
The incidence and prevalence of inflammatory bowel disease (IBD) continues to increase. Around 1 in 400 people in the UK have either ulcerative colitis (UC) or Crohn's disease, and approximately 10,000 people are newly diagnosed each year. Improved understanding of the aetiopathogenesis of IBD has contributed to the development of new drugs while efforts continue to optimise the use of currently available treatments.
This article will focus on recent advances in the medical management of IBD, however, advances in surgical management, diagnostics, endoscopy and imaging (see article on page 609–12) should not be forgotten.
5-aminosalicylic acid
5-aminosalicylic acid (5-ASA) remains the mainstay of treatment for mild to moderate ulcerative colitis for the induction and maintenance of remission. By contrast, although still commonly used by many, 5-ASA is at best only mildly effective in Crohn's disease.
Once-daily dosing
5-ASA has traditionally been taken in two to three daily doses. These regimens probably contribute to poor adherence which is well recognised in people who take 5-ASA.1 Recently, studies have compared the efficacy of once-daily mesalazine with divided doses. A new formulation of 5-ASA (Mezavant XL®) utilising a novel delivery system was found to be equally effective at inducing and maintaining remission in UC whether taken once daily or in divided doses.2,3 Subsequently, studies have been published showing that other formulations of 5-ASA are effective when taken once daily suggesting that this is probably a class effect.
Long-term use of 5-ASA reduces the increased risk of developing colorectal cancer associated with long-standing, extensive UC. Accordingly, measures to improve adherence, such as once-daily dosing, may have benefits in addition to decreasing relapse rates.1
Increased doses of 5-ASA
Given the tolerability and safety of 5-ASA, attention has turned to using higher doses of mesalazine to treat mild to moderate UC. In the ASCEND I study, more people with moderate UC taking oral mesalazine at a dose of 4.8 g/day had symptomatic improvement than those taking the standard dose (2.4 g/day). However, there was no improvement in remission rates and no benefit was demonstrated for people with mild UC.4
An alternative approach to increased oral dosing was examined in a trial in which people with extensive mild to moderate UC were randomised to receive 5-ASA enemas or placebo in addition to high-dose oral 5-ASA. Combination therapy was found to be more effective at inducing remission than oral therapy alone.5
Overall, increasing the dose of 5-ASA in active disease results in a moderate improvement in efficacy without a marked increase in side effects.
Corticosteroids
Corticosteroids remain one of the most effective ways of inducing remission and, accordingly, their efficacy is unlikely to be improved markedly. However, their inability to maintain remission and their serious side effect profile make their use unacceptable except for short periods.6 Advances in this area are focusing on methods of reducing toxicity, for example through using novel delivery methods.
Immunomodulators
Methotrexate and thiopurines (azathioprine and mercaptopurine) are used in patients with Crohn's disease to reduce disease activity, maintain remission and decrease steroid usage. In UC, thiopurines are more commonly used than methotrexate, probably because the original trials of methotrexate in UC were negative. However, problems with the design of these trials, along with evidence from retrospective studies suggesting that methotrexate is effective in about half of patients who fail to respond to or are intolerant of thiopurines,7 has resulted in increased use of methotrexate as a second-line immunomodulator in UC. Recently, thiopurine use has been optimised in several ways.
Adjustment of thiopurine dosing: thiopurine methyltransferase
It is now standard practice in many centres to measure the activity of thiopurine methyltransferase (TPMT), an enzyme involved in thiopurine metabolism, before initiating treatment with a thiopurine. This allows identification of the 1 in 300 people who will predictably develop bone marrow suppression due to deficiency of TPMT. Approximately 10% of people are TPMT heterozygotes (with intermediate activity) and require lower doses of thiopurines.8 Conversely, people found to have high levels of TPMT activity may require higher doses, although evidence for this is variable.9
Adjustment of thiopurine dosing: thiopurine metabolites
Further refinement of thiopurine dosing has become possible with the measurement of metabolites of thiopurine. In patients in whom standard doses of thiopurines have proved ineffective it is possible to identify whether they require higher doses, are poorly adherent, are resistant to therapy, or metabolise the
drug preferentially to an inactive/toxic metabolite.8 In an intriguing study, the latter group of patients have been shown to respond favourably to a combination of thiopurine and allopurinol; allopurinol, by inhibiting xanthine oxidase, alters the metabolic pathway resulting in an increase in the active metabolite of azathioprine.10 This combination of drugs was previously avoided due to their potentially fatal interaction together. They should only be used concurrently by experts experienced in their use together who have access to appropriate monitoring facilities.
