
ABSTRACT
The aim of this study was to characterise the patients and outcomes of an acute medical take. 107 consecutive patients admitted to the acute medical take in a tertiary referral centre were investigated and followed-up at 6 months. Data were collected within the following domains: demographics, observational parameters, initial clinical care, outcomes, patient flow and follow-up. There was a high prevalence of renal dysfunction (27%) and possible/probable sepsis (56%). 22% of patients benefitted from early advanced imaging. Average length of stay (LoS) was 8.15 days for general medicine patients vs 3.23 for patients treated by specialist teams (p < 0.05). LoS was 11.1 days longer if patients’ biochemistry suggested probable sepsis (p < 0.05). 31% were readmitted within 6 months. We conclude that patients presenting to the acute medical take are physiologically stable, though frequently present with renal impairment or sepsis, and that specialist patients experienced a shorter LoS. These data are important in planning the future provision of acute medical care.
Introduction
Hospitals in the UK are under significant pressure to manage emergency medical admissions.1 There were 15.2 million UK hospital admissions between September 2011 and August 2012.2 Acute admissions have increased by 37% over the last decade and are now responsible for 65% of hospital bed days in England.3 The acute medical take is the major interface between community and hospital acute care.4
Current literature relating to medical admissions focuses on examining a single disease entity, biochemical marker, mode of presentation or appropriateness of a scoring system. There is very little that examines the full variety that constitutes an ‘acute medical take’. Lim et al used the CURB-65 score to characterise and attempt to standardise treatment for those presenting to hospital with community acquired pneumonia.5 Similarly, the ‘surviving sepsis campaign’ by Rivers et al6 and acute kidney injury (AKI) work by Forni et al7 have taken an approach to analysing and managing acute hospital admissions that focuses on a single disease entity.
This paper is the first attempt to characterise what constitutes an ‘acute medical take’ in the United Kingdom. Data aiming to characterise patients presenting to UK hospitals are collected by the Hospital Episodes Statistics Service but at a much broader level than is described here. Similar studies to this one have been carried out in developing countries such as Nigeria.8 Such data can be used to optimise health service delivery at the hospital and community level, guiding appropriate staff training and resource use and reducing hospital admissions and healthcare costs.9,10
Definitions used in this paper are given in Box 1.
Methods
The study took place in a 1250-bed tertiary referral teaching hospital in the West Midlands offering both percutaneous coronary intervention (PCI) and stroke thrombolysis, among other interventions. 107 consecutive patients admitted on an acute medical take in October 2012 were recorded and their electronic records analysed. The medical take covered a 24 hour period from Sunday to Monday evening. All patients were admitted via the emergency department (ED), including general practitioner referrals, referrals from smaller district general hospitals and those admitted via FAST positive or ST segment elevation myocardial infarction (STEMI) pathways operating in the hospital.
The hospital operates a triage system with an ED consultant or senior registrar directing patients directly to an appropriate speciality. All patients allocated to medicine then proceed through the single ‘acute medical take’ before being assigned to specialist care based on the decision of the admitting medical team, or remaining under general medicine; care of the elderly is included under general medicine. The patients were admitted under the care of four acute consultant physicians (including the current author, A Stein). Patient observations are triaged using the modified early warning score (MEWS) system.11,12
Data collection occurred within six categories:
> demographics (gender, race, age, comorbidities)
> laboratory and observational parameters (serum urea and electrolytes, full blood count, modified early warning score and evidence of AKI and sepsis as defined above)
> initial clinical care (use of advanced imaging, initial and final diagnoses, specialist input, electronic discharge summary completion rate)
> outcomes (LoS and mortality)
> patient flow (ICU admissions, appropriate first/final ward, readmissions, zero-day admissions
> 6 month follow-up (mortality and re-admissions, including time to re-admission, LoS and diagnosis at readmission).
Data were descriptively analysed with two sample t-tests to assess the impact of sepsis and specialist care on length of stay.
Results
Demographics
Average age of admission was 61.8 years (range 20–98); 44% (48) were aged over 70 (see Fig 1). 55% (59) were female. 86% of patients were of Caucasian ethnicity,10% Asian and 4% black ethnicity. The majority of patients presented with co-morbidities (modal average 2, mean 1.89); specialist care patients had on average 2.1 co-morbidities, compared to 1.83 for general medical patients (p = 0.24).

