
ABSTRACT
Understanding patients' wishes regarding organ and tissue donation is an important aspect of advance care planning (ACP). Many patients with life-limiting illnesses are still eligible to be corneal donors. A quality improvement (QI) approach has promoted a positive change in culture at an inpatient hospice, making the discussion of patients' wishes on corneal donation the norm. This cultural change led to a sustained high rate of such discussions, despite the multitude of challenges presented by the COVID-19 pandemic.
Introduction
Prior to 2018, the discussion and practice of corneal donation among inpatients at our hospice was uncommon, with only one donation having been facilitated at the hospice during the preceding 3 years. This change in practice was triggered in response to a patient who died at the hospice and had been a strong advocate for corneal donation; his family are still involved in supporting our work to this day.
For patients with many corneal disorders, a corneal transplant is the only option for the recovery of their sight and carries a 93% success rate at one year.1,2 Many patients with a life-limiting diagnosis incorrectly assume that they would not be eligible tissue donors. Facilitating patients to explore and express their wishes with regards to organ and tissue donation is an important part of advance care planning (ACP).3 A survey of healthcare professionals identified that the barriers to conversations about corneal donation are complex and include staff confidence, fear of upsetting patients and families, and concern about enucleation.4 Another qualitative study which explored the views of donor families found that almost all were glad they had agreed to donation.5
Our hospice is a 28-bedded unit split across two wards and serving a population of over 350,000. The medical team on each ward comprises one consultant and up to two junior doctors alongside the multidisciplinary team. The Model for Improvement was used as a framework to guide the project.6 The primary aim of the QI project was to make discussion of corneal donation part of the hospice's culture. The proportion of patients who were given the opportunity to express or discuss their wishes regarding corneal donation was our primary outcome measure, however we also sought to understand how this impacted on numbers of successful corneal donations, which was our secondary outcome measure.
Method
The first cycle of change included an educational session delivered to the hospice doctors to raise awareness of corneal donation and changes to the electronic patient record (EPR) clerking template. This prompted its routine discussion at admission, helped determine eligibility and highlighted patients who wished to donate by triggering an alert to appear on their patient record.
