pancreatitis. Often the most difficult diagnostic interpretation is distinguishing chronic focal pancreatitis from a hypoechoic pancreatic mass in patients with chronic pancreatitis. In this situation a positive EUS-FNA is very helpful but the low sensitivity means that surgery is often required when EUS-FNA is negative for malignancy.
Choledocholithiasis
In patients with suspected biliary stone disease, EUS has a sensitivity of greater than 90% in detecting common bile duct stones. It is comparable to ERCP in diagnosing biliary stone disease, without the inherent risks of pancreatitis, but it lacks the therapeutic ability for stone removal. It is far superior to transabdominal ultrasound and controlled studies have shown EUS is comparable or superior to magnetic resonance choiangiopancreatography in the detection of biliary stone disease.12
Subepithelial lesions of the gastrointestinal tract
Endoscopic ultrasound has an important role in the evaluation of subepithelial lesions in the GI tract. It can characterise lesions by determining their size, margins, layer of origin and echo texture and can differentiate between extramural or intramural lesions. The most common upper GI subepithelial lesions are normal wall indentations caused by extramural organs such as the liver, spleen, gall bladder or splenic vein.13 Benign subepithelial lesions identified by EUS include lipomas, simple cysts, congenital duplication cysts, ectopic pancreatic tissue and varices. Malignant subepithelial lesions diagnosed by EUS include metastases, lymphoma and carcinoid tumours. Gastrointestinal stromal tumours (GISTS) are increasingly recognised with the majority of these lesions being benign but some have malignant potential depending on size, mitotic index and location. EUS trucut biopsy can enable differentiation between malignant and benign GISTs.14
Mediastinal lymphadenopathy
Endoscopic ultrasound can readily identify lymph nodes in the aortopulmonary, subcarinal, paratracheal and para-oesophageal regions. EUS-FNA of mediastinal nodes improves the diagnostic accuracy in determining the malignant feature and hence avoiding mediastinoscopy or thoracotomy. EUS-FNA has been shown to yield diagnosis when CT, PET, bronchoscopy and pleurocenteses have been negative or inconclusive. The sensitivity of EUS-FNA for detecting malignancy in mediastinal lymph nodes is in the region of 88–96%15 and it is also possible to differentiate tuberculosis, sarcoidosis and lymphoma following EUS-FNA and trucut biopsy without the need for invasive mediastinoscopy. The recent development of tissue elastography to determine malignant lymph node potential by analysing lymph node tissue density is also possible using EUS which may help refine future EUS-FNA to the most suspicious node.16
Endoscopic ultrasound in lung cancer staging
The staging of lung cancer is dependent on transbronchial biopsy, CT-guided FNA, mediastinoscopy with biopsy or thoracoscopy. EUS-FNA has been proven to be an accurate and safe procedure for lymph node staging in patients with documented lung cancer.17 EUS also has the ability to identify mediastinal nodes missed on staging CT and in non-small cell lung cancer EUS-FNA has been shown to be accurate and cost effective for nodal staging in patients with documented posterior mediastinal lymphadenopathy, with a sensitivity of 83% and the specificity of 97%.18,19 Recently the development of endobronchial ultrasound (EBUS) has been shown to be complimentary to EUS allowing near-complete minimally invasive mediastinal staging in patients with suspected lung cancer with a diagnostic accuracy of 90–100%.20
