
Introduction
Osteoporotic fractures are a major cause of morbidity and mortality in the elderly population. One woman in two and one man in five over the age of 50 years will sustain a fracture during their remaining lifetime, resulting in an annual cost to the health services in the UK of around £2 billion. In recent years there have been major advances in the prediction of fracture risk, enabling more accurate targeting of treatment. Furthermore, a range of therapeutic options with proven anti-fracture efficacy is now available. In spite of these advances, however, management of osteoporosis remains suboptimal and only around one-third of patients presenting with a fragility fracture receive appropriate diagnostic assessment and therapeutic intervention.
Diagnosis of osteoporosis and assessment of fracture risk
In 1994 a World Health Organization (WHO) study group produced an operational classification of osteoporosis, based on bone mineral density (BMD) measurements as assessed by dual energy X-ray absorptiometry (DXA).1 Osteoporosis was defined as a BMD T-score of ≤–2.5, the T-score being the number of standard deviations above or below the mean value for normal young women. Osteopenia was defined as a T-score between −1 and −2.5, while severe or established osteoporosis was defined as a T-score ≤–2.5 in the presence of one or more fragility fractures. These definitions were based on the known inverse relationship between BMD and fracture risk.
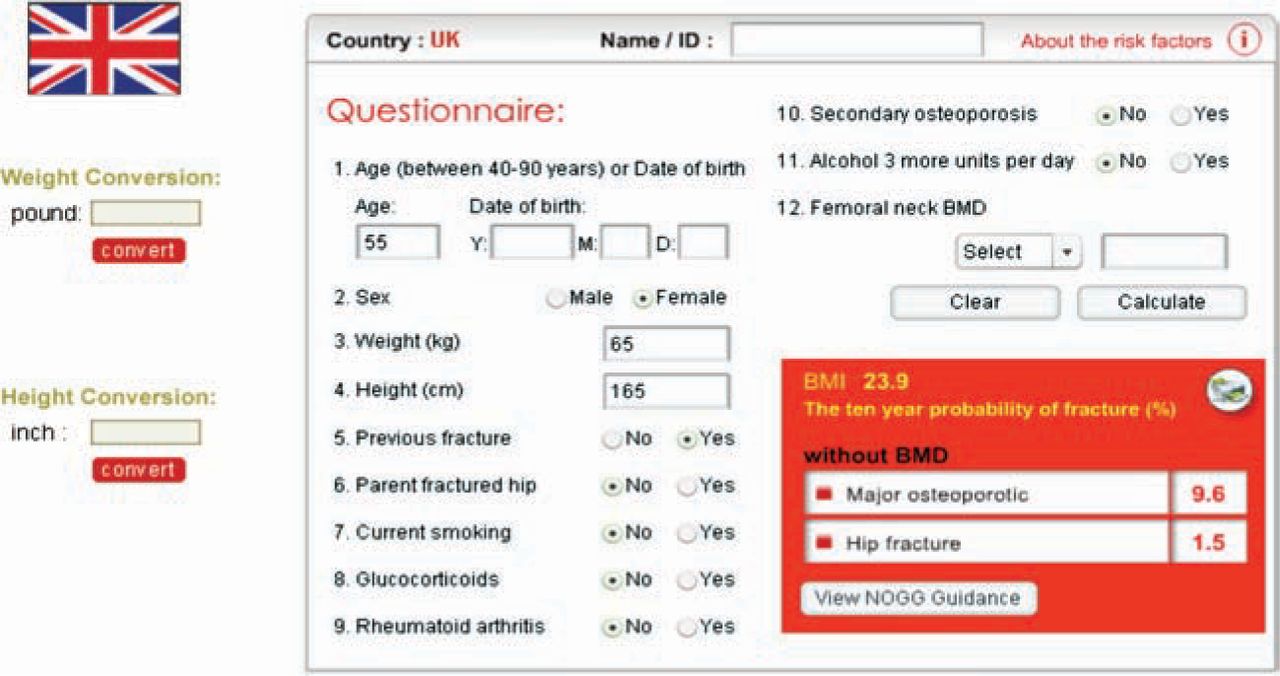
The use of BMD measurements to predict future fracture risk has a high specificity but a low sensitivity, and the majority of postmenopausal women presenting with a fragility fracture have a BMD T-score higher than −2.5. Recently the importance of clinical risk factors that affect fracture risk independently of BMD has been recognised.2 These are shown in Table 1 and are used in the WHO-supported FRAX® risk algorithm, with or without femoral neck BMD.3 FRAX® expresses fracture risk as the 10-year probability of hip fracture and of major osteoporotic fracture (hip, wrist, spine or humerus), from which intervention thresholds can be derived. Country-specific versions of FRAX® are available for a number of countries, including the UK (Fig 1; www.shef.ac.uk/FRAX).