A flow chart was developed and displayed to encourage discussions with patients and simplify the referral process.7
The QI project was initiated by the medical team on one ward, though interventions were implemented on both wards. Data were initially analysed on a ward-by-ward basis to identify learning that might be shared between wards during the plan, do, study, act (PDSA) cycles. A driver diagram was used to help us to identify change ideas which could then be prioritised for PDSA cycles (Fig 1).8

Aims, drivers and interventions. EPR = electronic patient record; NHSBT = NHS Blood and Transfusion.
Results
In the early months of this work, when measures were reported weekly and interventions were introduced at the greatest pace, data analysis was undertaken separately for each ward to better understand what worked well.
The education sessions were supported by NHS Blood and Transplant, and, in addition to explaining the practicalities of the referral and retrieval processes, also involved a corneal donor's widow talking about her experiences, and how it had helped her and her two children following her husband's death. We also discussed phrases that staff could use when broaching discussions with patients and their families.
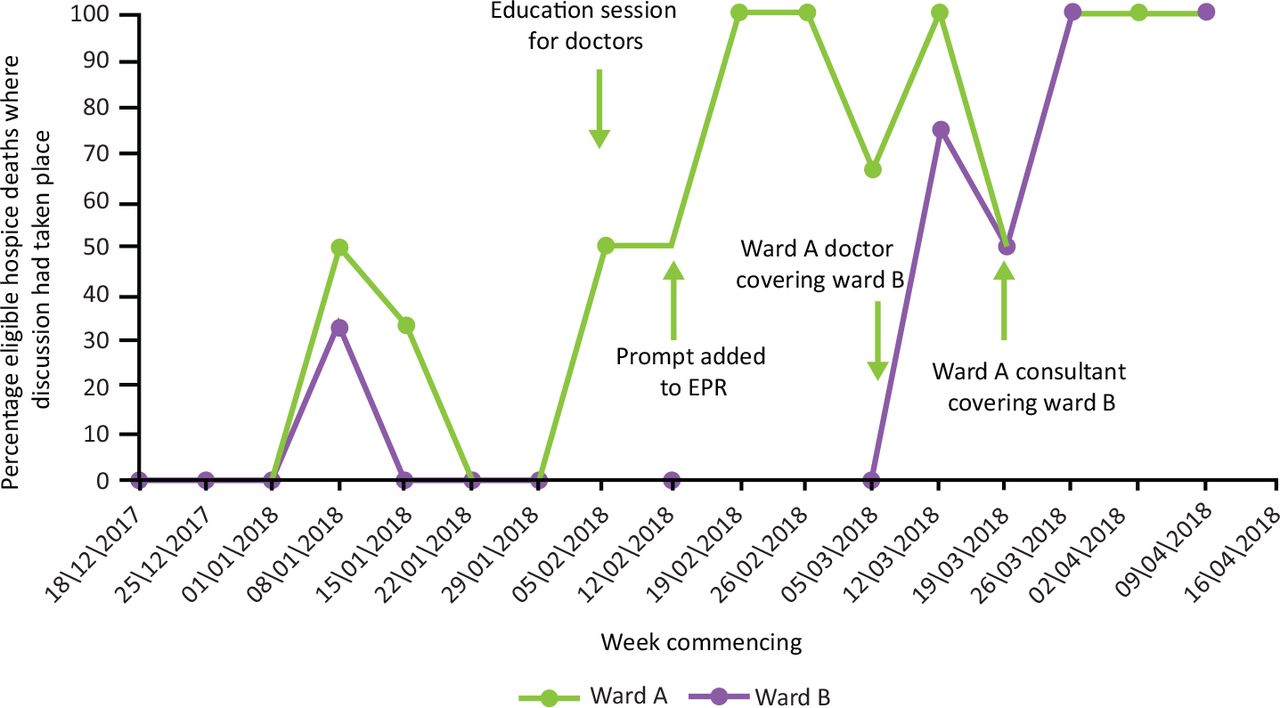
Despite the medical staff from both wards attending the same education session, there was a clear discrepancy in the percentage of patients being offered corneal donation discussion between the two wards (Fig 2). We suspected that the success rate on ward A was a result of greater confidence of all doctors on ward A, who had initiated the project, in opening the discussion. Cross-cover of the wards, which allowed the doctors on ward B to observe the ward A doctors having the discussions, increased the confidence of ward B doctors and within weeks both wards were achieving equally high discussion rates.

Run chart separated by hospice ward, with key interventions overlaid.
The long-term monthly data demonstrates that the initial improvement noticed over the first 6 months of the QI project have been sustained over the course of the following 3 years (Fig 3).
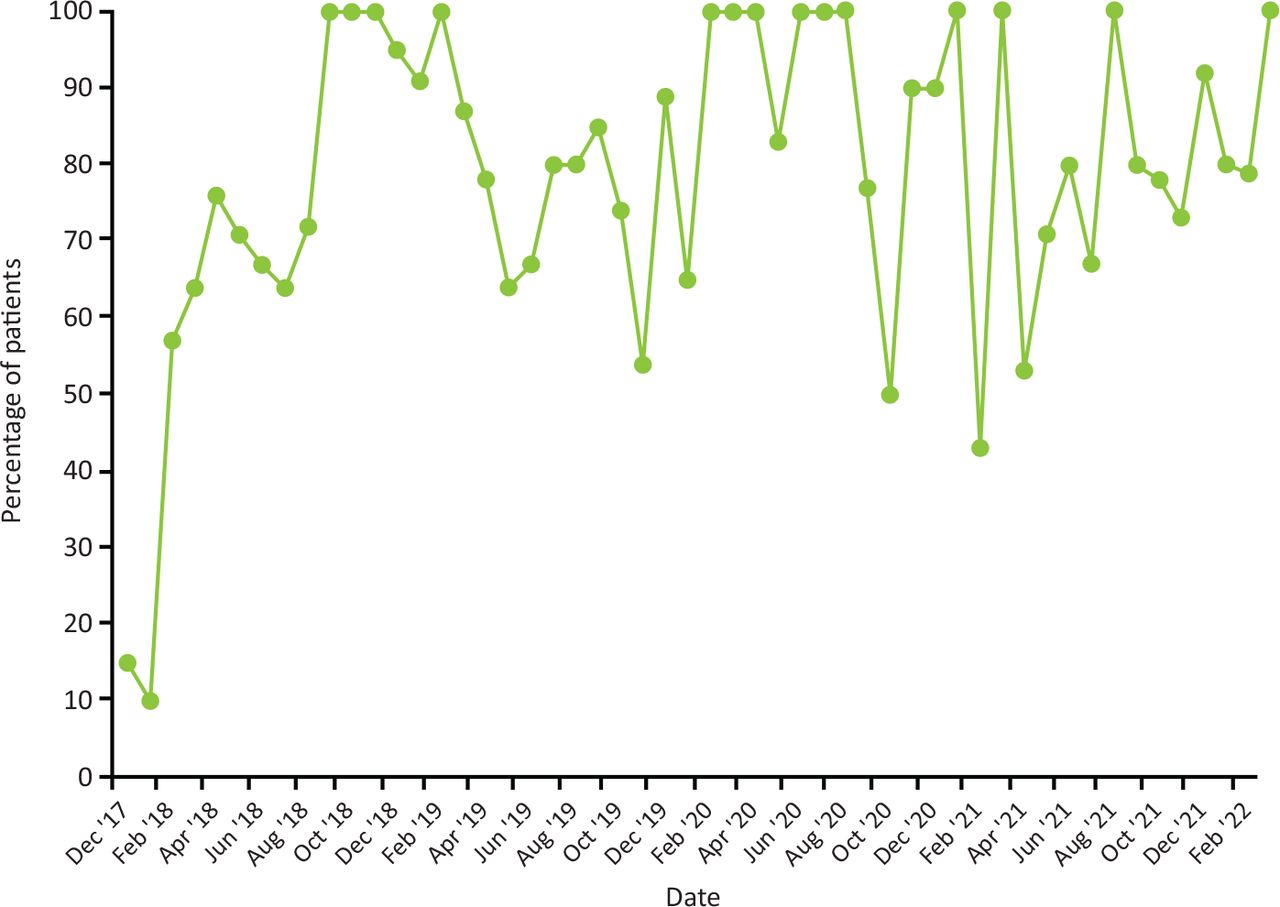
Run chart documenting the monthly proportion of all patients dying in the hospice and eligible to be corneal donors who had a documented discussion with staff regarding their wishes over the project course.
Explaining the process and celebrating our success is now a core element of induction for every new nurse and doctor at the hospice. We are continuously considering ways to improve and sustain our practice. In January 2022 we introduced a new prompt to the first Consultant review template on patients' wishes on corneal donation ensuring that missed discussions at admission were picked up.
