
ABSTRACT
The physician associate (PA) profession is relatively new to the British NHS. Little research has been conducted on the facilitators to integrating these new health professionals into a secondary care service. Thus, a grounded theory qualitative study was conducted. PAs who were educated in the UK and were the first PA in their secondary care service were interviewed, as well as doctors who were on the team when the PA started. Ten facilitators were identified, comprising three facilitator themes: PA involvement in role and skill development is crucial; having a champion for the PAs promotes integration; and principled behaviour by the PA allows the role to develop safely and effectively. Having a clearly defined role for the PA is the primary facilitating factor. This research identified approaches that both PAs and hospital trusts can implement to facilitate the introduction of PAs to secondary care services in the NHS.
Introduction
The physician associate (PA) profession was developed in the USA (where it is called the ‘Physician Assistant’ profession) during the 1960s to address a medical workforce shortage. The PA profession, although well established in the USA, is relatively new to the UK. The first British PA programmes were established during the mid-2000s and, by 2021, nearly 2500 PAs were listed on the Faculty of Physician Associates Managed Voluntary Register.1 Many newly graduated PAs enter secondary care employment either out of preference for secondary care or because they have had their education funded by hospital trusts eager for more medical providers.2 Given the youth of the profession, little is known about how PAs are integrated into medical teams in UK secondary care settings. Two pilot project evaluations were conducted during the mid-2000s, which evaluated incorporating very experienced US-trained PAs into secondary care in the UK.3,4 Both studies found that experienced US PAs were able to make a valuable contribution to the needs of secondary care services by providing safe medical care and increased continuity of care. Drennan and colleagues conducted a mixed-methods study of UK-educated PAs in the hospital setting in 2018. This study found that participants believed PAs were accepted by other members of the healthcare team, that they improved patient flow and continuity of care, and that their presence allowed for more teaching time for junior doctors.5