The World Health Organization fracture risk assessment tool (FRAX®). Data have been entered for a 55-year-old woman with a previous fracture. The 10-year probability of sustaining a major osteoporotic fracture is 9.6% and of a hip fracture 1.5%. Image used with permission of the WHO Collaborating Centre for Metabolic Bone Diseases, University of Sheffield. FRAX® is registered to Professor JA Kanis, University of Sheffield.
Risk factors for osteoporosis.
It should be noted that FRAX® has some limitations. It is designed only for postmenopausal women and men over the age of 40 who have not previously received bone protective therapy. It uses only ‘yes’ or ‘no’ responses, and so does not take account of dose-responses for several risk factors including previous fracture, glucocorticoid therapy and smoking. The weighting given to any previous fragility fracture is the same and prior clinical vertebral fractures, which carry a higher risk than other previous fractures, are not considered separately. Falls are not included in the algorithm. For all these reasons, it is important to exercise clinical judgement when using FRAX® to assess fracture risk in clinical practice.
Case finding strategy
Population-based screening of postmenopausal women and older men cannot be justified on economic grounds and current guidelines recommend an opportunistic case finding strategy, in which postmenopausal women and older men with one or more clinical risk factor undergo fracture risk assessment using FRAX®. In individuals with very low or very high fracture probability, decisions about treatment can often be made on the basis of clinical risk factors without recourse to BMD but in those at intermediate risk, BMD is helpful in improving the estimation of fracture probability.
Intervention thresholds – who should be treated?
Intervention thresholds should be determined by clinical considerations, but should also be cost effective. The National Osteoporosis Guideline (NOG) uses thresholds that correspond to the risk of fracture in a woman with a prior fracture, irrespective of BMD.4 These intervention thresholds are cost effective and are consistent with the guidance previously produced by the Royal College of Physicians (RCP).5,6 The percentage of the population potentially eligible for treatment rises from 23% in 50–54 year old women to 46% in women aged 80–84 years.
When the UK version of FRAX® is used, the estimated 10-year fracture probability can be electronically transferred, using the NOG guidance button, to charts containing the intervention thresholds (Fig 2; www.shef.ac.uk/FRAX/NOGG). It should be emphasised that these thresholds serve as a reference upon which to make treatment decisions, but do not replace clinical judgement when dealing with individual patients.

Assessment and treatment thresholds in the absence of a bone mineral density (BMD) test (left) and with a BMD test to compute fracture probability (right) for men and women. The graph on the left is used when BMD measurements are not included in the FRAX® assessment; the orange area represents a range of intermediate risk in which BMD measurement is recommended, while for fracture probabilities in the green or red area, no further assessment is required. When BMD has been included in the FRAX® assessment, the graph on the right-hand side is used to determine whether fracture probability is above or below the intervention threshold. Reproduced with kind permission from Springer Science + Business Media.4
Pharmacological intervention
A number of treatments have been shown to reduce fracture risk in postmenopausal women.7 These include the bisphosphonates, raloxifene, strontium ranelate and parathyroid hormone peptides. All have been shown to reduce vertebral fractures but evidence for reduction in non-vertebral and hip fractures is not universal (Table 2).7 The reduction in vertebral fracture rate has generally been between 50–70% and since there have been no head-to-head studies with fracture as the primary outcome, direct comparison of efficacy between agents is not possible. The magnitude of reduction in non-vertebral fracture, where demonstrated, has generally been smaller and in the order of 15–25%. This is likely to reflect, at least in part, the importance of falls in the pathogenesis of these fractures but may also result from differences in the effects of the various treatments on cortical versus cancellous bone.
Spectrum of anti-fracture efficacy of approved pharmacological interventions for osteoporosis.
