
ABSTRACT
Electronic handover tools have been advocated as a potential strategy to improve the quality of handover, especially during on-call periods at night and weekends. We aimed to quantify, categorise and explore the temporal relationship of handover tasks stored on an electronic handover system (eHandover) in an acute UK hospital trust in which the day-time primary team worked only weekdays, with only the day-time and night-time on-call teams being available at weekends. Second, we evaluated whether tasks that remained in the eHandover system throughout several shifts were likely to be completed. We defined the shift gap as the number of clinical shifts that passed between the creation of the handover task and its completion. 11,071 electronic handover parcels created on eHandover between March 2010 and January 2011 were analysed. More handovers were requested for completion on weekends (70 parcels a day) than on routine weekdays (22 parcels a day; p<0.001). The receiving teams reported that 89.4% (9,900) of the handover parcels were completed. Greater amounts of handover work was requested over weekends, when tasks were often transferred across many clinical shifts. Despite this, task-completion rates on eHandover remained consistently high. The use of a well-designed electronic handover system as part of a systematic intervention, in combination with organised verbal handover meetings, can help to reduce the risk of communication failure across shifts.
Introduction
The structure of the modern NHS is changing rapidly.1 There is a drive for hospitals to provide uniformly high quality care 24 hours a day, seven days a week. In reality, though, an eight-hours-a-day, five-days-a-week working culture for primary day teams is still engrained in most hospitals.2 Data show increased patient mortality at weekends,3 which is associated with a well-recognised reduction in the number of healthcare staff and specialised diagnostic services that are available. Primary day teams who are responsible for patient care during the working week are not present to deliver continuity of care at the weekend. Fragmentation of shift patterns following the European Working Time Directive,4 as well as trends towards specialisation and multidisciplinary team working, have created a system in which the clinical care of patients must be handed-over between healthcare professionals on a regular basis.5
Electronic handover tools have been advocated as a potential strategy for enhancing the quality of medical handover during these ‘at risk’ periods.6,7 Medical handover is defined as the process by which responsibility for immediate ongoing care is transferred between healthcare professionals.8 Both the Royal Colleges9–11 and the Medical Associations2,12 state that medical handover is a priority task for healthcare professionals. Since 2010, an electronic handover system (eHandover; Ascribe Ltd, www.ascribe.com) for medical patients has been used at Barking, Havering and Redbridge University Hospitals NHS Trust (BHRUT). The system provides a full electronic audit trail by capturing key information, including time of handover task request, task details and when task completion is expected.
Aims and objectives
The eHandover system provides the opportunity to analyse a number of key outcomes in relation to medical handover. The aims of this study were, therefore: first, to quantify, categorise, and analyse the nature of tasks handed over to on-call teams on the eHandover system; second, to investigate the temporal relationship of handover tasks across clinical shifts on weekdays and weekends; third, to study whether handovers moved across multiple clinical shifts are completed by the receiving team; and finally, to discuss the implications of the handover data in relation to seven-day working.
Method
Trust demographics and staffing for general medical patients
BHRUT provides medical services for a population of approximately 750,000 people across two acute sites: the Queen's (QH, 1,100 beds, 360 general medical beds) and King George (KGH, 540 beds, 210 general medical beds) hospitals. Staffing levels for in-patient medical wards during weekday and weekend shifts were obtained from medical staffing records for 2010 and 2011 for both hospitals.
Description of clinical handover shifts for medical patients at BHRUT
During a routine weekday, three main clinical shift patterns operate in acute and general medicine at BHRUT: the day-time primary team shift (09.00–17.00 hours, Monday to Friday only), the daytime on-call team (08.00–21.00 hours) and the night-time on-call team (20.00–09.00 hours). Weekends and national holidays are covered by only two of the major shifts, the daytime on-call and the night time on-call teams. This is a common shift pattern seen in acute trusts across the UK.
Three handover meetings take place during routine weekdays (08.45, 16.15 and 20.00 hours); two meetings per day are held at weekends or national holidays (08.45 and 20.00 hours). Handover meetings were mapped to coincide with times of clinical shift change at the Trust.
eHandover
The eHandover system was introduced at BHRUT in 2011 as part of a quality-improvement programme to assist with handover communication and completion. eHandover was made available through the Trust's intranet site to all doctors involved in the acute medical take and in-patient care. Confidentiality was ensured by password-protected access. The system managed all acute admission patient lists, in-patient lists and handover patient lists.
