
ABSTRACT
Background Outside critical care environments, few studies have assessed the significance of oliguric acute kidney injury (AKI). This study investigated the feasibility of an electronic fluid balance chart to diagnose oliguric AKI. Data were used to determine if oliguric AKI was met earlier than creatinine AKI and to establish outcomes of those who developed AKI.
Methods A single-centre prospective cohort study investigated Kidney Disease Improving Global Outcomes oliguric and creatinine AKI criteria on general surgical wards.
Results 2,149 cases were included in the analysis. Incidence of oliguric AKI was significantly higher than creatinine criteria (73 versus 10.1%) and detection occurred earlier (2.1 versus 6.1 days, p<0.05). In cases with oliguric AKI, 8.1% also developed AKI by creatinine criteria. In cases not meeting oliguric AKI criteria, fewer cases developed creatinine AKI, as compared to those meeting oliguric AKI criteria (7.9% versus 11%, p=0.043). There was a high incidence of missing data.
Conclusions Oliguric AKI was met in a high proportion of cases and occurred earlier than by changes in creatinine. Barriers to consistency of recording must be addressed before oliguric criteria could be implemented in clinical practice.
Introduction
Acute kidney injury (AKI) affects at least 10% of hospital admissions, with over half a million episodes in the UK annually.1 It is associated with increased short- and long-term mortality, prolonged hospital stays, costs (at least £1 billion annually in the NHS),2 and increased requirements for kidney replacement therapy (KRT), critical care and de novo chronic kidney disease (CKD).3,4 Reports of deficits in recognition and management,5 alongside the absence of specific therapies for AKI, have driven interest in strategies to improve the delivery of basic elements of AKI care, including detection and monitoring.
Background
In 2014, NHS England mandated hospitals to alert to AKI using creatinine criteria.6 However, using changes in creatinine has shortcomings, being affected by baseline, delays to increase and under-representation of severity, making it an imperfect gold standard.7,8 The second criteria used by Kidney Disease Improving Global Outcomes (KDIGO), oliguria, can detect AKI earlier6,7,9 and could be the only indication of kidney dysfunction. However, there has been limited clinical implementation of alerting to oliguria, with few studies outside critical care.10 Explanations include difficulties in interpretation. For example, postoperatively, oliguria can be physiological or a result of diuretic medication. In addition, practicalities of ward-level, largely paper-based, urine output monitoring are challenging,11–14 particularly without catheterisation, precluding large data studies and alerting implementation. Previous studies reported a higher incidence of oliguric AKI (28–52%) than of creatinine increase (14–24%).15–18 In cases with oliguric AKI, a high percentage of cases also had creatinine-based AKI.17,19 Even in the absence of a creatinine rise, oliguric AKI is associated with increased use of KRT, hospital stay and mortality.7,15,17,20–22 However, KDIGO oliguria criteria are based on consensus opinion informed by predominantly critical care studies. This leaves key research questions: (1) what are the threshold and duration of oliguria that predict AKI by creatinine criteria, requirement for KRT, mortality, hospital stay and new or worsening CKD?; (2) does oliguria detect AKI earlier compared with creatinine change?; and (3) are results from critical care research transferrable to a hospital ward setting?
Objectives
This study investigated urine output recorded on an electronic fluid balance chart to establish:
Are AKI stage 1 by urine output criteria met before creatinine changes in adults on hospital surgical wards?
Are AKI stage 1 by urine output criteria associated with poorer outcomes for patients?
What is the quality of urine output measurements in a ward-based setting?
Methods
Study design
A prospective, single-centre, observational cohort study was performed with anonymous analysis of routinely collected clinical data from electronic patient records (EPR).
Setting
Participants were included following admission to an 870-bed general hospital in south-east England with an annual emergency department attendance of over 40,000. Surgery includes general surgery, urology, and trauma and orthopaedic, but does not include major trauma, neurosurgery, cardiac, major vascular or transplantation surgery. Day surgery and obstetric patients were excluded. Data were captured for 12 months (2018).