Because of their broad spectrum of anti-fracture efficacy alendronate, risedronate, zoledronate and strontium ranelate are generally regarded as front-line treatments in the majority of postmenopausal women. However, since generic versions of alendronate are now available, they represent the most cost-effective intervention and are therefore used as the first option in most cases.8
Bisphosphonates
Bisphosphonates are analogues of inorganic pyrophosphate and inhibit bone resorption. Nitrogen-containing bisphosphonates, which include alendronate, risedronate, ibandronate and zoledronate, act on the mevalonate pathway by inhibiting the action of farnesyl diphosphate and thus preventing the prenylation of proteins essential for normal osteoclast function. Alendronate and risedronate are available as once daily or once weekly oral formulations, ibandronate as once monthly oral or once every three months intravenous (iv) formulations and zoledronate as a once yearly iv formulation. All of these bisphosphonates are approved for treatment of postmenopausal osteoporosis; alendronate, risedronate and zoledronate are also approved for men with osteoporosis and for glucocorticoidinduced osteoporosis.
Oral bisphosphonates have to be taken after an overnight fast and 30–60 minutes before the first food or drink of the day or any other medicinal products. The tablet must be swallowed with a glass of plain water and the patient should remain in the standing or sitting position for 30–60 minutes. Compliance with this dosing regimen is essential to maximise intestinal absorption and prevent the occurrence of upper gastrointestinal side effects. Oral bisphosphonates are therefore not suitable for very frail patients or those with cognitive dysfunction and are contraindicated in the presence of significant oesophageal disease. The most common side effect of iv bisphosphonates is an acute phase reaction following the injection or infusion.9 This is sometimes severe, but is self-limiting and can be avoided or reduced in severity by taking paracetamol on the day of the infusion and the subsequent one to two days.
The optimal duration of treatment with bisphosphonates is unclear. Withdrawal of alendronate after treatment periods of up to seven years is followed by resumption of bone loss in the hip although the time course of this may vary between bisphosphonates.10 However, there are potential concerns that longterm suppression of bone turnover associated with treatment may eventually lead to adverse effects on bone strength. This remains largely a theoretical concern although there have been recent reports of atypical stress fractures in the femoral shaft or subtrochanteric region in patients on alendronate therapy; in some of these cases bone biopsies have been done and have shown severely suppressed bone turnover.11 However, it should be stressed that these fractures are extremely rare and easily outweighed overall by the beneficial effects of alendronate on fracture risk.
Another potential side effect of bisphosphonate therapy that has received much attention is osteonecrosis of the jaw. While it is likely that there is a causal association in patients with malignant disease receiving high doses of iv bisphosphonates, this remains unproven in patients receiving the much lower doses of bisphosphonates used for the treatment of osteoporosis. Since many of the cases reported have been associated with dental disease, invasive dental treatment should be completed before bisphosphonate therapy is started and where possible, avoided during treatment.12
Strontium ranelate
Strontium ranelate consists of two atoms of strontium linked to an organic acid, ranelic acid. Its mechanism of action is not fully understood but there is growing evidence that unlike other agents, its main effects are mediated through changes in bone material properties rather than alterations in bone remodelling. It is known that strontium can substitute for some of the calcium ions in hydroxyapatite and this may explain its effects on bone strength, rather than the weak effects that are seen on bone resorption and bone formation.13
Strontium ranelate is taken once daily as granules dissolved in water. It should be taken at least two hours after the last meal and is usually taken at bedtime. It does not cause upper gastrointestinal side effects and is therefore an alternative option in women who cannot tolerate oral bisphosphonates. It has a particularly strong evidence base in the very elderly, since unlike in most other clinical trials a large number of women over the age of 80 years were included in the phase III studies. Side effects include diarrhoea, nausea and headache; a small increase in the risk of venous thromboembolism was also seen in clinical trials.
Raloxifene
Raloxifene is a selective oestrogen receptor modulator and an inhibitor of bone resorption. It has been shown to reduce vertebral, but not non-vertebral, fractures and is taken orally as a single daily dose of 60 mg. Its use is associated with an increased risk of venous thromboembolism and it may cause or exacerbate vasomotor symptoms associated with the menopause. A small increase in the risk of stroke has also been reported. Its use is associated with a significant decrease in the risk of breast cancer.
