
During his ride to work on the London underground earlier this summer, your correspondent was interested to spot a sentence in the editorial columns of a leading newspaper, which read ‘.… it is shocking that it took the inspectors so long to identify and document the problem …’ This sentiment had particular resonance for him in the context of the Future Hospital Journal (FHJ), in that a principal driver for the work of the Future Hospital Commission (FHC) emerged from the review of the Mid Staffordshire NHS Foundation Trust by Sir Robert Francis QC. There, the failure not only of inspectors and regulators, but also of clinicians (in the widest sense) and their leaders, managers and inspectors, to identify problems in that Trust, resulted in shocking patient neglect, and saw the NHS at its lowest ebb for decades.
However, the sentence did not refer to Mid Staffordshire, but rather to the recent ‘Trojan horse’ episode in Birmingham: the allegations of infiltration of school governing bodies by those seeking to advance specific political and/or religious agendas. The immediate reaction of politicians was to propose that state schools should face unannounced spot inspections.
Whether the threat of an inspection, announced or not, improves any public service in many ways underpins the special focus of this issue: regulation and the regulators. The inspection mantra has been applied to other public services, many of which seem to be increasingly under the cosh. Your editor had time to recall without difficulty (partly thanks to a signal failure at Embankment station) the Lawrence Inquiry into the conduct of the Metropolitan Police, where the term ‘institutional racism’ was first coined; the Saville Inquiry, which examined the events of 30 January 1972 (‘Bloody Sunday’) in Londonderry (it finally published its findings in 2010 and reportedly cost £200 million); the Leveson Inquiry into the culture, practices and ethics of the British press; the Hutton Inquiry, set up to investigate the circumstances surrounding the death of David Kelly; and the inquiry into MPs’ expenses led by Sir Thomas Legg. Arguably all these inquiries represent a genuine disenchantment of the general public with aspects of public life or services. All of them, the Francis Report included, referred to the need for improved governance, scrutiny, and oversight with the ultimate aim of correction.
In certain cases, however, it has been the regulators and inspectors themselves who have come under scrutiny. The effects of the Mid Staffordshire and Winterbourne View scandals, and the death of Peter Connelly (also known as ‘Baby P’) – and indirectly that of Victoria Climbié (investigated by the inquiry of Lord Laming) – produced a major shake-up in the role and leadership of the Care Quality Commission (CQC), up to and including the resignation of the chair. A root-and-branch review of the CQC's role and inspection systems is only now nearing completion, and suggests that the inspectors themselves are as challenged as the bodies they inspect.
The number of inquiries tends to suggest that the British public has become disillusioned with politicians, and, by inference, the army, broadcasters, journalists, doctors, health service administrators, inspectors and others. The danger of this is that (unelected) experts, technocrats, judges and civil servants will be invested with more authority: is this an inevitable consequence of public services failing to deliver?
An interview conducted last year by Professor Humphrey Hodgson, editor of Clinical Medicine, with Professor John Caldwell, chair of the Mid Staffordshire NHS Trust during the immediate aftermath of the Francis Inquiry, suggests otherwise.1 Indeed, a novel concept raised by Professor Caldwell in that interview is the idea that the governance processes of the Trust were, if anything, over-engineered. His reasonable view is that as long as adequate mechanisms are in place to ensure a wide range of transparent performance indicators (generated both locally and nationally) are available to leaders and users of a service, we should be satisfied. The overlap between financial considerations and governance was also touched upon in the interview, although the precise relationship between Monitor (the regulator of Foundation Trusts) and the CQC remains obscure to your editor; this was an issue raised in the Francis Report, and his recommendation to merge the two bodies was not taken up by the government.
To explore these and other related themes further, we have asked leaders of the national regulatory bodies to write for the FHJ, with particular reference to their views on the FHC report and its aims. Some readers might be surprised (even alarmed) to see the General Medical Council (GMC) amongst the regulators – but there is no doubt that the GMC regards this as one of its central roles.
Where does that leave the medical profession(s)? Possibly -positioned at one corner of a ‘triangle of healthcare leadership’ (Fig 1). At another corner are the regulatory bodies, although how they interact with each other, and are themselves regulated, remains obscure. At the third corner sit the politicians.