Biologics
Anti-tumour necrosis factor (TNF) therapy has been used in more than 350,000 patients with IBD worldwide, and is licensed for use in both UC and Crohn's disease. While its efficacy is undoubted its expense has resulted in limited availability in the UK.
Ulcerative colitis
The ACT trials demonstrated that infliximab is effective in moderate to severe UC, although the proportion of patients remaining in remission six months later was only about 20%.11 The National Institute for Health and Clinical Excellence (NICE) has recently recommended that infliximab is not used for this indication.
Infliximab is also an effective rescue therapy for people with acute severe colitis.12 The relative ease with which it can be used has made it an attractive alternative to cyclosporine which requires close monitoring of drug levels. There are currently two ongoing trials addressing the issue of which of these drugs is more effective. In the meantime, new NICE guidance has suggested that cyclosporine should be used in preference to infliximab as rescue therapy in UC.
Crohn's disease
There are two anti-TNF agents available in the UK for the treatment of Crohn's disease; infliximab, a mouse-human chimeric antibody given intravenously, and adalimumab, a fully human antibody administered subcutaneously. Patients thus have a choice regarding route of administration. Furthermore, the GAIN study demonstrated that adalimumab was effective in patients who had lost response to, or could not tolerate, infliximab.13
It seems that infliximab and adalimumab have broadly similar activity in Crohn's disease for both the induction and maintenance of remission. Final NICE guidance regarding the use of anti-TNF in Crohn's disease is still awaited but, fortunately, seems likely to sanction maintenance therapy.
Anti-TNF drugs are also useful adjuncts for the treatment of a variety of extraintestinal manifestations, including pyoderma gangrenosum, uveitis and enteropathic arthritis.
Concomitant immunosuppression with anti-TNF drugs
There are concerns over the safety of combining immunomodulators with anti-TNF drugs particularly with regard to infections and malignancies such as lymphoma.14,15 Recent studies have, therefore, examined the need for concomitant immunosuppression when using anti-TNF drugs. It is clear that concurrent use of methotrexate or thiopurines improves the efficacy and safety of infliximab when the latter is used intermittently.16 However, when scheduled retreatment is used to maintain remission, the evidence regarding the need for concomitant immunomodulation is less clear (Table 1).
Summary of controlled trials examining the need for concomitant immunosuppression in patients with Crohn's disease receiving scheduled maintenance therapy with infliximab.
