
ABSTRACT
A significant proportion of COVID-19 patients show evidence of hyperinflammation (HI), of which secondary haemophagocytic lymphohistiocytosis (sHLH) is the most severe manifestation and diagnosed with HScore. Using a COVID-relevant modification of the HScore (%HScore), we set out to determine the prevalence of sHLH in 567 COVID-19 inpatient cases.
The overall incidence of individuals with an 80% probability of sHLH in our COVID-19 cohort was 1.59% on admission and only rose to 4.05% if calculated at any time during admission. This small cohort as defined by %HScore showed no excess mortality compared with the whole cohort. Overall, %HScores were lower in older patients (p<0.0001) and did not reliably predict outcome at any cut-off value (AUROC 0.533, p=0.211, odds ratio 0.99).
Our study demonstrates that a modified version (%HScore) of the conventional sHLH scoring system (HScore) does not enable risk stratification in people hospitalised with COVID. We propose further work is needed to develop novel approaches to predict HI and improve trial stratification for HI directed therapy in people with COVID-19.
Introduction
Mortality from SARS-CoV-2 infection causing COVID-19 in hospitalised patients in the UK has been reported to be 25.7%.1 The principal cause of death due to COVID-19 is respiratory failure due to acute respiratory distress syndrome.2 Early reports have suggested that a subgroup of individuals suffer a hyperinflammatory state with high mortality which is associated with high levels of IL-6 and C-reactive protein (CRP).3 Hyperinflammation (HI) has been previously described secondary to acute infection and termed cytokine release syndrome / cytokine storm (CRS/CS), macrophage activation syndrome (MAS), macrophage–cytokine self-amplifying loop (MCSAL) and secondary haemophagocytic lymphohistiocytosis (sHLH). HI in COVID-19 has drawn attention because of overlapping features with these classical syndromes, notably high fever, striking acute phase response and coagulopathy. Yet despite the descriptions of these overlapping conditions, characterised by a rapid increase in systemic inflammation, there remains no consensus as to the precise definition of what constitutes HI.4 However, early reports to date suggest that in COVID-19 the inflammatory response, as indicated by ferritin and CRP levels, is lower overall than in classical HI syndromes such as sHLH.5 HI in COVID-19 may either be a different inflammatory cascade to that induced by sHLH, or could possibly reflect differences in the spectrum of HI severity. Therefore, it is of interest to determine the prevalence of sHLH in people with COVID-19. In addition, we have applied modified sHLH criteria (%Hscore) to a cohort of people hospitalised with COVID-19 to determine whether such analysis illuminates debate around the HI disease spectrum, as has been previously suggested.6
While it is accepted that viral infections are the commonest cause of sHLH,7 symptoms of HI resemble those of general sepsis; therefore HI has generally been under-recognised at an early stage, leading to high mortality.8 It is likely that strategies to identify HI and targeted intervention will offer the most effective approach to the management of HI in COVID-19. Indeed, as well as anti-IL-6,9 other cytokines released in HI for which existing biologic therapies are available could also represent potential targets for intervention; these potential therapies include inhibitors of TNF-α (infliximab), IL-1 (anakinra), and JAK (eg ruxolitinib). Randomised controlled trial data have shown that the anti-inflammatory agent dexamethasone can reduce mortality in severe COVID-19 in an unselected cohort1 and targeted anti-inflammatory anti-IL-6 therapy in an unselected intensive care COVID-19 population showed reduced mortality in the intervention vs control arms (22.2–28% vs 35.8%, respectively).10 While impressive, these results suggest that targeted anti-inflammatory interventions given early to individuals with HI may show even greater benefit in mortality, and this approach may be the key to reducing the morbidity of COVID-19 by preventing escalation to high dependency and intensive care. To facilitate diagnosis of sHLH, the most extreme form of HI, the ‘HScore’11,12 has been developed because of evidence that early recognition and intervention is beneficial (Table 1).12 While the HScore has some limitations,13 including that it was not validated on a critical care population, and that despite its use sHLH is still under-recognised because of the complexity of the syndrome, some authors have recommended using the HScore in COVID-19.14 A recent report using this approach has provided evidence that the prevalence of sHLH is low (7.5%) in intensive care patients with COVID-19 (n=40). We therefore set out to examine the HScores in people hospitalised with COVID-19, and to explore the prevalence of sHLH as assessed by a COVID-modified H score across the whole hospitalised COVID-19 cohort.