Age distribution of patient admitted to the acute medical take.
Laboratory and observational parameters
Haemoglobin levels were similar between genders (mean haemoglobin 123g/l). 10 patients were hyperkalaemic (K+ greater than 5.0mmol/l), 6 were hypokalaemic (K+ below 3.5mmol/l). 16 patients were hyponatraeimic (Na below 135mmol/l) and 4 hypernatraemic (Na above 145mmol/l). 20% of admissions met criteria for probable sepsis, and 36% possible sepsis. Of patients with a creatinine (n = 100), 27% had AKI or chronic kidney disease (CKD) with 17% having CKD. One patient was diagnosed with an ST elevation myocardial infarction (STEMI) and another with a stroke. 94% presented with a modified early warning score (MEWS) of ≤2, with 6% scoring 3 and 2.85% >3.
Box 1: Definitions

Initial clinical care
22% of patients underwent advanced imaging in the first 48 hours. There was strong correlation between initial and final diagnoses, with 14% of diagnoses changing substantially (different organ system and/or pathological process) from that decided upon at initial clerking. One diagnosis was changed by a specialist team. The distribution of patients referred to specialist teams was distinct, with the average age being 20 years younger and a particularly large number of patients among the 40–49 age group (Fig 2).
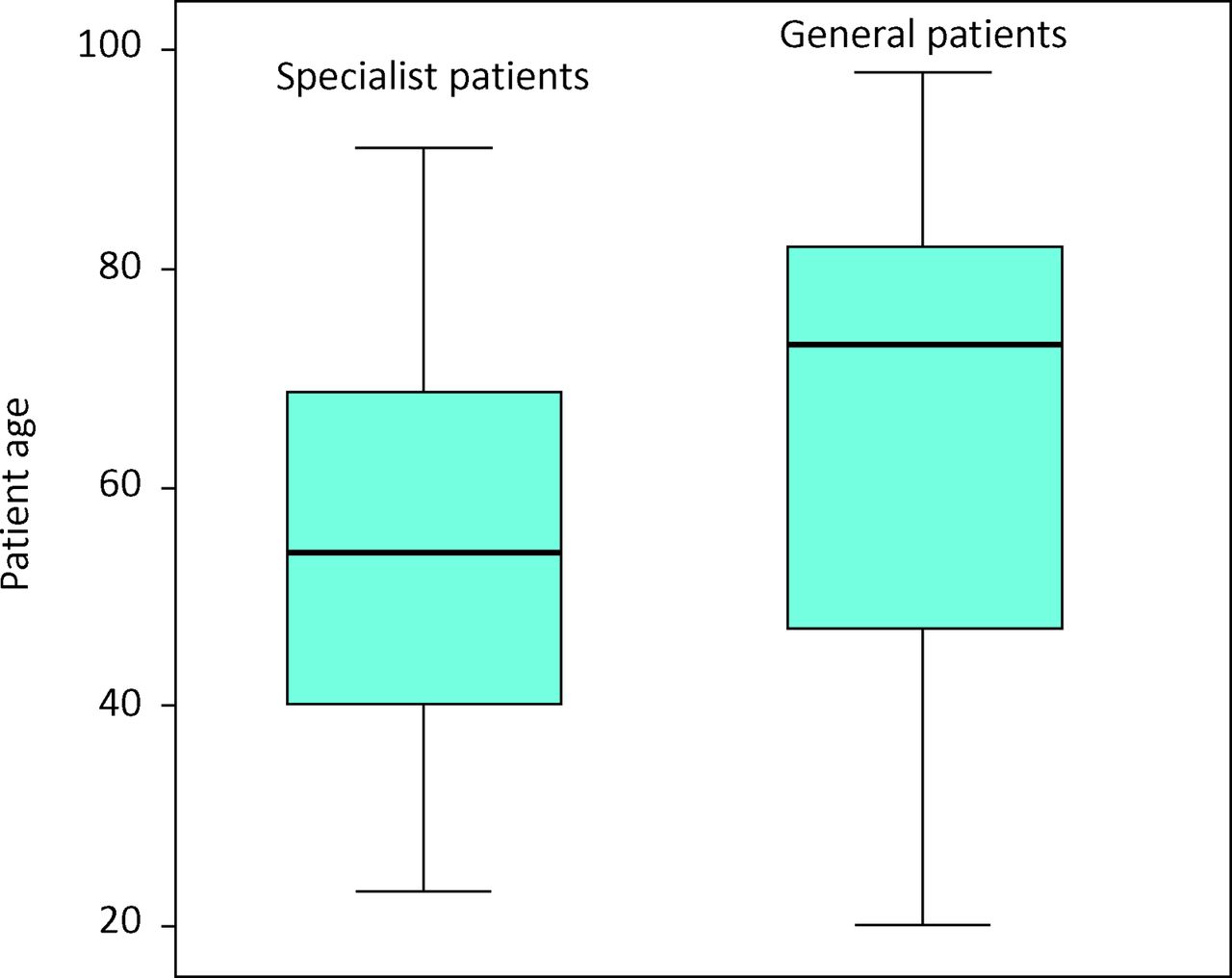
Age differences between specialist and generalist patients.