We were eager to track the impact of the COVID-19 pandemic, given our reduced bed capacity secondary to staffing levels and the need to distance patients within the hospice. In addition, recent COVID-19 infection was a recognised contraindication to corneal donation. When comparing the 12-month period pre-pandemic with the first 12 months of the pandemic (Table 1), we demonstrated that while our bed numbers and the number of donors had both halved the proportion of patients who had been offered discussion remained high.
Pre-pandemic data compared with data from the first year of the pandemic
Discussion
Discussion around corneal donation has become part of everyday language at the hospice. We believe by making a change in culture our primary goal, as opposed to increasing the number of donors, is the success driving this QI project, and in particular its sustainability even in the face of the disruption of the COVID-19 pandemic. Despite halving the bed capacity and redeploying staff, the proportion of patients offered discussion remained sustained at an average of 80%.
The number of patients expressing a wish to donate does not equate to the number of referrals and the number of referrals does not equate to the number of donations. Explanations for this discrepancy include families not wanting to consent despite the patients' wishes, hospice staff missing the referral window, discovering a medical contraindication to donation or the retrieval team's inability to facilitate retrieval within the time frame. While increasing the number of referrals for corneal donation was not our primary goal, it is of course of public health interest to note of the significant number of corneal donations facilitated in one unit as a result. Over the past 4 years since our first referral in 2018 there have been 235 referrals with 156 of those referrals resulting in donors.
In terms of next steps and scaling up the success we have had in making corneal donation discussions the norm, we, together with the widow of our first donor, have provided training sessions for nearby hospices, been interviewed on national radio and more recently have been filmed with NHS Blood and Transplant for training videos that they intend to use to support other hospices across England and Wales.
Conclusion
This project demonstrates the role of QI methodology in enabling change of culture, which is reproducible despite significant challenges, as seen during COVID-19. This QI initiative has been key in encouraging ACP discussions in patients with a life-limiting diagnosis while enhancing the lives of many by giving the gift of sight.
Acknowledgements
We would like to acknowledge the involved patients, relatives and staff of Marie Curie Hospice Cardiff and the Vale, who supported this work and engaged in conversations about their wishes regarding tissue donation.
- © Royal College of Physicians 2023. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.