
ABSTRACT
There is now a need more than ever to streamline services. A one-stop shoulder clinic was introduced during the COVID-19 pandemic. A total of 861 patients were seen, saving 794 future appointments. 111 patients had an ultrasound scan and 285 patients had an ultrasound-guided procedure, saving an average waiting time of 134 days. 327 patients had physiotherapy, and the average Oxford Shoulder Score improved by 8.56 at 1 year.
Introduction
Rotator cuff pathology accounts for 70% of cases of shoulder pain and frequently impacts on patients' quality of life.1 Prompt diagnosis and early treatment of shoulder pathology increases the likelihood of return to normal function in patients.1 There is now, more than ever, a need to save and streamline time and resources in the NHS. The concept of a ‘one stop’ service has been developed around the world, involving the collaboration of multiple healthcare professionals to assess and treat patients with shoulder pain on a same-day basis.2,3 These services have been shown to be both cost-effective and time-efficient for patients and service provision.3
Services have included orthopaedic surgeons using portable ultrasound machines in clinic.4–6 So far, none of these services have included the combination of orthopaedic surgeons, musculoskeletal radiologists, and specialist physiotherapists to create a more streamlined, specialist service. At Airedale General Hospital, a one-stop service combining these professionals was introduced in October 2020. The aim of this article was to assess the one-stop clinic service, in terms of time and money saved and patient-reported outcomes.
Method
The one-stop service was delivered in a large room with multiple patient cubicles. The service was provided by two orthopaedic consultants, two orthopaedic middle grade doctors, one musculoskeletal radiology consultant, one radiology fellow, a specialist musculoskeletal physiotherapist, physiotherapists and staff nurses.