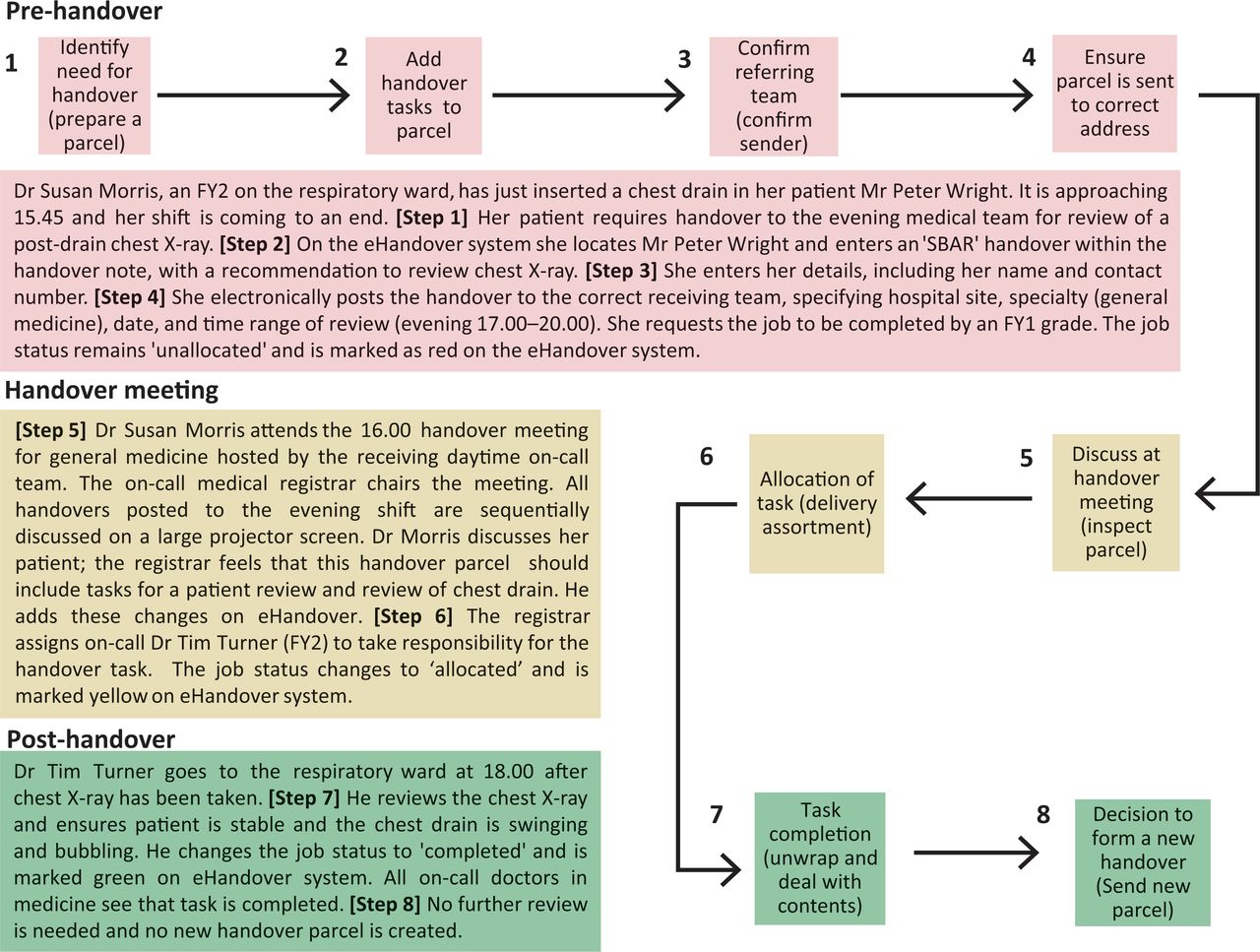
The solution uses a colour-coded traffic-light system consisting of an eight-step process akin to posting a parcel. These steps are grouped into pre-handover (steps 1–4, red), handover discussion or meeting (steps 5–6, yellow), and post-handover (steps 7–8, green). A fully worked example of how eHandover operates in clinical practice is shown in Fig 1. Briefly, the referring clinician would select a patient for handover and create a patient-specific handover parcel containing tasks that must be completed. A handover discussion would take place between the referring team and the designated receiving team in a scheduled handover meeting. After the meeting, the assigned clinician would complete the handover tasks found within the parcel. The referring clinician can set a number of different clinical handover tasks within each electronic handover parcel for future completion. For example, in Fig 1, three different tasks were set within the parcel; i) clinically review the patient; ii) check the drain is working; and iii) review the post-drain chest X-ray.