Our study sought to establish which factors were specific facilitators and barriers to the integration of the first UK-educated PAs in a secondary care service in the NHS. The first PA in a trust faces the challenge of both introducing a new role and becoming the exemplar for that new role. This study interviewed PAs who were the first PA on their secondary care service and doctors who worked with them, to characterise the barriers and facilitators these teams faced when recruiting a PA. In this paper, we report on the facilitators to the integration of the first PA in a clinical service.
Methods
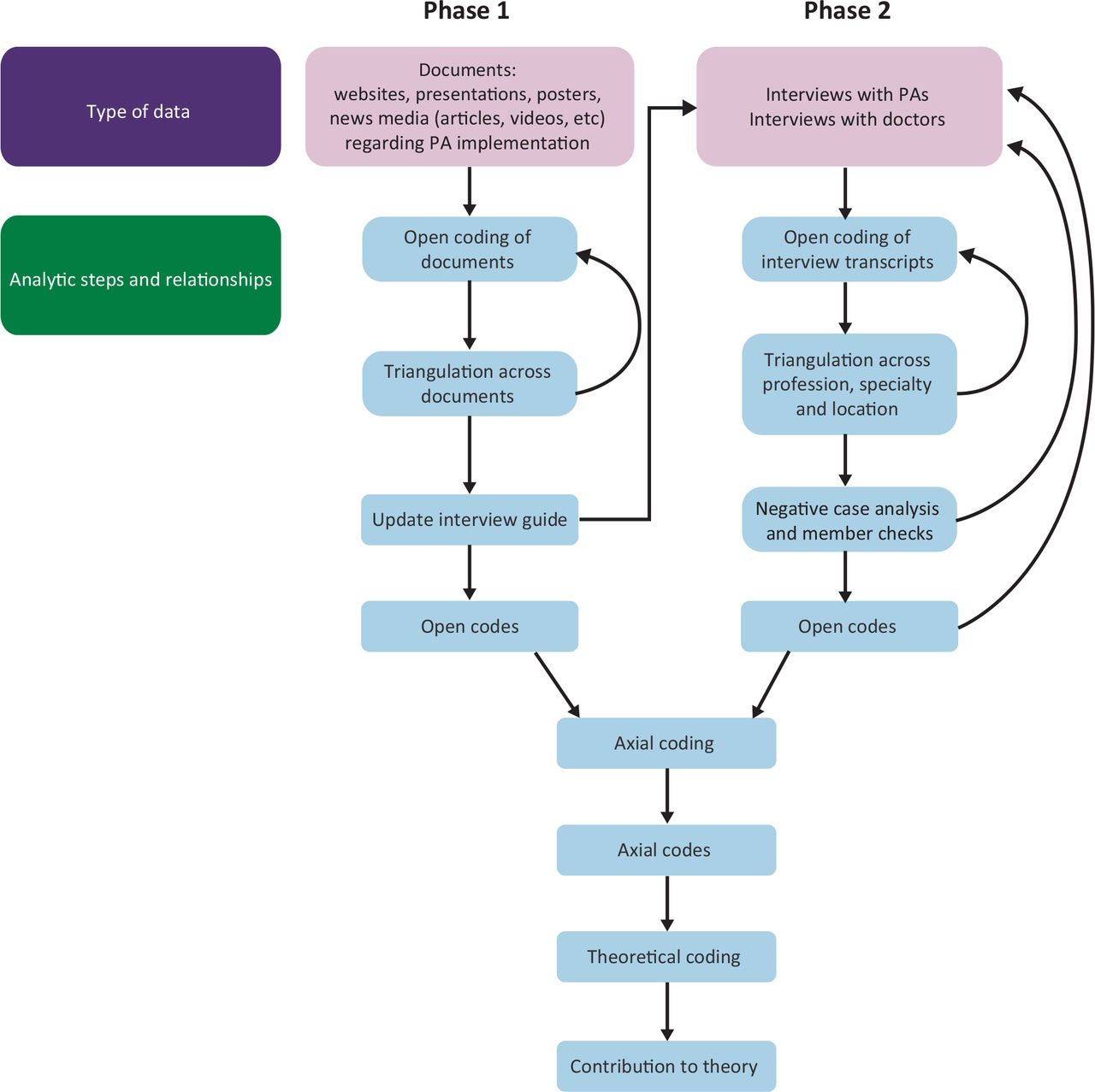
This study used a grounded theory qualitative approach to the research question, with the goal of developing a framework that will inform future larger scale quantitative research. Given that the integration of British PAs into secondary care services had not yet been well described in the literature, any survey using closed-ended questions would likely have failed to capture the needed information. Standard qualitative methodology was used to conduct this study (Fig 1). Grounded theory methodology uses an iterative approach to the data collected, with earlier review of materials and earlier interviews influencing the selection of topics discussed with subsequent interview participants to obtain more detailed information about themes raised by earlier interviewees.
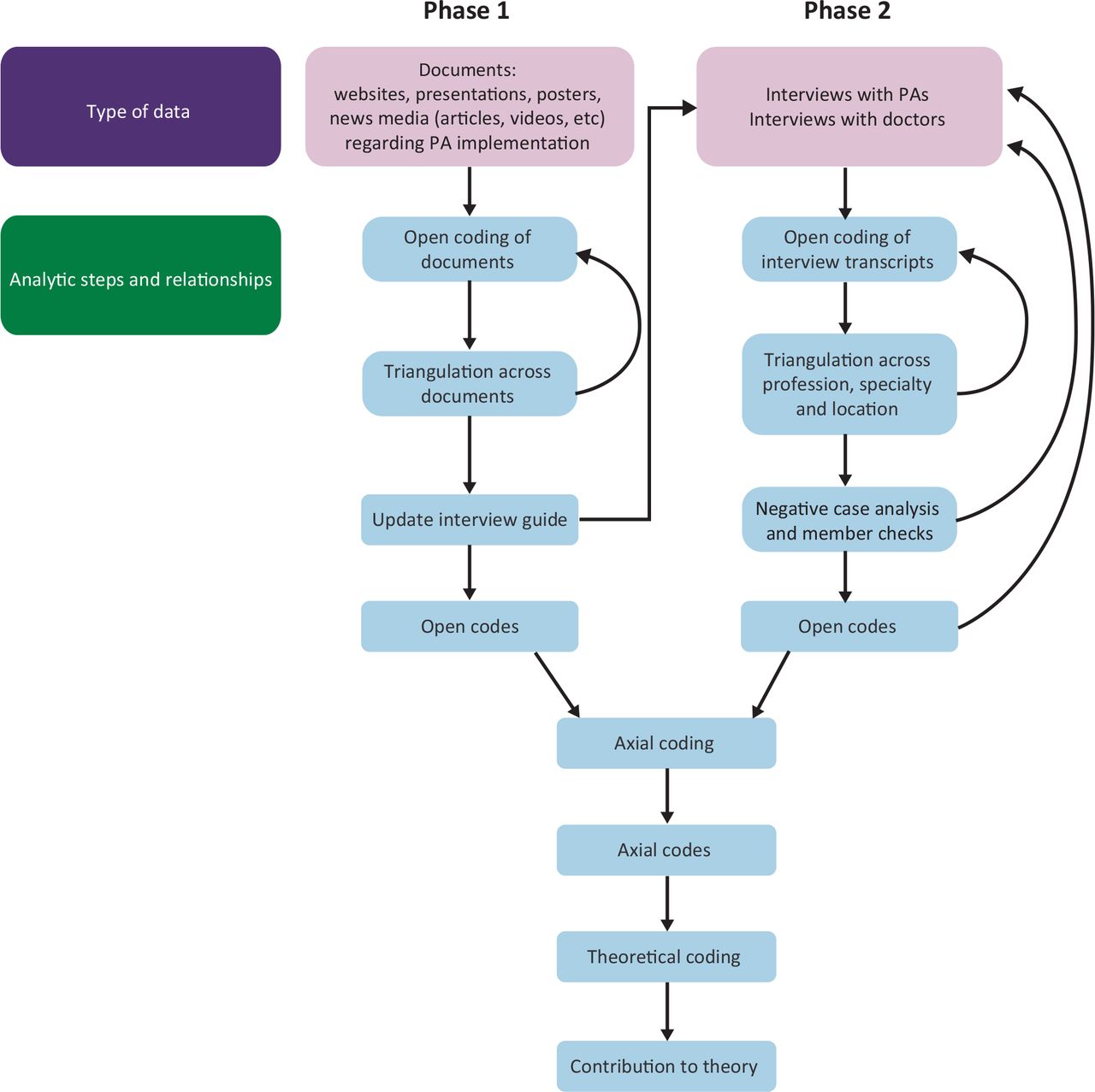
Data collection and analysis model. PA=physician associate.
Research ethics approval was obtained from the Research Ethics Committee at St George's, University of London and the Institutional Review Board at the George Washington University School of Medicine. Participants were recruited via emails sent to the UK PA programmes that had graduated PAs before January 2018, social media posts and word of mouth. PAs were recruited first. These PAs were then asked to approach a doctor with whom they had worked at the time they began practice. All of these doctors were also currently working with the PAs in the study. Consent was obtained from