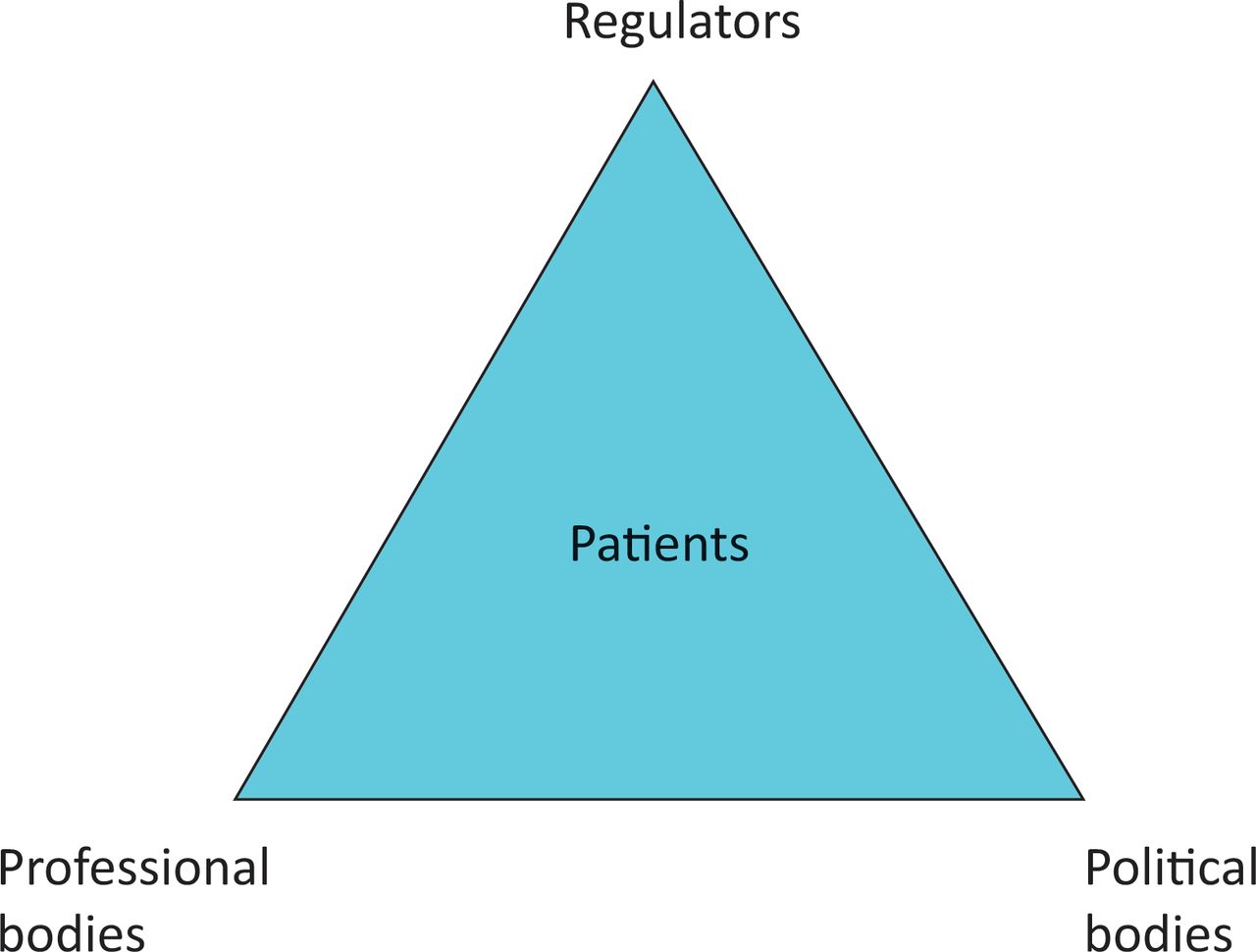
The triangle of healthcare leadership.
Responsibility for the NHS is becoming increasingly depoliticised, and devolved more and more to the (willing or unwilling) professionals who actually run it. This is an excellent state of affairs; local ownership of healthcare systems – and democratic accountability to the populations they serve – is a bedrock of the recommendations that emerged from the FHC. However, professional bodies such as royal colleges and faculties must present the agreed optimal clinical standards required for running services for scrutiny and adoption; the clinical standards that are central to establishing the best means by which health services are run, and the standards to which they must be held accountable.
At the centre of this triangle must be our patients. How they access the services provided, interpret the standards developed by the professionals, and, above all, engage with and improve those services (partly through the inspectors and regulators, if not politicians) when they fall short, is really what the FHC is all about.
Readers may feel that their editor has waxed lyrical (or otherwise) about issues that fall outwith his remit, or that he spends too much time reading on the Underground. Either way, many would share his view that for the first 60 years of its existence, the NHS has been a political football. The advent of the Health and Social Care Act (2013) may paradoxically have changed this, for better or worse. We may be moving from the NHS – about which we might feel warm and cosy (but our patients increasingly do not) – to an NHS. This extremely important distinction will see the triangle change continuously from equilateral, to isosceles, to irregular. This will change the distance and amicability of the relationship between the corners, but must not be allowed to distance the professionals from the patients for whom they care; this relationship must remain close, responsive, attentive and mutually respectful.
A last word: the difference between young and established democracies is arguably centred on the integrity and credibility of their institutions.2 Those sitting at the ‘third corner’ – royal colleges and faculties – may gain some satisfaction from this assertion, if only by virtue of their longevity. However, distinguished histories and attractive premises are not enough to guarantee that we, and others, can hold the balance of power between politics and regulation. Effective leadership, full engagement of our membership and the trust of our patients are required for that.
- © 2014 Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.