Participants
Data from four adult (≥18 years) surgical wards were collected during the first 7 days of hospital admission.
Variables
Primary outcome measures included AKI incidence (oliguric and/or creatinine), time (days) to AKI detection, and mortality, alongside frequency of output measurements. AKI detection was measured as:
Oliguric AKI: outputs were recorded during routine care on a digital fluid chart (Fig 1) from Time 0 (first entry) and subsequent 12-h consecutive blocks (Table 1). Oliguric AKI was defined as urine output <0.5 mL/kg for 12 h, in line with KDIGO AKI stage 1 by urine output criteria.
Creatinine AKI: creatinine measurements were collected routinely according to clinical care during the first 7 days of hospital stay and a diagnosis of AKI was made according to KDIGO criteria: either an increase ≥26.5 μmol/L in <48 h or an increase >1.5 times baseline within 7 days.23
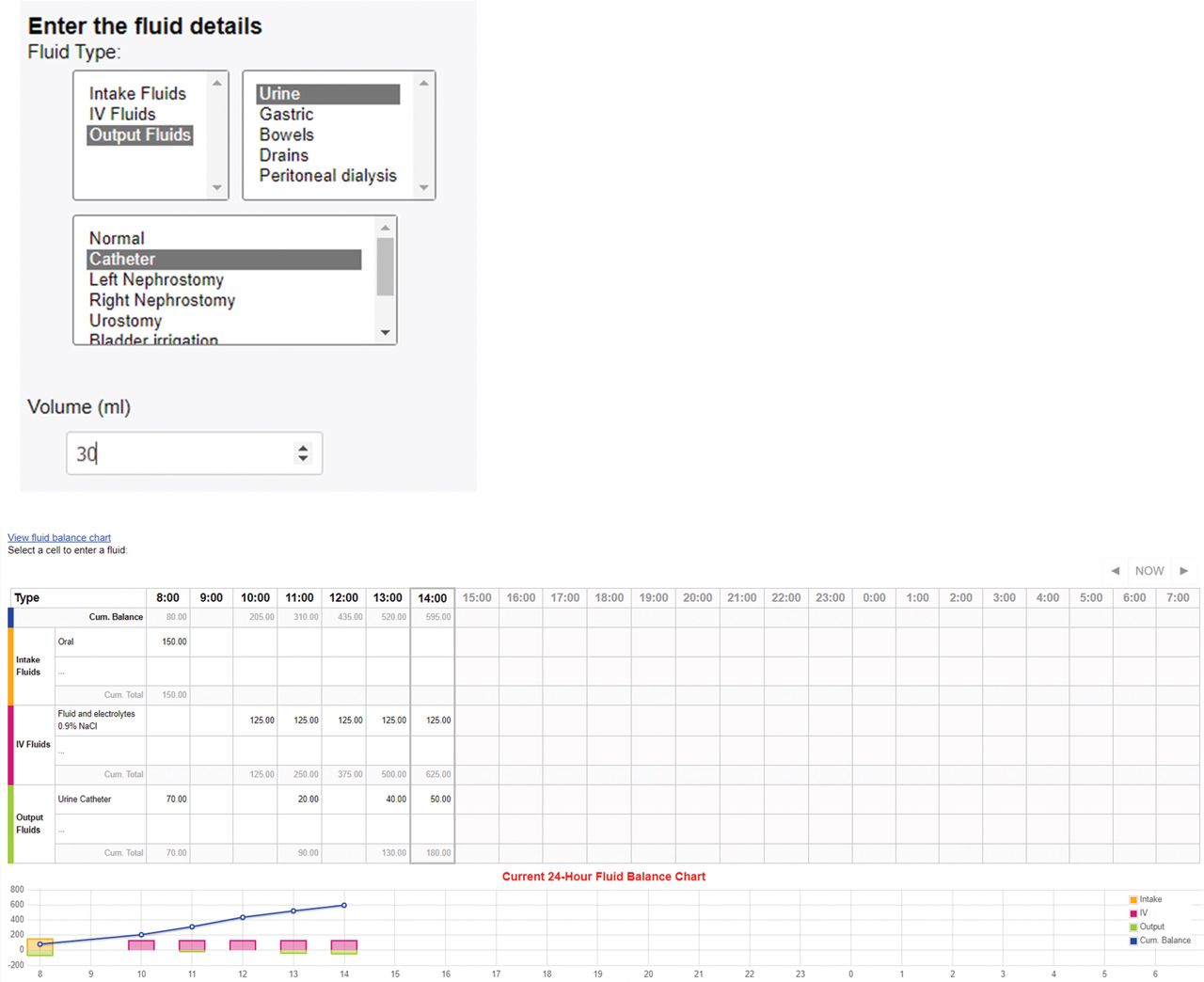
Example of the electronic fluid balance showing data entry including input and output fluids.