Key points
High-dose 5-aminosalicylic acid is safe and effective
Earlier use of immunomodulators and biologics in Crohn's disease may alter the natural history of the disease
Combining immunomodulators, steroids and anti-tumor necrosis factor drugs in people with inflammatory bowel disease greatly increases the risk of infectious complications
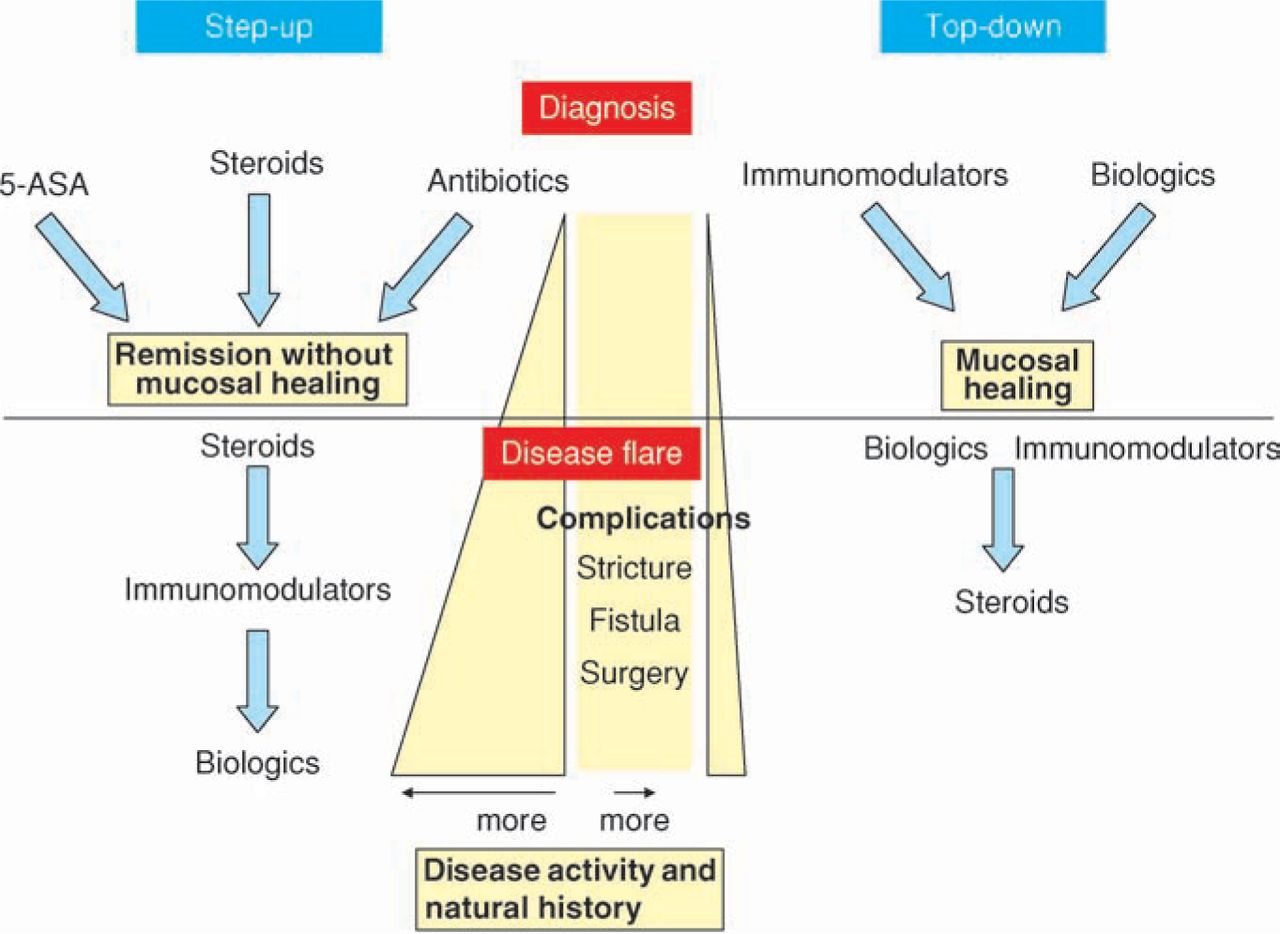
Crohn's disease: top-down or step-up (Fig 1)

Step-up versus top-down therapy for
In the past, medical management of Crohn's disease involved a combination of 5-ASA, intermittent steroids and/or antibiotics (depending on the physician's preferences) before moving on to immunomodulators and then biologics. However, with this approach, there was often an inevitable progression to long-term complications such as stricture and/or fistula formation, often necessitating surgery. The holy grail of managing Crohn's disease would be to alter the natural history of the disease. The concept of top-down therapy involves using biologic and/or immunomodulating therapy at or soon after diagnosis in an attempt to prevent later complications. Early data provide some support for this concept although longer and larger trials are needed before it can be adopted as standard treatment: certainly the risks of unnecessarily treating people with mild disease with toxic drugs need to be considered.17 In the meantime, the trend in the UK is for earlier use of immunomodulators.
Others
As is always the case in IBD, a number of new drugs and technologies are at various stages of development and investigation. Of these, few will prove to be effective or safe enough to make a major impact. However, the development and availability of biologics and other novel agents are likely to continue to improve the treatment of IBD over the coming years: for example, natalizumab, an anti-α4 integrin with proven efficacy in Crohn's disease,21 is already available for use in the USA for people who have failed treatment with an anti-TNF drug.
More unusual treatments that have been shown to be effective in recent years include aloe vera,22 Trichuris suis ova (a whipworm),23 and a variety of probiotics.24 However, such novel therapies tend to be
Crohn's disease.
targeted at people with mild disease, many of whom can be effectively treated with standard therapy.
Conclusion
The challenges faced by clinicians managing patients with IBD remain considerable. While continued development of novel agents to address these challenges is vital, optimising the use of those drugs that are already available, even those that have been in use for half a century, is equally important.
- © 2009 Royal College of Physicians
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.