24% (26) of patients lacked e-discharge summaries, with 21% (16) of the general medical patients lacking summaries, compared to 28% (10) of the specialist patients. Patients lacking e-discharges had an average length LoS of 4.16 days compared to 7.57 for patients who had an e-discharge summary completed.
Outcomes
Five patients (4.7%) died as inpatients, three in the first 24 hours. Patients stayed on average 6.76 days; 40% were discharged within 48 hours. Patients treated by specialist teams stayed on average 3.23 days compared to 8.15 for general medical admissions (p<0.05). Patients admitted with biochemistry consistent with probable sepsis had a mean length of stay of 13.8 days vs 2.70 for those without (p<0.05). Patients presenting with renal impairment experienced an average length of stay of 9.2 days vs 5.6 days for patients without renal impairment (p = 0.12). Neither gender nor age impacted on length of stay.
Patient flow
11% of patients were admitted to an inappropriate ward. Three patients were admitted to ICU with two of these dying. 23% of patients were re-admissions. Re-admission patients had more co-morbidities (mean 2.32 co-morbidities) and an increased length of stay (8.56 days). Men accounted for a greater percentage of readmissions, with 15% of male patients classified as readmissions compared to 9% of women. 20% of inpatients were classified as ‘zero day’ admissions where ambulatory care would have been possible were such pathways available within the hospital trust.
Six month follow-up
Seven patients (6.5%) died within 6 months of discharge based on hospital records. Combined with inpatient deaths this gives an 11% combined 6-month mortality. 31% of patients were re-admitted within 6 months. 36% of general medical ward-based patients were re-admitted within 6 months vs 19% of specialist-ward based patients. Average time to re-admission was 59.2 days. 50% of those readmitted had a similar diagnosis (affecting the same organ system) to the index admission. Average LoS for re-admissions was 7.71 days.
Discussion
Patients presenting to an acute medical take, while usually physiologically stable (low MEWS), typically present with complex pathological states, a high prevalence of renal impairment and potential for sepsis, on a background of multiple co-morbidities. There appears to be a ‘recurrent-admission cycle’ with almost a quarter of the acute medical take involving recently discharged patients, and approximately the same amount likely to be re-admitted within 6 months. It is perhaps predictable this involves a particular subset of patients with increased co-morbidities and LoS. Interestingly our study did not demonstrate any link between age and LoS. A possible reason for this could be that elderly patients with a low physiological reserve are admitted unwell, but for relatively simple problems who are thus easy to treat and discharge. Alternatively the relatively low socio-economic status of the study hospital's population (30% of the city's population live within the lowest quintile of deprivation in England13) mean social delays to discharge are not limited to the elderly but are also an issue among younger patients.
A significant minority of patients leave without an electronic discharge summary. This may reflect an acute care system ‘under pressure’ with high bed occupancy rates together with the need to achieve Department of Health/NHS England Emergency Department flow targets and a desire to discharge patients quickly – this is supported by the statistically significantly shorter LoS for patients lacking an e-discharge.