HScore and %HScore algorithm
Patients and methods
Following national ethical approval (Identification of Novel Factors Leading to Activated Macrophage Expansion in COVID19 and related conditions to guide targeted intervention, Inflame COVID-19 Study, NRES 286016) which included retrospective collection of virus-induced sHLH controls, we recruited all cases of COVID-19 infection that tested positive for SARS-CoV-2 viral RNA in our laboratory and were admitted to University Hospitals Southampton NHS Foundation Trust between 7 March 2020 and 9 June 2020 (n=626). Additionally, we recruited a retrospective cohort of sHLH (viral infection associated) from the same institution based on confirmed diagnosis recorded as ICD-10 D76.2 (n=16).
Structured and semi-structured data were accrued from the trust integration engine using SQL Developer 4.2 queries and then cleaned/transformed using python 3.7 and associated libraries: numpy and pandas. Analysis was performed using matplotlib, seaborn and scipy. Statistical analysis was undertaken using GraphPad, Prism (8.4.3).
The classical HScore (Table 1) includes three clinical parameters (immunosuppression, pyrexia, organomegaly), five blood tests (triglyceride, ferritin, transaminase, fibrinogen, cytopenia), and bone marrow aspirate features. Each of these is weighted by variable and a score based on the value/result is summated to provide an overall score ranging from 0–337. This value is then utilised to calculate a probability of a diagnosis of HLH; for example, an HScore of ≤90 equates to a <1% probability of sHLH, while there is a >99% probability with an HScore of ≥250. We calculated the HScore based on parameters available retrospectively. As expected from the infective precautions taken on COVID-19 patients, or from the lack of clinical indication for the investigation, few data were available on palpable hepatosplenomegaly or bone marrow aspirate histology, and on analysis we found the electronic data on immunosuppression status to be unreliable. Therefore, we excluded these three parameters. To account for these missing values we created a modified HScore calculated from the percentage points from the available parameters expressed as a percentage (%HScore, Table 1).
The primary outcome utilised in this study was binary: discharge from hospital or death in hospital. Admission date was an unreliable marker of disease onset as some of our cohort contracted COVID-19 after prolonged periods in hospital and therefore the time of initial infection was unclear. Clinical teams arranged testing as symptoms presented and therefore, to facilitate comparison between cases, investigation parameters were normalised to the date of SARS-CoV-2 viral RNA laboratory confirmation and outcome data tabulated from day –1 to day 21.
Results
Considering the influence of age on mortality, we examined our dataset for the number of recorded HScore parameters (day –1 to 4), as distributed by age (n=621) (supplementary material S1a). This showed that the individuals for whom few data points were available were more likely to be older (p=0.0025). To address this source of potential bias, we removed individuals with fewer than three data points from further analysis. Subsequent analysis of the distribution of data points in the reduced cohort (n=567) confirmed no association between the number of data parameters and age (p=0.094), confirming that the analysis was valid across all age groups. The characteristics of the 567 eligible cases (41.8% female) showed a high prevalence of comorbidities in line with the high overall average age (median 71 years, interquartile range [IQR] 54–82; Table 2).
COVID cohort characteristics and comorbidities
As expected, because of missing data, the classical HScores in our cohort were low (maximum 147, equivalent to 43.6% of the maximal possible HScore). However, %HScore measured in the first 5 days of illness (day –1 to 4 after laboratory virus confirmation) was a very strong predictor of the %HScore during the whole admission (r=0.8499, p<0.0001, Fig 1a), and good correlation was observed between %HScore and classical HScore (r2 =0.88; see supplementary material S1b). Interestingly, examined in isolation, none of the parameters in the %HScore measured at day –1 to 4 differentiated those who would survive or die except for white cell count, where those who survived versus died showed a lower mean value (6.63 vs 8.27 × 109/L, p= 0.000071; false discovery rate <1%; see supplementary material S1c).