Example of how oliguric acute kidney injury was detected from digital fluid charts
Data sources
Baseline data were collected from the hospital EPR, including age, gender, weight, admission and discharge date, whether surgery was performed, presence of a urinary catheter, duration of hospital stay, admission to critical care and in-hospital mortality (Table 2). To establish multiple health conditions, electronically coded histories (diabetes mellitus and congestive cardiac failure (CCF)) were retrieved using the International Statistical Classification of Diseases 10th (ICD-10) and CKD was defined as an estimated glomerular filtration rate (eGFR) <60 mL/min before admission (in those with an available baseline creatinine). Data were transferred to a research database and anonymised before analysis.
Demographics for all cases in the study
Bias
The study gathered routinely collected clinical data over a 1-year period. Data were extracted from EPR by the Information Technology team based on the eligibility criteria provided by the Principal Investigator (PI). Requirements set out by the local research and development department of the hospital trust were followed for accessing, sharing and the anonymous analysis of routinely collected data. This provided an extra layer of assurance that the data were not manipulated or changed, and without introducing bias from the PI to ensure validity of the data. The project was approved by the ethics committee at the University of Southampton. Healthcare staff were unaware that the data were being investigated.
Study size
In this exploratory study, a formal sample size was not determined by a power analysis. The analysis included cases if they met the following criteria:
urine output measurements recorded on an electronic fluid chart
weight recorded
absence of community-acquired AKI and
at least one repeat creatinine measurement during admission.
From 4,200 cases, 2,051 cases were excluded because of no output entries (n=1240), no weight (n=233), community-AKI (n=164) and/or no repeat creatinine measured (n=414), leaving 2,149 cases for analysis. Eligible patients were followed up until discharge from hospital, or death, during the inpatient spell.
Quantitative variables
The primary outcome measures in this study included AKI incidence (oliguric and/or creatinine), time (days) to AKI detection, hospital mortality and frequency of urine output measurements.
Statistical methods
Statistical analyses were performed using SPSS V.25. Continuous, normally distributed variables were expressed as mean±standard deviation (SD) and nonparametric variables were expressed as median and interquartile range (IQR). Tukey's Honestly Significant Difference (HSD) test was used to report differences between sample means for significance. Categorical variables were expressed as absolute (n) and relative (%) frequency. Data were analysed using each definition of AKI with parametric and nonparametric tests, as appropriate. Differences were significant at p<0.05.
Results
Participants
From 2,149 cases, 48.5% (n=1043) were male, median age was 71 years (IQR 55–82), median hospital stay was 7.8 days (IQR 3.3–15.9), in-hospital mortality was 3.3% (n=70), and 31.9% (n=685) underwent a surgical intervention. Diabetes was present in 8.1% of cases (n=174), 26.5% of cases (n=569) had CKD and 4.2% of cases (n=91) had CCF. Baseline creatinine was available in 83% of cases (n=1783) (Table 2).