Patients were initially consulted by the orthopaedic team, and most received an ultrasound scan performed by the musculoskeletal radiologist. The patient, if indicated, would then have an ultrasound-guided procedure, such as a cortisone subacromial injection or suprascapular nerve block. The patient was then consulted again by the orthopaedic team, followed by the specialist physiotherapist who would initiate a rehabilitation programme for the patient. If a patient required surgery, they would be consented and listed in the one-stop shoulder clinic.
Information about the numbers of patients seen and future appointments saved was collected prospectively. Information related to patient-reported outcomes was acquired from the department's database on Amplitude Pro One (https://amplitude-clinical.com/). These outcome measures were recorded by patients via questionnaires sent out to patients via email through Amplitude. The outcome measures used included the EQ-5D Health Visual Analogue Score (VAS), the EQ-5D Health Index, the VAS Pain Score, and the Oxford Shoulder Score (OSS).
Results
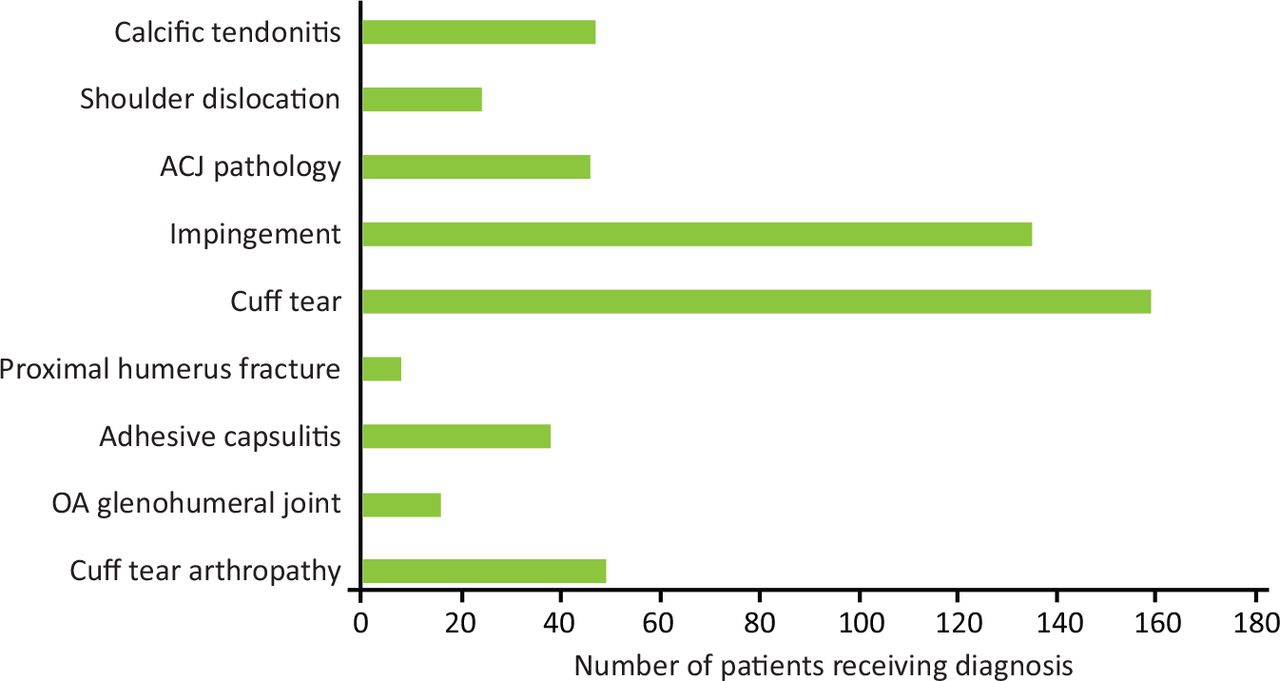
Between October 2020 and June 2022, a total of 861 patients were seen, with 458 male and 403 female patients. Most of the patients had a diagnosis of rotator cuff tear or impingement. Other diagnoses included calcific tendinitis, acromioclavicular joint (ACJ) related pathology (ACJ dislocation or subluxation, ACJ sprain, ACJ osteoarthritis (OA), inflammatory effusion in ACJ), rotator cuff tear arthropathy, adhesive capsulitis, shoulder dislocation related pathology (superior labral anterior posterior (SLAP) lesion, acute dislocation of the shoulder, Bankart's lesion, recurrent/locked shoulder dislocation, anterior shoulder subluxation, chronic shoulder dislocation, chronic shoulder instability, humeral avulsion of the glenohumeral ligament (HAGL) lesion, glenoid fracture of the scapula, labral tear), osteoarthritis of the glenohumeral joint and proximal humerus fracture (Fig 1).
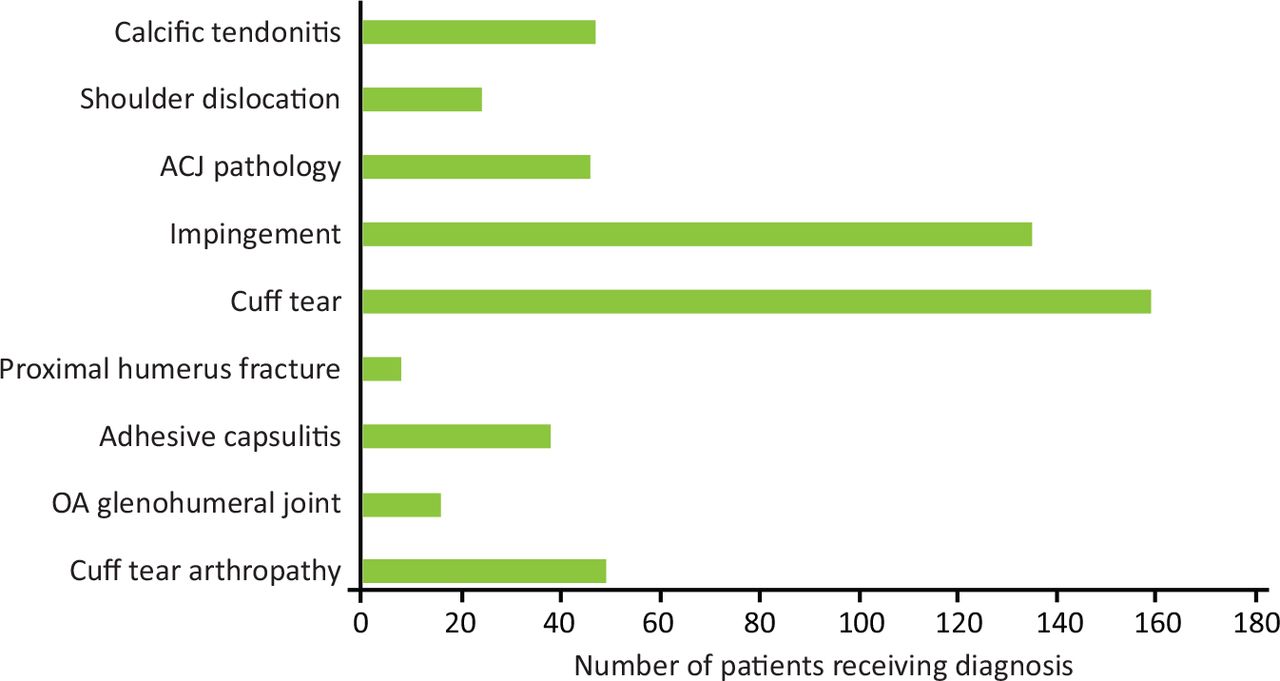
Diagnoses of patients seen in the one-stop shoulder clinic. ACJ = acromioclavicular joint, OA = osteoarthritis.