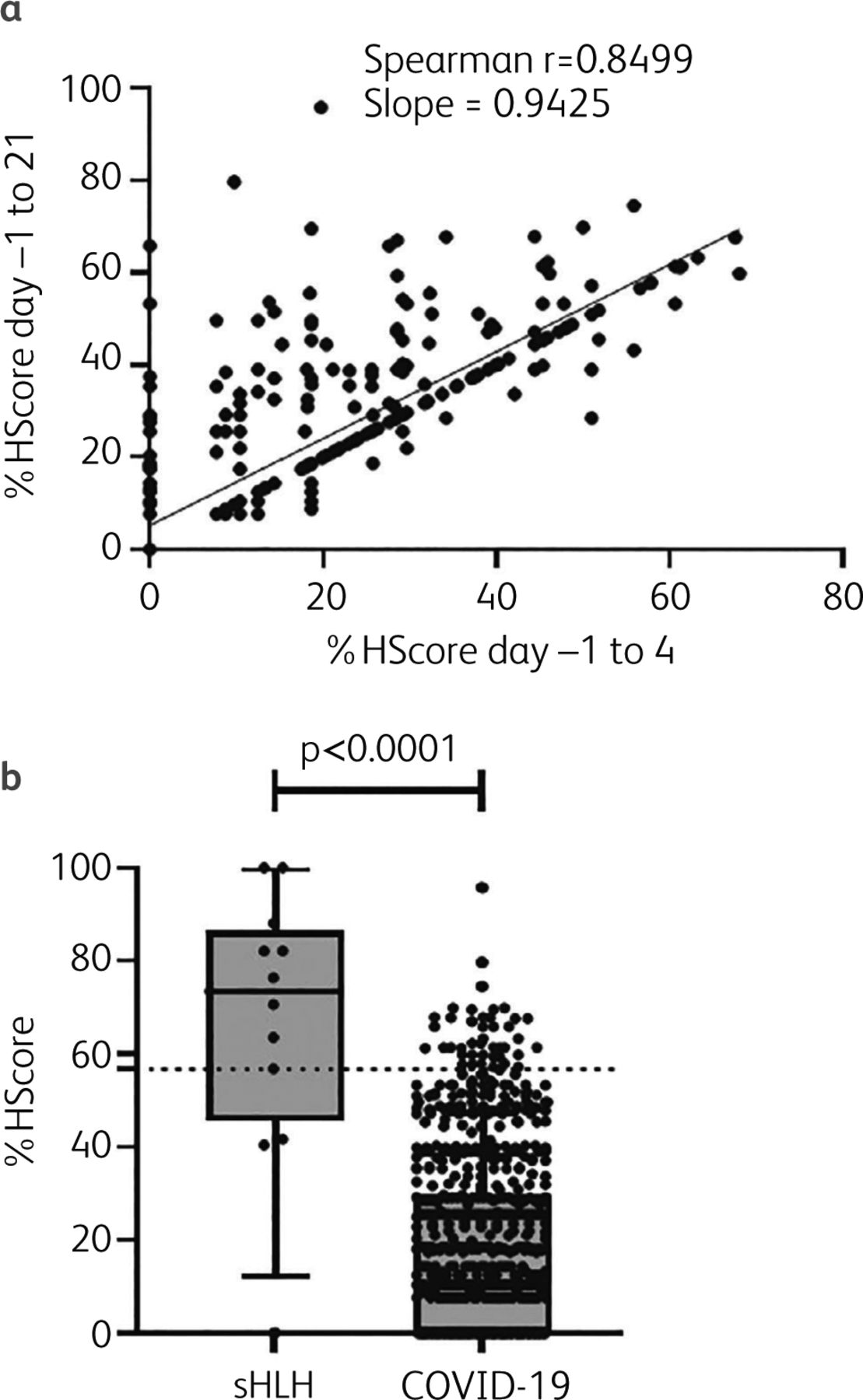
sHLH shows a higher %HScore than COVID-19, but %HScore in COVID-19 shows no correlation with mortality. a) %HScore as measured from data points recorded at virus diagnosis timepoints day –1 to 4, versus day –1 to 21. Spearman's correlation coefficient (r) presented. n=567. b) Plot of %HScores from a retrospective cohort of secondary haemophagocytic lymphohistiocytosis (sHLH) versus COVID-19. Dotted line at 56.7% (80% probability of HLH). Error bars represent 10–90% confidence. Mann Whitney test presented.
Compared to the sHLH cohort, COVID-19 showed a significantly lower %HScore (median 73.47% vs 18.13% respectively, p<0.0001, Fig 1b). An HScore which predicts an 80% probability of sHLH is reported to be 191/33711 which is equivalent to a %HScore of 56.7%. If %HScore was calculated from ‘worst’ values at any time day –1 to 21, the proportion of COVID-19 cases meeting the sHLH threshold was only marginally higher at 4.05% (23 of 567). At the early time point (virus day –1 to 4), these criteria were met by only 1.59% (9 of 567) COVID-19 cases. Surprisingly, for those individuals with a %HScore above the sHLH threshold, there was no increase in mortality as compared to the whole cohort mortality of 30.43% vs 30.69% respectively (p>0.05).