Descriptive data
The mean number of urine output entries entered over the 7-day study period was 21.7 (SD 29), with a median of 10 (IQR 4–28) entries. Missing data were frequent: 50.2% (n=1078) had eight or fewer entries in total, and 10.2% (n=220) had only a single output entered. Those with a urinary catheter (53.3%) had a similar number of entries to those without a catheter.
Outcome data
AKI incidence
The incidence of AKI by creatinine criteria occurred in 10.1% of cases (n=218), whereas AKI by oliguric criteria was met in 73.0% (n=1568) of the cohort. Of cases with oliguric AKI, 8.1% (n=172) also developed creatinine AKI (Table 3). In cases that did not develop oliguric AKI (n=581), 7.9% (n=46) went on to develop creatinine AKI, whereas, in those with oliguric AKI (n=1568), 11% (n=172) met criteria for creatinine AKI (p=0.043).
Cases with acute kidney injury, time to acute kidney injury detection and mortality between the study groups
Time to AKI detection
AKI oliguric criteria occurred earlier than creatinine AKI by 2.05 versus 6.1 days, respectively (ANOVA (F(2,1956)=113,30, p<0.05) (Table 3). Tukey's HSD was used to determine the nature of the differences between the three groups (oliguric AKI versus creatinine AKI versus both). This analysis revealed that those with oliguric AKI were diagnosed sooner than were those with creatinine AKI. Those with both oliguric and creatinine AKI were diagnosed sooner than those with creatinine AKI alone.
In the 172 cases meeting both oliguric and creatinine AKI criteria, 82.7% (n=143) met oliguric AKI criteria before creatinine AKI. Oliguric AKI occurred before creatinine AKI by 1.6 versus 6.1 days, respectively (p<0.0001) (Table 4).
Results for 172 cases meeting both oliguric and creatinine criteria, looking specifically at time to detection for each acute kidney injury criterion
Discussion
Key results
To our knowledge, this is the first study to assess oliguria prospectively to define AKI in a general hospital population using a digital fluid balance chart. Data from a full year provided a realistic picture of care on general surgical wards, considering fluctuations in healthcare, such as winter pressures, staff sickness and staff shortages. Previous studies, generally with small sample sizes, all in higher care settings, found that oliguria detected AKI earlier than did changes in creatinine.15,18,19 Oliguric AKI was met with a higher incidence compared with creatinine AKI, as previously discussed. Regardless of AKI criteria investigated in previous studies, incidence of oliguric AKI was always higher than creatinine-based AKI, with poorer patient outcomes seen in patients with oliguric AKI, even in the absence of creatinine AKI.17,19,20 The latter findings are not entirely concordant with the current study, although they could be explained by the large amount of missing data captured, resulting in a high incidence of oliguric AKI. This high incidence appears implausible, given that only a few cases with oliguric AKI had worse outcomes. These findings highlight the need for improvements in urine output monitoring on hospital wards; to this end, digital innovations that allow automated urine flow monitoring are being investigated. If these innovations prove effective, they could be used to identify AKI early, with alerts to clinical staff of patients with oliguric episodes. Given the well-described delays and difficulties in interpreting creatinine in patients who are acutely unwell, these innovations could improve early AKI recognition and subsequent management. The number of deaths in the current study was also low, precluding firm conclusions from being drawn.
Interrogation of the data collected in this study suggested that electronic capture potentially overdiagnosed oliguric AKI, because of missing data from sporadic entries by the clinical team. Half of the cases had eight or fewer entries and one in 10 only had a single entry, despite expectations that the investigated cohort would have more frequent monitoring because of their acuity and perioperative setting, and that charts had been started by the clinical team. Over half the cases had a catheter facilitating frequent monitoring, yet the number of entries were no different in this group. One explanation might be that the patients' status had quickly improved, resulting in a decision not to frequently record outputs.