Therapeutic endoscopic ultrasound
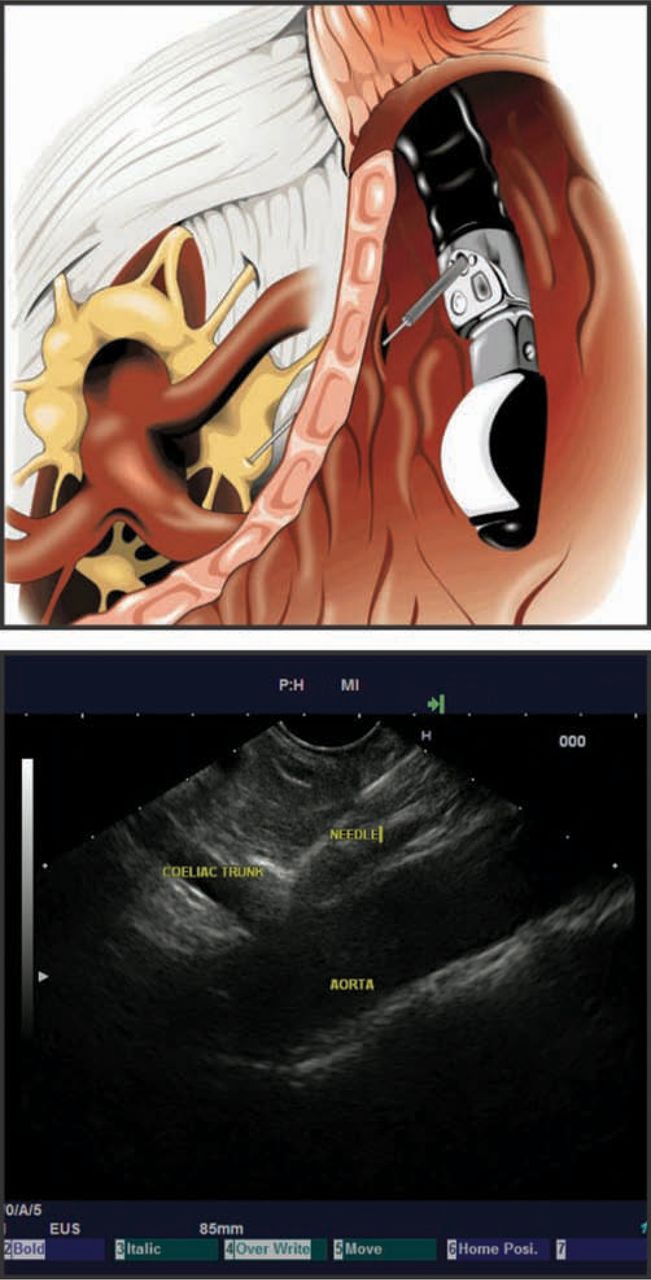
The initial development of EUS-FNA has progressed to provide new and novel therapeutic indications for EUS. Coeliac plexus blocks and neurolysis using EUS-guided injection of steroids or alcohol into the coeliac plexus, and more recently directly into the celiac ganglia, is a safe and effective method for pain control in pancreatic cancer and to a lesser extent in chronic pancreatitis (Fig 4). 21,22
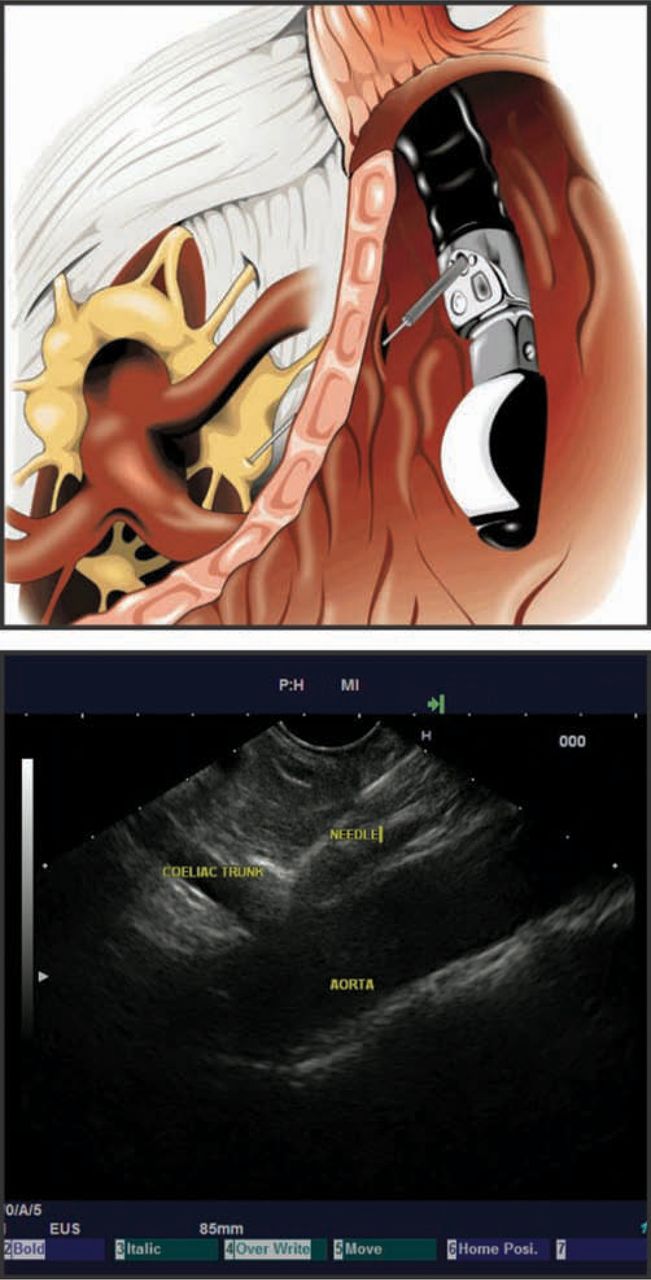
Endoscopic ultrasound coeliac ganglia neurolysis. Reproduced with permission of the original author.23
Drainage of symptomatic pseudocysts previously has been done blind via a direct endoscopic approach or required surgery. EUS cystogastrostomy allows characterisation of the pseudocyst, direct puncture into the cyst under EUS visualisation (thereby avoiding any vessels) and stent placement in one procedure while having a shorter patient stay than surgery. This should be the treatment of choice for symptomatic uncomplicated pseudocysts where available.24 EUS can also be utilised to access the biliary system when ERCP has failed by puncture of the common bile duct with a wire under EUS guidance and can detect and drain ascites not apparent on CT.25,26
Experimental applications of EUS undergoing current study include local delivery of brachytherapy or chemotherapy in advanced pancreatic cancer,27 alcohol ablation of adrenal metastases28 or pancreatic neuroendocrine tumours29 and EUS-guided submucosal implantation of radiopaque markers prior to radiotherapy.30 The rapid development of natural orifice transluminal endoscopic surgery is now blurring the boundaries between endoscopy and surgery with EUS playing a key role in its future.31
Summary
Although initially slow to be accepted within the UK, EUS has now an established role in many arenas. It is a safe and cost effective procedure which has a significant impact on the management of patients with oesophageal and oesophagogastric junctional cancer in accurately staging the disease. It is also the most sensitive method of detecting pancreatic malignancies, for determining the nature of subepithelial lesions and has a complimentary role in the staging of non-small cell lung cancer. Its therapeutic potential continues to increase as new indications are found and the procedure gradually becomes more available across the UK.
- © 2009 Royal College of Physicians
References








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- What is endoscopic ultrasound?
- Indications for endoscopic ultrasound
- Staging of gastrointestinal cancers
- Pancreaticobiliary disease
- Subepithelial lesions of the gastrointestinal tract
- Mediastinal lymphadenopathy
- Endoscopic ultrasound in lung cancer staging
- Therapeutic endoscopic ultrasound
- Summary
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.