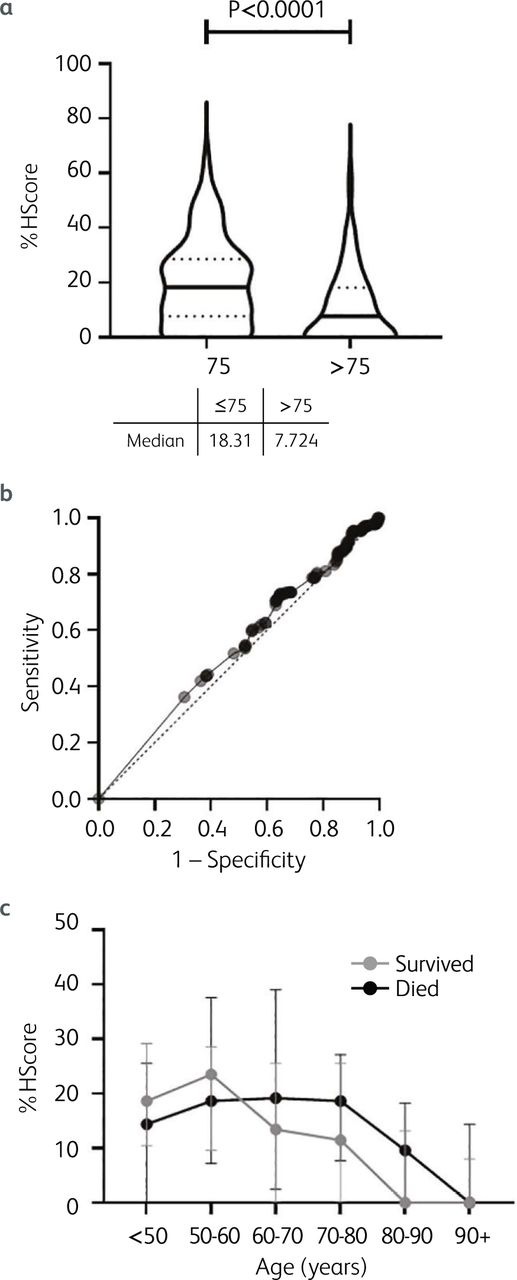
In order to determine the role of %HScore for early identification of HI across the whole cohort, we restricted analysis to scoring from day –1 to 4, and then correlated this early measure with mortality at any time point. As seen in many studies in COVID-19, overall mortality was strongly predicted by patient age (p<0.0001; median age survivors 64 years, IQR 49–76; mean age of those who died 81 years, IQR 73–87; see supplementary material S2a). At a threshold of 75 years of age, the increased risk of mortality was significant (odds ratio [OR] 7.295, 4.89–10.8, p<0.0001). However, age conferred a strong negative correlation on %HScore (Spearman r = –0.305, –0.38 to –0.226, p<0.0001; see supplementary material S2b), across the cohort. Strikingly, the median %HScore was significantly lower (p<0.0001) in the older age group: >75 years median %HScore 7.724 (0.0–18.16) vs ≤75 years median %HScore 18.31 (7.72–28.57) (Fig 2a). Receiver operator characteristics (ROC) over the whole cohort suggest that at any threshold, %HScore is not useful as a predictor of mortality in COVID-19 (AUROC 0.533, p=0.211; OR 0.99, 0.98–1.00) (Fig 2b). However, because of the very strong association between age and mortality, it is important to stratify for age to examine the effect of %HScore on mortality. Stratification showed that the negative correlation between age and %HScore was highly significant in both those who survived (r = –0.307, –0.441 to –0.164, p<0.0001) and those who died (r = –0.309, –0.441 to –0.164, p<0.0001) and that there was no difference in %HScore between those who died and survived (p = 0.3125) (Fig 2c).

Age, %HScore and risk of mortality in COVID-19. a) Violin plot of %HScore in those ≤75 versus >75 years (n = 567). Horizontal bars represent median value, interquartile range dotted. Mann Whitney statistic presented. b) Receiver operator characteristics of prediction of mortality by %HScore. c) %HScore in cases who died (black dots) versus survived (grey dots) by age stratification. Error bars represent 25–75% confidence interval.
Discussion
We report here the largest dataset assessing sHLH incidence by %HScore in COVID-19 to date (n=567), which exceeds the 312 sHLH cases in the original series identifying the HScore11 and the 40 cases where HScore was applied to intensive care patients.13 During COVID-19, inevitably some parameters in the HScore were not obtainable, and our study demonstrates that use of the HScore during the pandemic is challenging. However, to address missing data, we utilised a mathematical programmed approach to facilitate rigorous data collection from centralised hospital electronic records and utilised cross-checking and cross-validation to optimise data cleaning, thus avoiding collection errors, while minimising missing data. Furthermore, to identify the subgroup with sHLH in COVID-19, we undertook a stringent approach to the analysis and did not impute any missing values and instead designed a COVID-modified HScore, %HScore.