Most patients are managed by non-specialists for their particular condition, usually on a ward specialising in treating other conditions. The initial diagnoses made on admission are typically those the patients are discharged with. These diagnoses are developed with little advanced imaging or significant specialist input. While in part this could be due to the diagnostic accuracy of acute physicians, it could reflect a reluctance to change diagnoses once they are made. This increases the importance of utilising imaging and specialist input early to ensure an accurate first diagnosis, with the risk of inappropriate management if this is wrong. Incorrect diagnoses could result in increased re-admission rates and emphasise the importance of high quality initial patient care on the acute take. Improving initial care and improving ambulatory pathways could allow a significant number of admissions to be avoided; however, the impact on re-admissions would need to be evaluated.
This study provides an interesting insight into the effect of the continuing trend towards clinical specialisation. The data suggest that specialist physicians have a limited early role in diagnosing patients admitted to an acute medical take, usually accepting the diagnosis decided upon by the admitting team. Those patients who move to specialist care are typically younger, and enjoy a shorter hospital stay and reduced risk of re-admission within 6 months. The reasons for these observations are unclear; younger patients potentially have fewer co-morbidities than older patients thus reducing the chance of complicating factors – be they biological, psychological or social – which could allow earlier discharge; however, our overall data suggest age alone does not significantly impact on LoS. Nor do these factors explain the higher rates of young referrals to specialist care. Specialist patients were also noted to have a reduced rate of completed e-discharge summaries. This suggests there is a consequence/cost to the faster discharges. Above all, these data demonstrate that further work focused on the role of specialisation is needed, so both general and specialist care teams can be resourced appropriately.
The high prevalence of renal impairment amongst acute admissions is not a new observation.14,15 Previous studies show a frequency of 30%, whereas in our study, 27% was seen. In contrast to previous studies,16 we demonstrate only a slightly increased length of stay as a consequence of renal impairment. The high rates of potential sepsis among the acute medical take is a new observation,17 and an important one given the statistically significant increased LoS as a result. This could be a consequence of intravenous antibiotics often requiring inpatient delivery, thus placing an absolute lower threshold on length of stay. This emphasises the importance of antibiotic stewardship in order to keep intravenous treatment durations to a minimum. Taken together, the high rates of sepsis and kidney injury strongly argue for the inclusion of screening bloods for these conditions at the point of entry to medical care (ie at triage), supported by appropriate scoring systems eg the RIFLE classification for AKI.18
When considering readmissions it is important to note that the average time to readmission was 59.2 days, suggesting that current financial incentives for hospital trusts to minimise readmissions within 28 days may be insufficient in their scope, and that longer term incentives and support are needed. Despite this elongated time to re-admission, half are still for a similar reason to the index admission. Our results suggest it is possible to identify a cohort of patients at increased readmission risk – male, co-morbid general medicine patients. Given the increased LoS for readmissions, this subgroup of patients warrants further study.
While these data provide interesting areas for consideration, there are a number of limitations. This study is observational, providing a snapshot of a single 24 hour take in a single tertiary referral centre. That snapshot occurred from a Sunday night to a Monday night, with the proximity of a weekend potentially having an impact on the results. Repeating this exercise at other centres and for a longer time period would provide useful comparisons. Patients admitted to other local acute trusts will not be included in readmission data here, nor will patients dying in the community be included in mortality statistics. One of the important findings of this study – the significantly increased LoS for patients with probable sepsis – relies on a proxy measure of sepsis risk rather than a full diagnosis of systemic inflammatory response syndrome and infective presence. However the simplicity of this definition is also its strength, making it an easy tool to aid in the identification of potential long-stay patients. Finally, this study focuses only on those patients admitted via the acute medical take. In contrast the total cohort of medical patients within a hospital will include those admitted electively or those admitted through other specialities but then transferred to the medical teams. These are an important and potentially under-recognised (and under-studied) population of patients.
Acknowledgements
The authors would like to thank the Royal College of Physicians’ Future Hospitals Commission Group.
- © 2014 Royal College of Physicians
References








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.