Parathyroid hormone peptides
When administered intermittently, parathyroid hormone (PTH) peptides have anabolic skeletal effects. The resulting increase in bone formation is most marked in cancellous bone; in cortical bone, the effects may be site specific and transient decreases in BMD are often seen in the first year or so of treatment, possibly due to increased cortical porosity.14 PTH peptides are administered by once daily subcutaneous injection, in a dose or 20 μg daily for teriparatide and 100 μg daily for PTH (1–84) and the duration of treatment is limited to 18 and 24 months respectively. Because of their expense, the use of these drugs is restricted to individuals with severe osteoporosis in whom other treatments are not tolerated or appear to be ineffective.
Calcium and vitamin D
Calcium and vitamin D supplements should be prescribed as an adjunct to other treatments unless there is evidence of an adequate dietary calcium intake and normal vitamin D status. The recommended daily doses are 1–1.2 g and 800 IU respectively. Because of their high risk of vitamin D deficiency, supplementation at these levels is recommended in the elderly housebound population and those living in residential care homes or nursing homes.
Current guidance for the management of osteoporosis
The National Institute for Health and Clinical Excellence (NICE) has produced guidance for the primary and secondary prevention of osteoporotic fractures.15,16 This guidance is restricted to postmenopausal women with osteoporosis as defined by a BMD T-score of ≤–2.5, and does not include men with osteoporosis or individuals treated with glucocorticoids.
Several recently approved interventions, including ibandronate and zoledronate, are also not included in the guidance. The NOG was launched in October 2008 to address these deficits.17 It is endorsed by many scientific and professional organisations including the National Osteoporosis Society and the RCP.
Both NICE and NOG guidance include recommendations to treat elderly postmenopausal women with a fragility fracture and to use generic alendronate as a first-line option because of its high cost effectiveness. There is also agreement that BMD measurements may be useful in reaching treatment decisions in younger postmenopausal women with a fragility fracture. However, whereas NICE requires a T-score ≤–2.5 in most women for either primary or secondary prevention, NOG recognises the added contribution of independent clinical risk factors to fracture prediction and recommends the use of the WHO-supported fracture risk algorithm FRAX®. In addition, NICE guidance for second-line options demands different combinations of bone density and risk factors for different treatments; not only is this complex to operate in a primary care setting, but also raises difficult ethical issues, since some patients who meet the criteria for alendronate treatment but are unable to take it cannot have an alternative therapy until there is evidence of further disease progression. In contrast, NOG adopts a more pragmatic approach and does not require different criteria for second-line treatments in those who are unable to tolerate alendronate. In practice, therefore, a combination of the NICE and NOG guidance may provide the best way forward for the management of osteoporosis. An example of this approach is shown in Fig 3.

Possible algorithm for management of osteoporosis in postmenopausal women and men aged over 50 years. The dotted arrow indicates that although further risk assessment is often indicated in postmenopausal women aged ≤75 years and men aged over 50 years with previous fragility fracture, in some cases treatment without further assessment can be considered. BMD = bone mineral density; CRF = clinical risk factor.
Future developments and challenges
A number of agents are currently undergoing assessment for the treatment of osteoporosis. These include new selective oestrogen receptor modulators, calcium sensing receptor antagonists, cathepsin K inhibitors and inhibitors of sclerostin, a protein produced by osteocytes that inhibits bone formation. A human monoclonal antibody to receptor activator of NFkB ligand (RANKL), a cytokine that stimulates osteoclast development and activity, has been shown in phase III trials to reduce vertebral, non-vertebral and hip fractures and is currently being evaluated by the regulatory authorities.18 It is administered once every six months by subcutaneous injection.
An important challenge for the future is to improve adherence to therapy.19 Current data indicate that 50% or fewer of patients are taking their osteoporosis medication after one year, thus reducing the potential impact of therapy on fracture burden. While the reduced dosing frequency of newer bisphosphonates may be associated with improved adherence, the causes of non-adherence and how these may be addressed needs further research. Secondly, more effective models of service delivery are required to improve the currently low rate of treatment in elderly individuals sustaining a fragility fracture. Fracture liaison services have proved effective in identifying such individuals and initiating appropriate diagnostic and therapeutic intervention, but more effective communication between secondary and primary care is required to ensure that treatment recommendations are implemented.20
Acknowledgement
JEC acknowledges the National Institute for Health Research for research support.
Footnotes
This talk was part of the conference ‘Expounding boundaries of endocrinology’ which took place at the Royal College of Physicians on 27 January 2009 and was organised by Professor John Wass, Oxford Centre for Diabetes, Endocrinology and Metabolism
- © 2009 Royal College of Physicians
References








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.