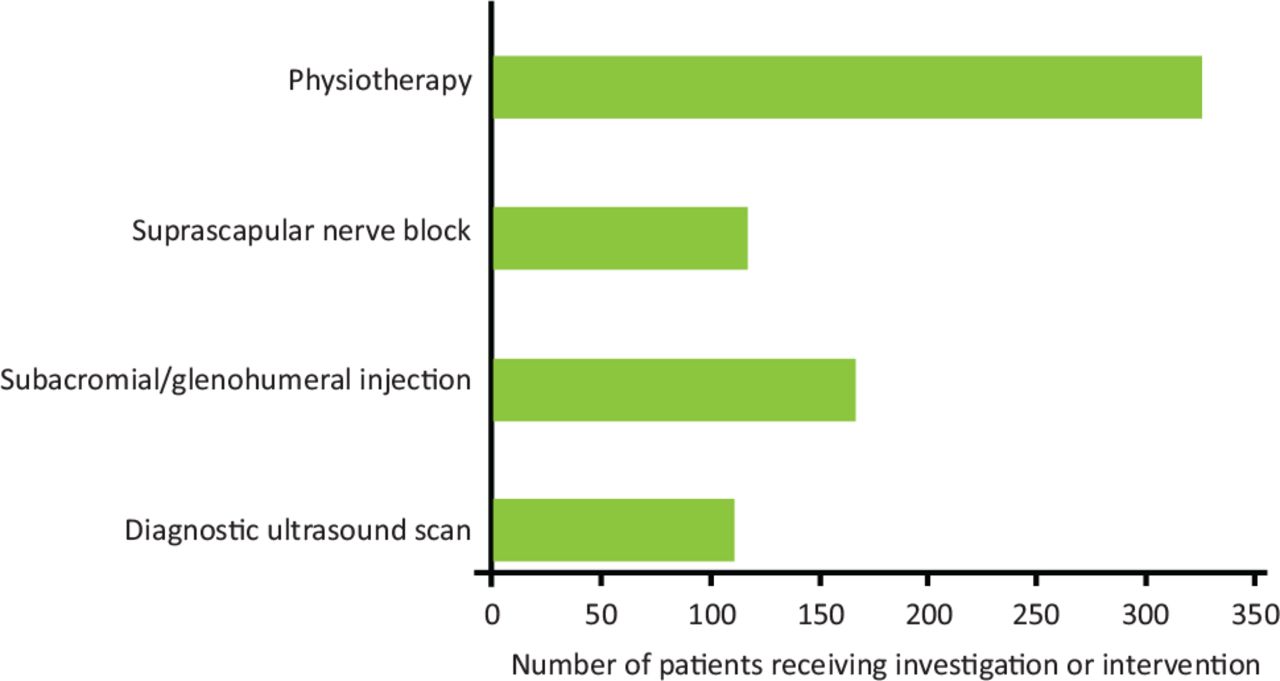
During the patients' one-stop clinic appointment, 111 patients had a diagnostic ultrasound scan. 167 patients had an injection (subacromial or glenohumeral joint), 118 patients had a suprascapular nerve block and 327 patients had physiotherapy (Fig 2). The average waiting time for ultrasound-guided injection outside of the one-stop shoulder clinic was 134 days. For every patient that had either an ultrasound or physiotherapy appointment in the one-stop clinic, there were ‘did not attend’ (DNA) rates. Based on previous DNA rates, an estimated 85 radiology appointments were saved.