both the PA and the doctor before entering the pair into the study. Teams from a variety of medical and surgical specialties were recruited to maximise variations in experience (Table 1). At the time of the study, there were no UK-educated PAs working in Wales or Northern Ireland. Attempts to recruit Scottish participants were unsuccessful.
Characteristics of physician associate–doctor participant teams
Inclusion criteria were based on the PA's status. To participate, the PA must have been the first PA or part of the first group of PAs to be employed in a particular secondary care setting. The PA must also have undertaken their PA studies in the UK and started their employment within the past 5 years. The PAs were asked to recruit a consultant or a very senior trainee doctor with whom they had worked at the time they started on the service. Junior doctors were not eligible. PAs and doctors were offered a £10 gift card as an incentive to participate. Seven PA–doctor pairs were eventually enrolled in the study as well as one group of one doctor with two PAs. This group was enrolled to increase the potential for a negative case analysis because these two PAs started at the same time, but one of the two PAs left employment on that service after only ∼1 year. Four potential participants (PAs) could not find a doctor eligible to participate and, thus, were not interviewed. Participants were informed that the Principal Investigator (PI) is a PA who has worked in secondary care and that this research was part of her work for a PhD.
The PI interviewed each participant separately for 30–50 min using a semi-structured interview guide, which had been pilot tested before initiation. Interviews were conducted in an online videoconference, audio recorded and subsequently transcribed by a UK transcription service that complies with data protection laws. Transcripts were independently coded by two investigators using standard three-level grounded theory methodology (open, axial and theoretical coding). Coding of data using NVivo 116 began immediately after the first interview and themes from early interviews were explored in greater depth with later interviewees. Interviewing new pairs continued until later interviews stopped revealing new themes.