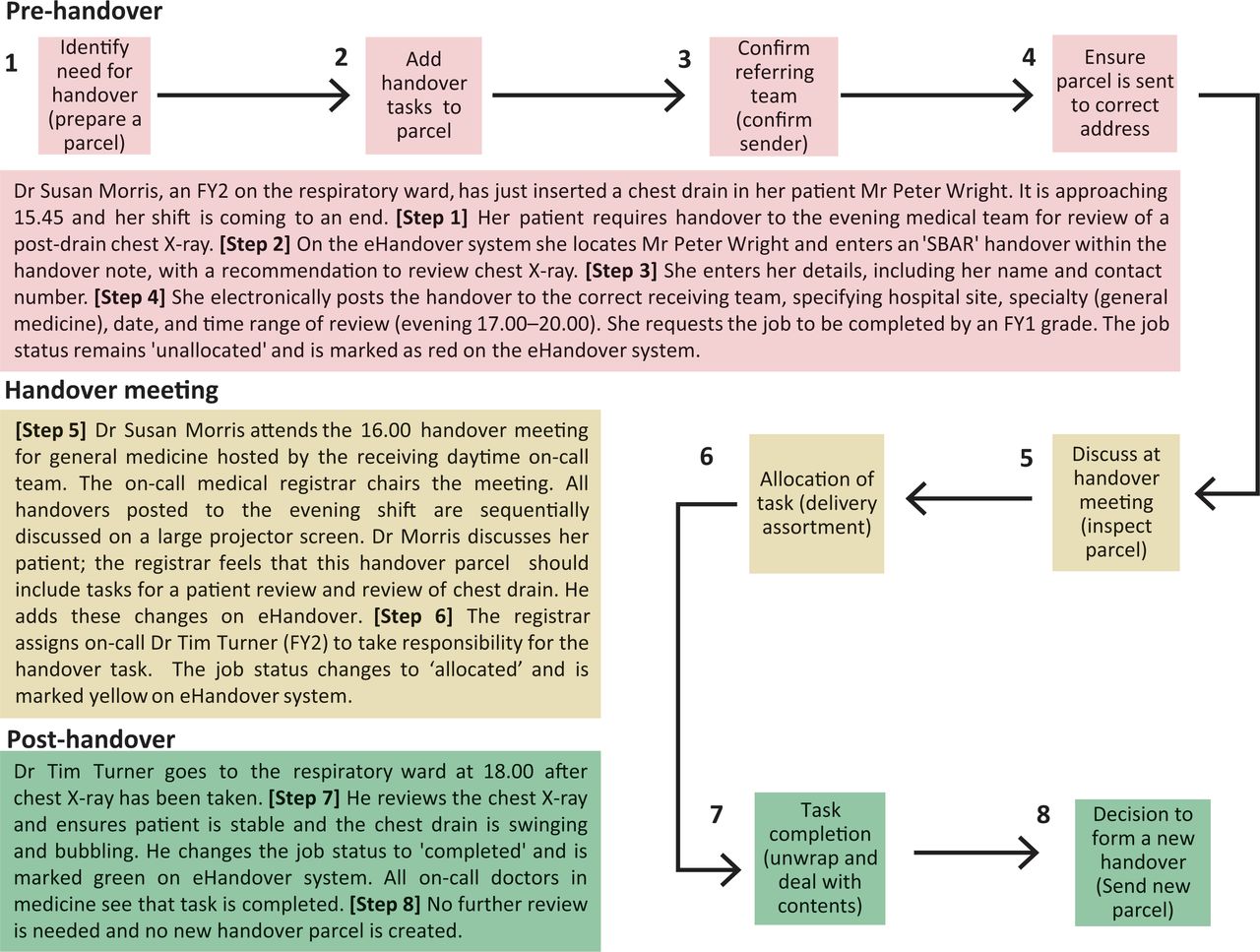
The process of information transfer by eHandover is akin to posting a parcel.
Analysis of handover parcels and tasks
The handed-over data were captured on eHandover between 15 March 2010 and 3 January 2011 (QH, 202 weekdays and 42 weekends; KGH, 136 weekdays and 28 weekends).
Each handover parcel record was examined for tasks contained within. A handover task is analogous in part to the ‘Recommendation’ component of the SBAR handover model.13 We interrogated the electronic data fields linked with ‘R – Recommendation’ (Table 1). Most handover tasks were identified from the ‘Handover note and progress’ data field. Handover tasks were itemised and categorised according to defined clinical activities. Patient reviews were identified from the ‘Clinical priority code field’ attached to each parcel.