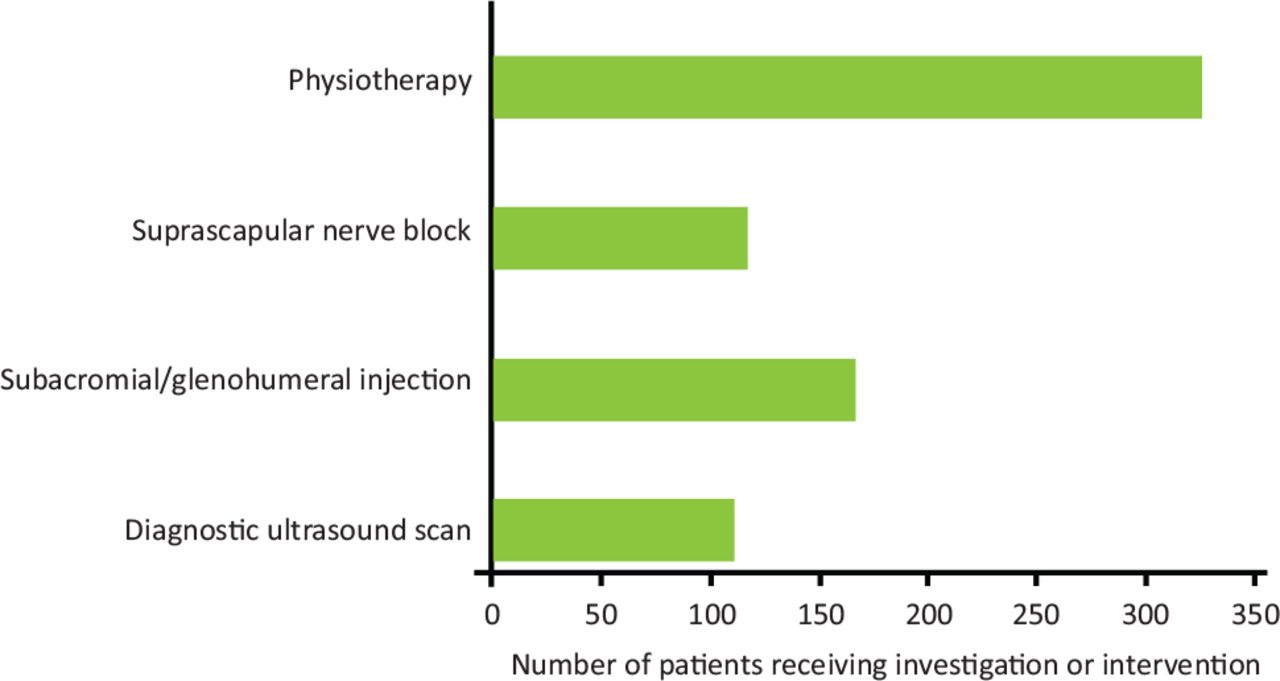
Scan or interventions given in the one-stop shoulder clinic.
There was a dramatic improvement in outcome scores for all the patients 1 year following initial presentation. There was an improvement in OSS by 8.56 at one year (Fig 3). The mean EQ-5D Health VAS improved by 1.76 at one year following first treatment. The EQ-5D Health Index improved from 0.56 to 0.64 and the EQ-5D pain VAS improved from 55.3 to 41.4 at 1 year. There was a reduction in patients that filled out the outcome measures at 6 months and 1 year (Table 1). Overall, 795 future appointments were saved.