Standard quality assurance methods for qualitative research were used to improve the trustworthiness of the data. These included triangulation with other data sources, confidential interviews, piloting of the semi-structured interview guide, multiple data coders, negative case analysis and purposive sampling for maximum variation among participant characteristics, such as specialty, region of the country and whether the PA had been hired as a lone PA or as part of a group of PAs.
Results
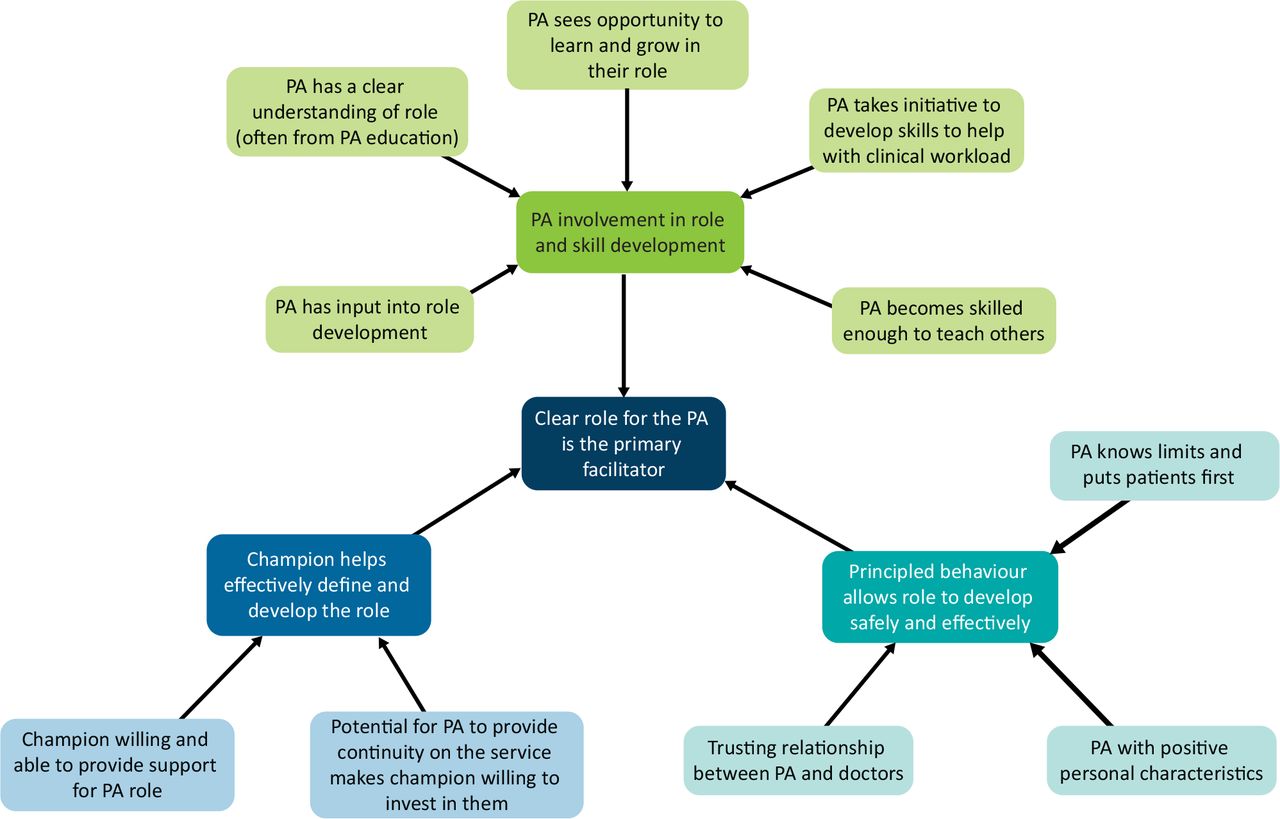
Ten concepts emerged from the data collected, which were grouped into three facilitator themes. Each of these three themes support the overall conclusion that a clear role for the PA on the service is the primary facilitator to the effective integration of the secondary care PA (Fig 2).