Reliability of urine output data was also questioned, because volumes frequently appeared inaccurate. Timings of 12-h blocks were calculated from the point of first entry and, as a result, influencing factors, such as staff shift changes, might have affected the accuracy. Although not identified in these studies as a reason for poor compliance, staffing issues in ward areas might also contribute. Results from a study in a critical care area18 showed that 27% of output data was missing, thus highlighting the added difficulties in ward areas with fewer staff. The apparent lack of monitoring has been highlighted in multiple reports and is concerning because fluid assessment is a fundamental element of good patient care.5,24 Unfortunately, neither report produced recommendations specifically for improving fluid balance charting and, from this current study, it would appear that improvement is required. In several studies that investigated fluid balance charting, reasons for poor compliance were identified as a lack of standard training and clear guidance, with a lack of knowledge leading to a failure to recognise its importance.11,12,25
Other possible explanations for the high incidence of oliguric AKI in this study might be because of the AKI criteria investigated. This was investigated in line with Stage 1 KDIGO criteria for AKI and because urine output monitoring at least every 6–12 h was felt to be a suitable level of monitoring in patients on surgical wards. Previous studies investigating oliguric AKI used various criteria for detection, making reliable comparisons difficult.18 Importantly, all previous studies were undertaken in higher care areas; therefore, AKI incidence is likely to have been higher compared with a hospital ward population.26
To establish whether cases met criteria for creatinine AKI, information regarding prior kidney function was needed to establish a baseline. Baseline creatinine measurements were derived from previous results and, in some cases, might have been measured several months previously, thus making differentiation of community from hospital AKI difficult to define accurately. However, a high proportion (83%) of baseline estimation was possible.
In our study, although a minority of cases with AKI defined by oliguria progressed to develop creatinine AKI, there was an increased risk compared with no oliguria, suggesting that oliguria did represent an early sign of kidney dysfunction. In cases that did not progress to creatinine AKI, it is unclear whether true renal injury or dysfunction was present, or whether oliguria occurred for other reasons, such as part of an intact physiological response postoperatively or misdiagnosis from a lack of data collection.
Oliguric AKI criteria were met on average before creatinine AKI, findings that concord with previous research.15,18,27
Limitations
The study was undertaken in a single centre, on surgical wards, with fewer than half the cases undergoing surgery. However, it represents one of the largest data sets described to date. Neither the type of surgery nor whether surgery was for elective or emergency reasons was established, which the latter being relevant because such patients are at higher risk of AKI.28 Although output data were collected prospectively, information regarding multiple health conditions were extracted from EPRs from coding events, which might have led to an underestimation of disease prevalence.
Interpretation
This study found a high incidence of oliguric AKI using an electronic fluid balance chart in a ward setting. Oliguria can provide an early alert to patients at higher risk, including those more likely to develop AKI, defined by a rise in creatinine. More protracted oliguria was associated with increased hospital stay. The variable reliability of urine output recording prevents the drawing of robust conclusions and clinical implementation.
Generalisability
This is the first prospective study investigating oliguric AKI outside critical care. The paucity of studies outside critical care settings has previously been acknowledged. Given the availability of digital data, a large ward-based population was studied. The study highlights how digital capture can provide teams with robust data to feed back on completeness of collection or monitoring.
Quality improvement strategies could include education, refinement of digital charting and integration of clinical decision support systems. A large prospective study could investigate utility of (accurately diagnosed) oliguria as a marker of kidney dysfunction and adverse patient outcomes. Patients at higher risk of AKI (ie those with diabetes, CCF or CKD) could also be investigated, looking specifically at the incidence and outcomes of those with oliguric and creatinine AKI. If oliguria was found to be a useful predictor of adverse outcomes, an automated electronic alert could prompt staff, triggering appropriate attention and interventions, potentially optimising patient outcomes.
Finally, the use of renal biomarkers in concert with oliguria could be used to provide enhanced risk stratification. Thus, oliguria could be a prompt to perform a further biomarker test, allowing a more personalised approach.
Funding
This work was undertaken during a NIHR-funded Masters In Clinical Research awarded to the first author.
- © Royal College of Physicians 2023. All rights reserved.
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.