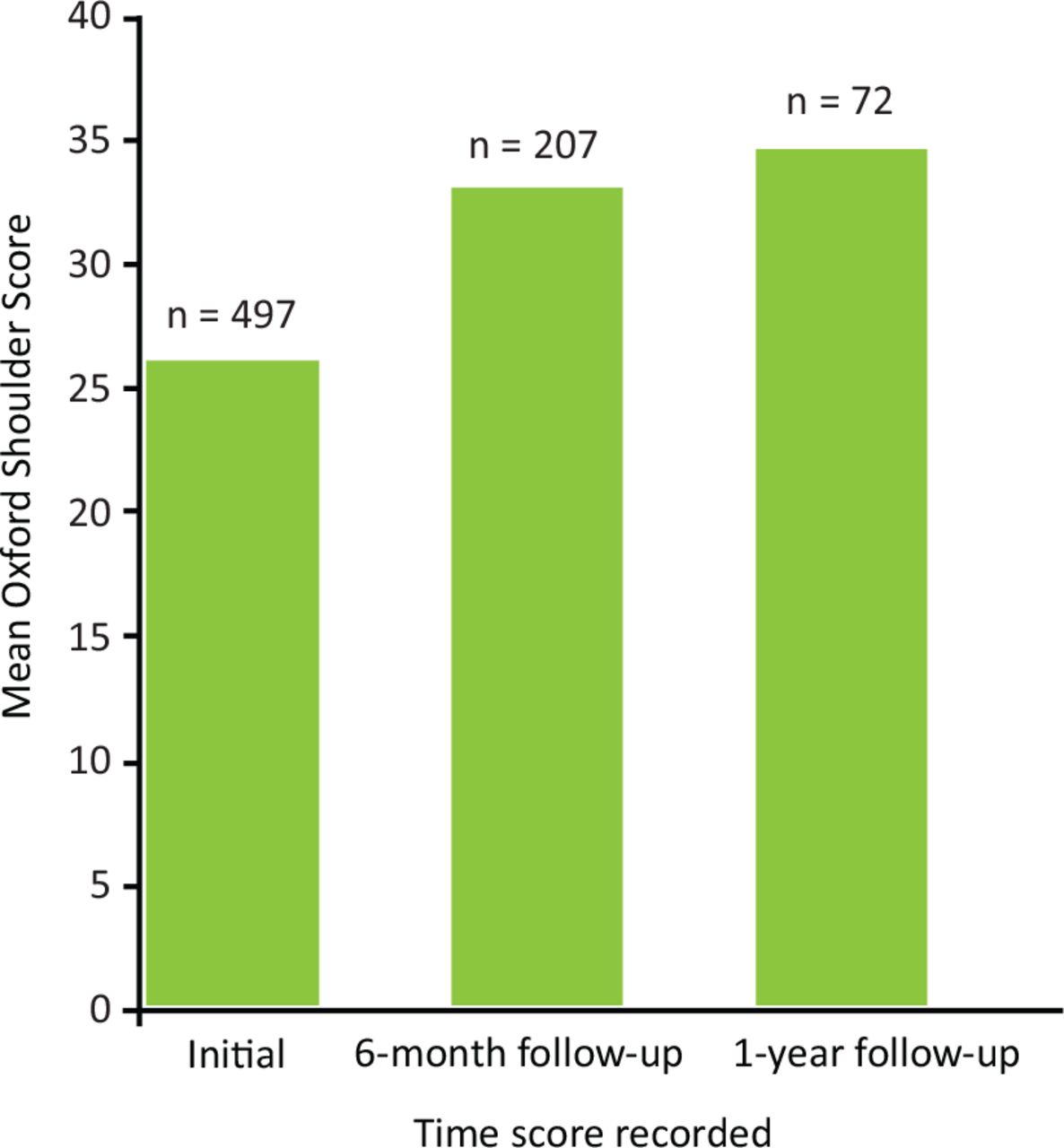
Oxford Shoulder Score of patients seen in the one-stop shoulder clinic.
Patient reported outcome measures for patients seen in the one-stop shoulder clinic
Discussion
Our one-stop service has dramatically saved time for patients, clinical and administrative staff. The DNA rates for physiotherapy and ultrasounds done in the clinic would have likely been higher if future appointments were made instead. Patients witness collaboration between teams which usually happens behind the scenes, undoubtably having a positive impact on patients' perception of their care. The Oxford Shoulder Score in the patients seen in the clinic improved by 8.56 at 1 year which is better than reported minimally important clinical differences.7–9
Having a musculoskeletal radiologist in the one-stop clinic saves time and allows specialist radiologically guided procedures to be performed, which has not been reported in other one-stop services. There are also opportunities for education between surgeons, physiotherapists and radiologists as they work closely together.
A limitation of this study is the reduced number of outcome measures at 6 months, and especially 1 year.
Conclusion
The one-stop shoulder clinic has dramatically saved time and resources during the COVID-19 pandemic by reducing multiple future follow-up appointments and missed appointments. We would certainly recommend the introduction of further one-stop services around the country.
- © Royal College of Physicians 2023. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.