Handover parcels: field completion rates and errors
Defining and calculating the shift gap
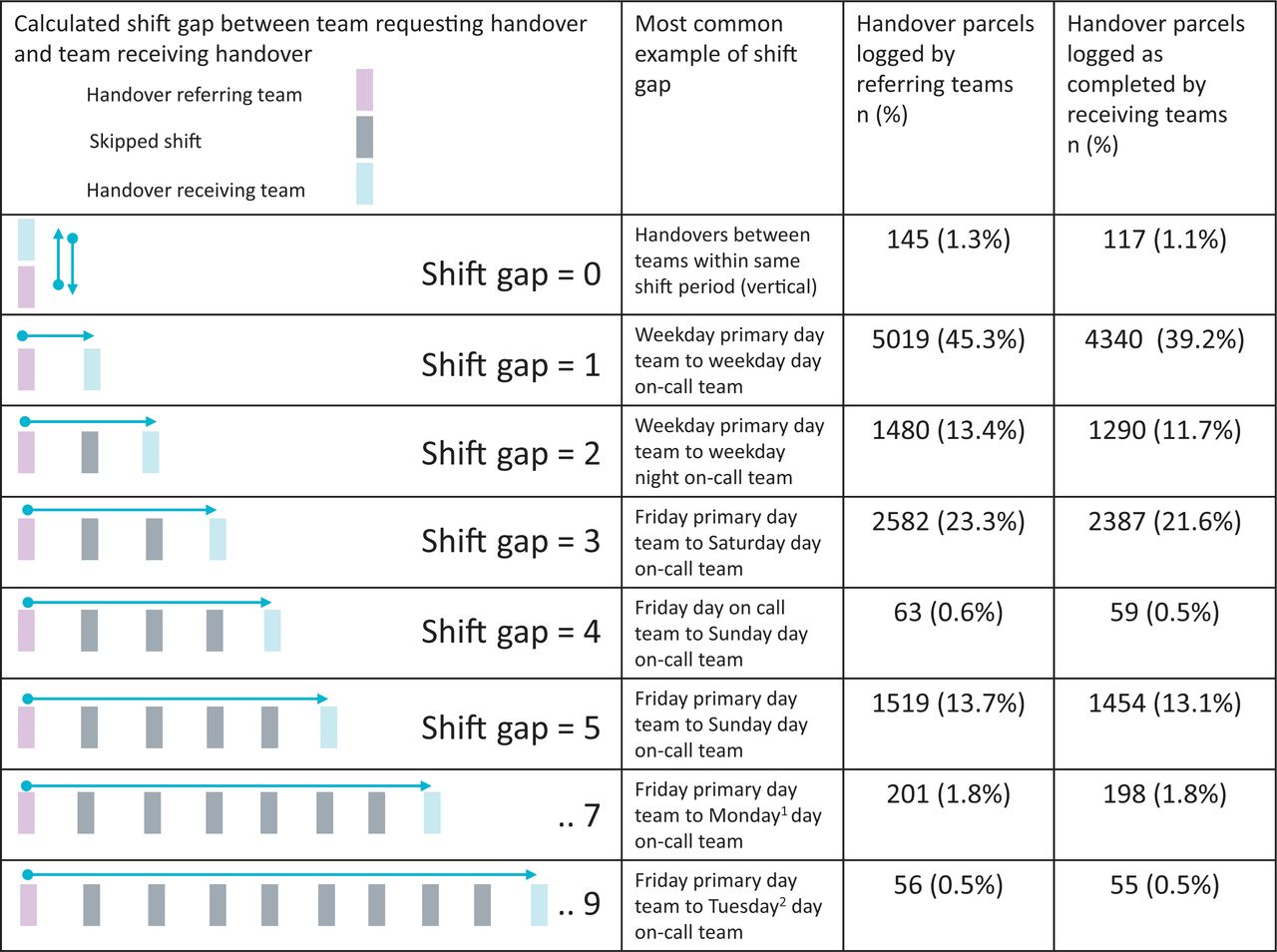
The e-Handover system has a full audit – trail and automatically records the exact date and time when a new handover parcel is added. The referring clinician enters a future date and time range specifying a shift during which they expect the accepting clinician to complete the handover task(s). We defined the ‘shift gap’ as the number of clinical shifts bridged between the team that created the handover task and the team that completed the handover task. For example, a shift gap of one is a handover that is requested for completion by the next clinical shift. In this case, the referring and receiving teams are able to meet to discuss the handover during an overlap period; but when there are shift gaps of two or more, the recipient for the handover task is not part of the next immediate shift.
We mapped all expected shifts for handover creation and completion and then calculated the shift gap for each parcel in the study.
Statistical analysis of self-reported completion rates of handover parcels
On creation of a handover parcel, the job status field in eHandover defaults to ‘not allocated’. On acceptance of a handover parcel, the receiving clinician changes the job status field to ‘allocated’. Finally, on completion of the handover tasks, the receiving clinician changes the job status field again to ‘completed’. We compared all self-reported completion categories against the expected shift gap for that parcel using the Kruskal-Wallis test. Further comparison of shift gap and self-reported ‘completion’ against ‘non-completion’ were assessed with the Chi-squared test, with the null hypothesis that non-completion is greater as the shift gap increases. The Mann-Whitney U test was used to determine statistical differences between mean weekday and mean weekend handover parcel frequency.
The data presented are means (SDs) unless otherwise stated. All statistical tests were performed on SPSS version 19.