In this report, we demonstrate that sHLH, as measured by the %HScore, is rare in hospitalised cases of COVID-19, similar to the reports of low incidence in intensive care settings.13,14 Indeed, we estimate that sHLH arises in 1.59% of hospitalised COVID-19 cases early in the course of the illness, and only rising to 4.7% over the whole admission. Surprisingly, mortality in the %HScore-sHLH cohort of COVID-19 cases meeting 80% probability showed no excess mortality as compared to the whole cohort (30.43% vs 30.69%). We emphasise some caution when translating this finding to cases diagnosed by the traditional HScore because of the natural limitations of undertaking this work in a pandemic meant that the full quota of HScore parameters (including, for example, the presence of haematophagocytosis on bone marrow aspirate findings) was impossible to attain on any COVID patient. Therefore, the cases with high %HScores here may not necessarily have achieved a similar HScore. In addition, this analysis did not stratify for therapy and it remains possible that medical interventions may have modified the mortality of the cases with higher scores. We stress that COVID-19 patients demonstrating high likelihood of sHLH should still be treated with standard treatment protocols for sHLH.15
It is notable that the index cohort of sHLH cases used to define the HScore had a median age of 51 years (IQR 36–64),11 as compared to our COVID-19 patients whose median age was 71 years (IQR 54–82). In addition, we identified that younger patients have significantly higher %HScores (p<0.0001) and additionally show that when stratified for age, there was no difference in %HScore. Why %HScore (and HScore parameters) decline with age in the context of COVID-19 is not clear but may predominantly reflect immunosenescence. In part this may be explained by responses to COVID-19 generally acting in an opposite direction to HLH. For example, while pancytopaenia would produce a higher %HScore, it seems that responses to the virus in older individuals are more likely to show increases in circulating white blood cells and platelets, which would clearly drive the %HScore down. Therefore, the association between reduced %HScore and age, as well as the relatively low mortality of sHLH in COVID-19, suggests that waning immunity with age may actually be protective against sHLH-type responses in COVID-19.
Although it is possible that high %HScores in COVID-19 do reflect dysregulated immunity, the absolute difference between those who die and survive is small, suggesting that the individual with a high %HScore may lie at or close to a tipping point between harm and benefit from innate inflammation. Therefore, it remains unclear what the effect of broadly applied anti-inflammatory therapies will have on older individuals in particular and a careful balance needs to be struck when designing clinical trials of anti-inflammatory therapies to determine where an individual lies on the risk spectrum of an excessive inflammatory response versus an impaired anti-viral response. Improved endotyping of COVID-19 cases by classification of validated biochemical and molecular phenotypes to identify the subgroup who will benefit from anti-HI strategies is critical and these should be used to stratify COVID-19 patients in the next phase of clinical trials; early reports look promising.16 This emphasises that interventional approaches need to be guided by deep understanding of the inflammatory processes underway at an individual patient level. Some efforts have also been made to develop markers of HI, but the index cohorts remain small.17
In summary, we present data which show that when applying a modified HScore (%HScore), sHLH is uncommon in hospitalised cases of COVID-19 and in cases where scores are higher, this does not predict outcome. Why %HScore (and most HScore parameters) decline with age in the context of COVID-19 is not clear but may predominantly reflect immunosenescence in this mainly elderly cohort of patients. We suggest that waning immunity with age may actually be protective against sHLH-type responses in COVID-19 patients. However, several studies have shown the benefit of anti-HI therapy in COVID-19 patient cohorts (dexamethasone in oxygen-dependent patients and tociluzimab in ITU patients). We show here that the conventional scoring system for sHLH will not identify the group who are most likely to benefit from such therapy. Indeed, while the work here shows that in COVID-19, sHLH is uncommon, this work does not undermine the utility of the HScore as a diagnostic tool for sHLH in COVID-19 and we encourage readers to actively manage sHLH in accordance with international guidance.15 Our study demonstrates the importance for novel algorithms to predict HI in COVID-19 as well as randomised controlled trials targeted at this patient group.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/clinmedicine:
S1 – Analysis of available HScore parameters versus age.
S2 – The effect of age on overall survival and %HScore in COVID-19.
- © Royal College of Physicians 2021. All rights reserved.
References








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.