Facilitators to the integration of the first physician associates (PAs) into a secondary care service in the NHS.
The three themes comprised the following facilitators:
PA involvement in role and skill development facilitates the deployment of PAs (see Table 2 for supporting data)
The PA has some say in the development of the role.
PAs have a clear understanding of the PA role and can communicate that to others.
PA sees opportunity to learn and grow in their role.
PA takes the initiative to develop skills that help the team with clinical workload.
PA becomes skilled enough to teach others.
A champion who helps effectively define and develop the role facilitated integration of PAs (data in Table 3)
Champion is willing and able to provide support for the PA role.
The potential for PAs to provide continuity of the service makes champions willing to invest in them.
Principled behaviour on the part of PAs allows the role to develop safely and effectively (data in Table 4)
PA knows limits and puts patient safety first.
Positive personal characteristics help the team accept the PA.
A trusting relationship between PAs and doctors enables them to work together effectively.
PA involvement in role and skill development facilitates the deployment of PAs
A champion who helps effectively define and develop the role facilitates integration of physician associates
Principled behaviour on the part of physician associates allows the role to develop safely and effectively
The theoretical code that emerged from these data was that a clear role for the PA is the primary facilitator to successful integration into a secondary care service (Fig 2).
Discussion
This qualitative study of PA–doctor teams offers insights into the factors that enable NHS trusts to introduce the PA more effectively to secondary care teams. We found that having a clear role for the PA on the team was the primary facilitator to integration of the PA in the team. To develop this role, it is helpful to have PAs involved in the process of delineating the PA's responsibilities and the ways in which the PA will interact with the team. This process is made easier when the PA has a clear understanding of their knowledge and limits and when there is a doctor willing to be a proactive champion for individual PAs and for the PA role within the institution. PAs can increase the acceptance of their role by exhibiting desirable personal characteristics, such as humility, service to the team and an awareness of their own limitations, and by working hard to develop advanced clinical skills, which will benefit both patients and the secondary care team. In turn, PAs provided several benefits to the team, most prominently continuity of care that junior doctors cannot provide, given their frequent rotation. Senior doctors felt their investments in training PAs and developing trust with them yielded fruit for years instead of months, which increased their interest in having PAs on their team.
Although several of the findings of this study are consistent with previous literature on PAs both in the UK and abroad, a few findings in this study were new. A crucial finding new to the literature is that having opportunities to grow and learn in their role is a key facilitator of PA practice. When PAs took the initiative to develop skills they thought would be valuable, doctors noted this with appreciation. Learning new skills set up a beneficial cycle. PAs noted that demonstrating facility with one skill often increased the willingness of doctors to train them further. PAs claimed the medical identity through undertaking tasks previously only performed by doctors, such as invasive procedures or breaking bad news to patients. Given that doctors could see how training the PAs reduced their own workload, they became even more willing to educate the PAs further. Although this finding is new in the PA literature, research has found that employees are motivated by development opportunities.7 It will be interesting to observe over time just how motivating these factors are for PAs.
The finding that PAs integrate into the team more effectively when they have some input into the development of their particular role is also new in this population. However, it is more likely that no one has asked this specific question before, rather than that this finding is novel. Ritsema and Roberts obliquely touched on the degree of satisfaction that PAs have with their ‘freedom to choose my own way of working’ in their paper on PA job satisfaction.8 Literature on employee motivation more generally has demonstrated that highly educated professionals strongly value having input into the content and structure of their work.9
The importance of the ability of PAs to communicate their role clearly to others has previously been reported. Multiple studies have shown that PAs need to understand, and be able to articulate, their role to patient and other NHS workers. They cannot rely on others to know that they expect to be contributing as a member of the medical team and, thus, need to advocate for themselves.10 Most PAs were able to make their expectations for their roles clear to the members of the team, but a few PAs struggled to get their teams to view the role the same way they did, and had their scope of practice restricted because of these misunderstandings.