Results
Medical staffing across shifts
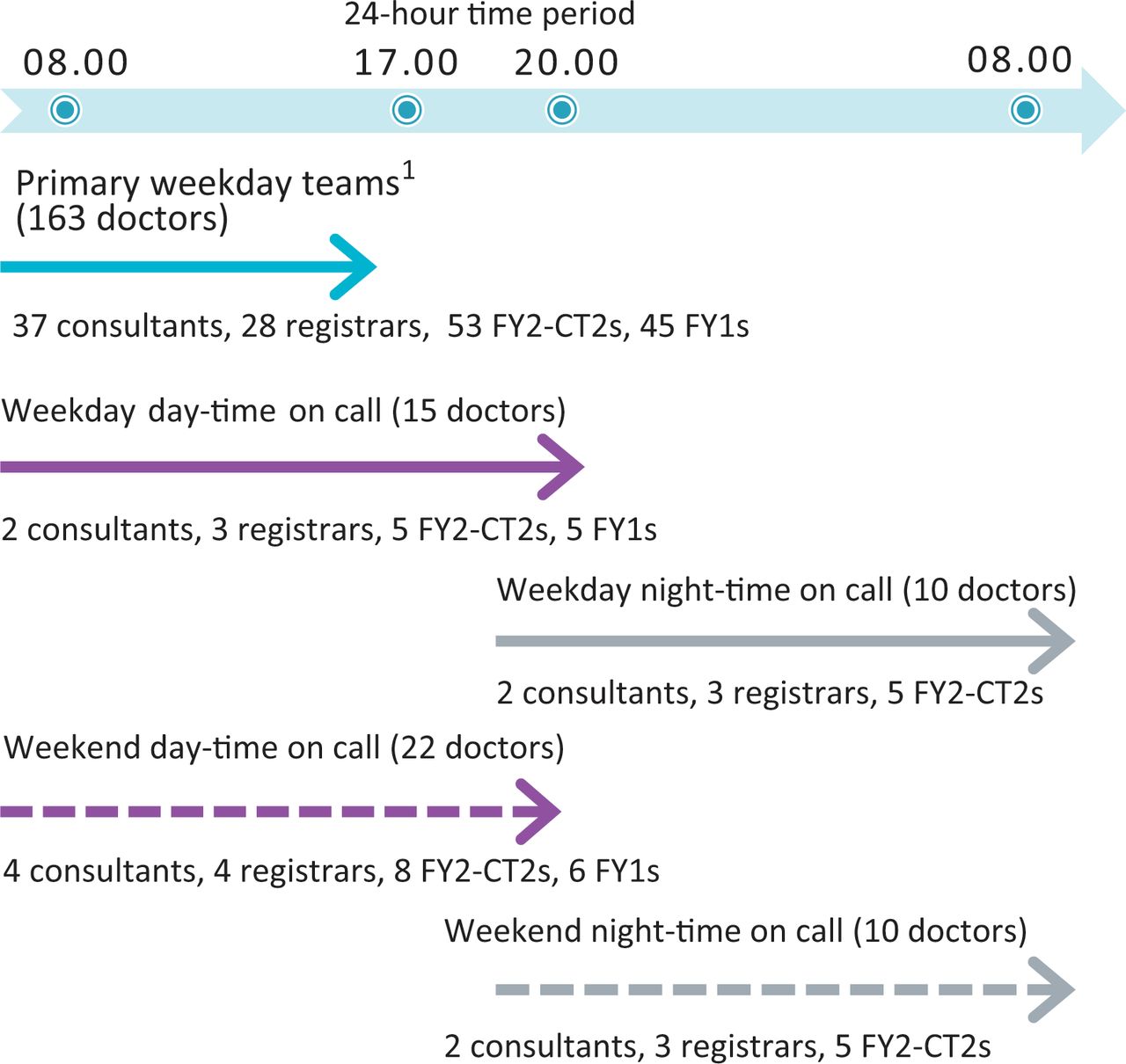
Fig 2 displays medical doctor staffing levels for acute and general medicine across both hospitals during the study period. On weekday evenings after 17.00, the medical workforce dropped from 163 doctors down to 15 doctors. Overnight after 2100, this dropped further to 10 doctors. The consultants were non-resident overnight. Weekend day-time cover was also limited with 22 doctors on duty for acute and general medicine.

Staffing levels for in-patient medical patients during major shift periods across both acute sites (Queen's Hospital and King George Hospital). 1Primary weekday teams are Monday to Friday teams that -manage medical in-patients and that work 09.00–17.00.
Quality of user entry data on eHandover
A total of 275 clinicians used eHandover during the study period, registering 11,285 handover parcels on the eHandover system by 3 January 2011. A small number (n = 214, 1.9%) were excluded from the study, mainly because of duplication of handover parcels by referring team and/or errors regarding handover date allocation.
The remaining 11,071 handover parcels were valid for analysis. The data entry quality was high for available fields on eHandover, but the user failed to record the routine day-time management plan onto eHandover in 32% of cases. The ceiling of care was unrecorded in 50.2% of all patients. In 28% of handover parcels, the eHandover system could not identify which doctor had been allocated the handover task (Table 1). In all cases, however, the name of the doctor recording the completion of the task could be viewed through the automated audit trail.
The 11,071 handover parcels related to 4,771 patients; 2,527 (53%) were female and the mean age (SD) was 68.2 (20.0) years. It was common for patients to be handed over more than once to the on-call teams; 1,326 patients had three or more handover parcels created on the system during the study period.
Parcel content
Each handover parcel contained a mean (SD) of 2.2 (0.95) handover tasks. Table 2 catalogues all of the handover tasks contained within analysed parcels during the study period, the most common of which was patient review (77.8%). Checking blood results was commonly handed over to subsequent shifts (42.0% for a biochemistry urea and electrolytes review and 31.8% for full blood count review; checking troponin level was requested in 723 (6.5%) handover parcels. On 1,240 occasions (11.2% of all parcels), incoming teams were requested to perform phlebotomy. There were 580 (5.2%) requests for blood cultures and 289 (2.6%) requests for arterial blood gas analysis. Drug prescription was also a common handover task (made on 1,816 occasions, in 16.4% of all parcels) and 9.9% of handovers requested that the incoming team arrange a review by another hospital speciality.
Breakdown of handover tasks found within the 11,071 handover parcels in the study.
Comparison of weekdays and weekends
A higher proportion of handover parcels were created for completion on weekends and national holidays. A total of 4,523 (40.9%) handover parcels were assigned for completion during the weekday out-of-hours period with a median of 22 parcels a day. 5,987 (54.1%) were assigned for completion at weekends and 561 (5.0%) were requested for the eight national holidays, with a median of 70 parcels a day (p<0.001).
Shift gap analysis and self-reported completion rates
During weekdays, most handover parcels contained tasks that required action during the next immediate shift. The mean shift gap between the creating and completing teams was therefore generally close to one. At weekends and on national holidays, when the routine primary day teams were not available, the shift gap widened considerably for all tasks being handed over (Table 2).
Assigned handover parcels were separated by shift gap and are shown in Fig 3. A high proportion of handovers placed on the system were not intended for completion during the next shift (5,907 parcels, 53%). Despite this, the self-reported completion rates recorded on eHandover did not fall with the widening shift gap. The common shift gaps of three (Friday primary team to Saturday day-time on-call team) and five (Friday primary team to Sunday day-time on-call Team) achieved self-reported completion rates for assigned handovers of 92.4% and 95.7%, respectively.
Discussion
Main findings
This study has demonstrated that there is a greater than three-fold increase in handover work tasked for completion on weekends and bank holidays compared to routine weekdays. Tasks are being handed over across a gap of multiple shifts, involving periods when the medical workforce is severely reduced and the primary day team is unavailable. Despite the widening shift gap and greater load of handover work on weekends, clinicians still managed to record overall completion rates of 89.4% of handover tasks on the eHandover system.
Strengths and weaknesses
This is the first study to catalogue the quantity and nature of handover tasks posted to on-call teams in an acute UK hospital trust. The content of handover parcels was stored on permanent record with a full audit trail, allowing accurate identification of all tasks. The automated date and time stamps stored on eHandover ensured accurate mapping of expected clinical shifts and calculation of shift gap. Clinicians’ entry of handover data fields was, on the whole, very good. The recording of a routine management plan and the resuscitation decision was often omitted. This was probably because these fields were not compulsory at time of implementation. This has now been rectified.
eHandover was not designed to manage handovers created and completed between teams within the same shift (vertical handover). These were not captured on the system. Also, some handovers to the next immediate shift may not have been collected on the system. Clinical teams could have used verbal communication alone to pass on tasks. Hence, the total handover work with a shift gap of one could be underestimated in this dataset. The recording of handover tasks with a shift gap of two or more is, however, complete because verbal communication was not feasible for these tasks.
eHandover as a handover process
Electronic systems enable a systematic approach to medical handover.14–16 eHandover captures the high-risk activity of ‘horizontal handover’, when the incoming teams and outgoing teams are not resident in hospital at the same time other than for a short overlap handover period. eHandover uses an intuitive traffic light system to manage the key steps of pre-handover (red), handover (yellow) and post-handover (green) (Fig 1). The system records the clinician ownership and completion of assigned tasks, which traditional verbal or written systems struggle to do. The system encourages team-working because the handover activities for the assigned shift are visible to the whole team. The objective for the team of on-call clinicians is to complete all of the handover tasks assigned to them, turning the list ‘Green’ before the next shift.
One of the major features of eHandover is its ability to move handover work across shifts electronically without loss of data available to the oncoming shifts.17 For example, the Sunday day-time on-call team in the study received requests for handover work from at least three different previous clinical shifts (Fig 4). eHandover stores and organises the handover work from all of these previous shifts into one coherent list for the incoming team. Before eHandover implementation, some of these handovers were verbally received or handwritten on scraps of paper causing confusion in the overwhelmed Sunday teams.
The system has been used to support the training of doctors. Trainees can plan and track their admissions, patient activity, handover patient activity and non-elective procedural tasks, and can record them on the system anonymously. This allows easy recollection of tasks that have been performed, facilitating reflective practice and the creation of evidence e-portfolios. Trainees have found it easier to manage patients out of hours since the implementation of eHandover.18 User uptake and data records have certainly increased as doctors working at the Trust have become accustomed to the use of the electronic tool. The system has been recognised for its role in improving patient safety in relation to handover.19
Handover activities between weekdays and at weekends
Handover parcels varied considerably in size and nature and were rarely referred as a single task. Patient review was the most common handover task, reflecting the main concern for continuing patient care when doctors leave their shift. A large amount of blood work was handed over, both checking of results and taking blood. Fluid and drug prescription by on-call teams in a dynamic environment is a potential source of error. Decision-making may be impaired without a full understanding of patient background, comorbidities or previous monitoring of clinical progress.