A few studies, including this one, have begun to demonstrate that PAs can become skilled enough on a service to begin to be able to train others, including medical students and junior doctors.5 Initially, PAs needed a lot of help from junior doctors, but, over time, the direction of training often reversed. PAs become the experts on the needs of the patients in the services on which they work, often for years. Trainees rotating through these services then benefit from the knowledge and skills of the PAs and, as future consultants, are introduced to the PA role. The importance of having a champion for PAs within the hospital trust and the finding that champions are willing to invest in PAs because they reap the benefit of their investment in the continuity of care have both been described in previous studies.4–5,11 Champions smoothed the path for the PAs in many ways: administratively, socially and educationally. Crucially, champions used their own credibility to help the PAs increase their own credibility with the medical teams and hospital staff.
The current study reinforced findings related to the effects of prosocial and ethical behaviour of PAs. A key concept in the establishment of the PA profession in the USA 50 years ago was that PAs would be trained explicitly to know the limits of their medical knowledge and seek help when needed.12 In this study, PAs and doctors alike spoke about the need to establish trust. PAs worked to establish this trust by knowing their limits, telling the truth, working diligently to expand their medical knowledge and being willing to do less-glamorous ward tasks. These findings are consistent with studies by Williams and by Theodoraki in which doctors noted how the strong communication skills of PAs increased their willingness to have them on their clinical team.13,14 PAs in this study had often been instructed in these prosocial behaviours by the leadership of their PA programmes.
These findings should assist both those considering recruiting PAs and PAs themselves. As hospital trusts consider adding PAs, they should determine exactly how PAs might help fulfil the needs of their services. PAs are not the answer to every workforce issue in the hospital. It might be advisable to recruit other health professionals instead. Hospital trusts or doctors considering adding a PA to the team would be advised to consult experienced PAs and PA educators about their plans to ensure that the envisioned role is appropriate for a PA. Hospital trusts also need to identify doctors to be PA champions, to be the face of the PA initiative and to give the PAs a source of help. PAs who are new to a service need to take the initiative to continue to develop their medical knowledge and clinical skills. They need to prioritise patient safety in all their work. PAs need to be willing to sometimes do unglamorous tasks, which will help them establish credibility with their teams. They need to capitalise on their training in communication skills to help them develop good relationships with patients, doctors and other members of staff.
The main limitation of this study is the inductive approach inherent in the study design. It is easy to ‘find what you are looking for’ in a study based on a relatively small number of interviews. We attempted to mitigate this limitation by having two investigators independently analyse the data. Another potential limitation is an overly homogenous set of informants, which might limit the themes raised. Unfortunately, we were only able to recruit from 60% of the universities with eligible graduates. In addition, most UK PAs work in south-east England and, thus, this area of the UK is over-represented here. A final limitation is that the participants in this study were all volunteers. It is possible that study volunteers have different views on the PA profession, which might have influenced the results. Further research that is more representative will be helpful to either confirm or refute the findings of this study.
This research study was conducted before the advent of the Coronavirus 2019 (COVID-19) pandemic and during a time where the number of PA programmes in the UK was expanding rapidly, bringing even more PAs into the NHS. These factors provide many avenues for future research. Interviewing a larger number of PAs, from more programmes and hospital trusts would enable us to characterise how the ‘second wave’ of new PA graduates is integrating into NHS hospitals. PAs might have had their roles changed or expanded because of the workforce needs of the NHS during various COVID-related surges. As more programmes have developed, the effects of potentially heterogeneous PA education on the development of individual PAs and the PA profession might become more apparent. Finally, the ongoing attempt to achieve regulation for the profession (as of this writing, slated for 2024) and more clarity around scope of practice could present new barriers and facilitators for PAs working in secondary care.15 Conducting more representative quantitative research with larger numbers of PAs and doctors across the UK would also allow us to overcome some of the methodological limitations of this study.
Conclusion
The success of bringing PAs into a secondary care service in the NHS is not automatically assured. We found 10 facilitators to the successful initiation of the role, some of which are under the control of the hospital trust and some of which are under control of the PA. Both PAs and the hospital trust leadership teams need to work and plan to enable the successful implementation of PAs. Further research as the profession expands across the country and across specialties will likely uncover further facilitators.
Acknowledgements
We would like to thank Dr Barbara Jackson for her mentorship and all of our participants for their time and insights. The authors would also like to thank the PA Foundation for their financial support of the transcription services for this project.
- © Royal College of Physicians 2023. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.