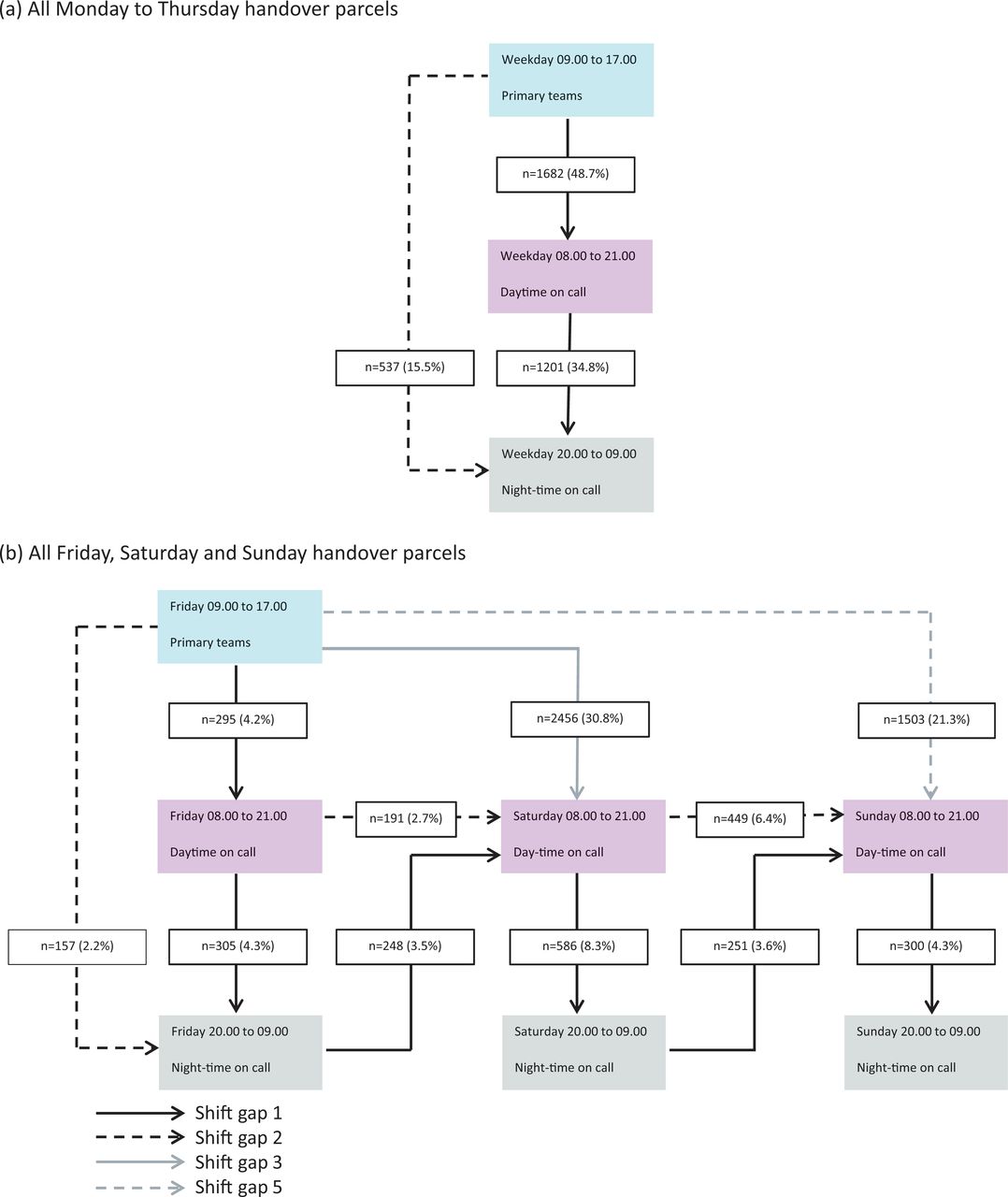
Fig 4 shows patterns of handover task assignments separated by routine weekdays and weekends. Tasks in this study were moved across many shifts before they became due for completion. On routine weekdays, a substantial handover workload was created by the primary day teams that leave the hospital at 17.00. A notable 15% of this work was, however, assigned directly to the night on-call team, bypassing the day-time on-call team. Thus, even on a weekday, some tasks were not carried out by the next shift and there were limited or no means of verbal communication with the completing teams.

Patterns of handover task -assignments separated by routine -weekdays and weekends. (a) Handover parcels for all routine workdays during study period (Monday to Thursday): based on day/night 13-hour on-call rota shifts and routine 8-hour weekday shift. The figure maps and quantifies all handover parcels for -Monday to Thursday during the study period (excludes national holidays). Most common handover patterns during routine weekdays were from primary day teams to day-time on-call teams (n = 1682, 48.7%) and day-time on-call teams to night-time on-call teams (n = 1201, 34.8%). Minor shift patterns are not displayed on figure (n = 35, 1.0%). The majority of this group consisted of -the same shift handover (shift gap = 0). (b) Handover parcels for all Fridays, Saturdays and Sundays during study period: based on day/night 13-hour on-call rotas shifts and routine 8-hour Friday weekday shift. The figure maps out and quantifies the handover parcels for common shift gaps between Friday, Saturday and Sunday. More than 50% of all handover parcels requested during the weekend period were from Friday primary day-time teams to Saturday day-time on-call teams (n = 2456, 30.8%), and Friday primary day-time teams to Sunday day-time on-call teams (n = 1503, 21.3%). -Minor shift -patterns are not displayed on figure (n = 226, 3.2%). The majority of this group consisted of within-same-shift -handover (shift gap = 0).
More handover tasks were created by the primary day teams on a Friday afternoon than at any other time. Being their patients’ regular clinicians, the doctors in these teams have a better understanding of their patients and greater ability to create handover tasks. Handover work assigned from the Friday primary teams sometimes spanned across five shifts on the weekend. As an example, non-invasive ventilation for chronic obstructive pulmonary disease (COPD) patients was reviewed over greater shift gaps on weekends than on weekdays. One can infer that level-one patients and those identified as sicker are being left without review for longer periods over the weekend than would ordinarily be the case during the week.
Approximately 33% of all handover workload tasks recorded for weekends were created after the Friday afternoon handover meeting. These handovers were mostly related to new non-elective admissions and in-patients who had recently become unwell. Tasks created on weekends moved across sequential day-time on-call shifts. During a routine weekday, handovers from one routine day shift to the next certainly did not occur because the primary day-team doctors responsible for patient care were available to review all of their patients during the next working day.
The handover completion rates self-reported by the accepting teams remained high throughout the study. Importantly, task completion rates did not fall with widening shift gaps, validating the primary function of the eHandover solution (Fig 4). Reasons for non-completion for requested tasks were mostly related to teams’ not updating handover records at the end of their shift. A smaller proportion of handover tasks were left incomplete because the clinician was unable to finish the task during his or her shift. Either these handover tasks were electronically moved on to the next shift or a clinical decision was made not to complete the task.
What improvements in clinical care have been made?
Having identified some specific clinical safety issues, potential solutions for improving care quality have been generated in the Trust. In 2013, we began a phased introduction of seven-day working. There is now seven-day on-site consultant cover for gastroenterology, respiratory medicine, care of the elderly, cardiology and acute medicine, broadening the wards that deliver continuity of care. The overall number of doctors working on weekend days has increased from 22 doctors in 2011 to 30 doctors this year. There are plans to implement enhanced therapies and pharmacy support for weekends in the near future.
In the study, 4.5% of all assigned tasks were related to discussing and chasing the results of CT and MRI scans with radiologists. An immediate overnight radiology reporting service for all CT-scan requests across seven days has been implemented. Phlebotomy jobs are frequently handed-over, identifying the need for further phlebotomy support in the hospital. This has now been established on a number of key wards, including the acute medical unit.
The Friday handover meeting will remain pivotal for patient safety at weekends unless full seven-day working is realised. The data confirm the large quantity of handover tasks being posted by the Friday teams for the weekend. These meetings can therefore last up to two hours. Teams have to be released from their duties to go through their requests for weekend handover tasks systematically at the meeting. The receiving teams for Friday, Saturday and Sunday also need to be in attendance to discuss and pre-empt anticipated issues. In the Trust, these meetings are always consultant- or registrar-led. Previously, the quality of handovers has been shown to improve when patients are discussed in handover meetings.20
Summary
Best practice involves doctors’ seeing all of the patients under their care every day. On weekends, this would be near impossible for general medical patients at the Trust. This study showed a three-fold increase in planned handover work, together with an eight-fold decrease in doctors, during weekends and national holidays. Hence, only a selected number of patients are handed over on weekends, with the sickest being prioritised. The remainder of the patients, although visible on the system to the on-call weekend and night teams, were not routinely seen. These patients may not move through their patient pathway as efficiently as those placed on the handover list. This lack of continuity of care is a major failing of five-day working systems and a risk to patient safety.
Medical handover is much more effective when using electronic handover systems in conjunction with verbal handover. This study has shown high self-reported completion rates for handover work that is moved across clinical shifts. The data have highlighted the large handover workload being posted to overstretched weekday and weekend on-call teams. Handovers will never be a risk-free activity in the acute hospital setting.21–23 Nevertheless, auditable electronic handover data can be used to plan service improvements that can help to reduce this workload. n
Statement of interest
Data collected in this research was obtained from an electronic handover system (eHandover). Barking Havering and Redbridge University Trust are the proprietors of eHandover. The system has been licenced to Ascribe Ltd for sale. Ascribe Ltd are solely responsible for sales. A proportion of any royalties from any external sales are returned to BHRUT and two clinicians who are creators of the system, one of whom is the primary author of this paper.
- © 2014 Royal College of Physicians
References








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.