
ABSTRACT
The stressful nature of the medical profession is a known trigger for aggression or abuse among healthcare staff. Interprofessional incivility, defined as low-intensity negative interactions with ambiguous or unclear intent to harm, has recently become an occupational concern in healthcare. While incivility in nursing has been widely investigated, its prevalence among physicians and its impact on patient care are poorly understood. This review summarises current understanding of the effects of interprofessional incivility on medical performance, service and patient care. A structured search and screening of literature returned 13 studies of diverse origin, methodology, quality, size and population type. The consensus is that interprofessional incivility is common among physicians and nurses and has both psychological and clinical outcomes, resulting in stress, compromised patient safety and poor quality of care. Junior staff are affected more often than consultants, with higher rates in radiology, general surgery, neurosurgery and cardiology. Incivility also undermines medical team performance, particularly in perioperative settings. In patient care, incivility is associated with complications, medical errors, mortality, and compromised patient safety and quality of care. Patients whose surgeons have a record of incivility can be at higher risk of complications. The impact of incivility on medical performance, service and patient care appears systemic and must be addressed accordingly. This analysis was limited by the methodological weaknesses of the included studies, which highlights the need for more high-quality empirical research. This would benefit the NHS and other stakeholders when designing targeted interventions. In particular, establishing quantitative methods for identifying and measuring incivility will be crucial for improving our understanding of the phenomenon.
Introduction
Healthcare is an undeniably stressful work environment. Its high-pressure nature is often linked to phenomena of overtly abusive behaviour, such as violence, aggression, bullying, tyranny, deviance, discrimination, harassment and ‘feuding’ among staff. These antisocial behaviours have been widely investigated in various professional environments, including healthcare. More recently, low-intensity negative interactions have also become a concern for organisational researchers.1 Rude, dismissive and aggressive (RDA) communication,2 as well as insensitive and disrespectful behaviours, are some of the manifestations of ‘workplace incivility’3,4 or ‘interstaff incivility’.1 Typical examples include belittling comments or dismissive gestures (eye rolling, lip sounds, sighs and muttering), skipping greetings, gossip, social exclusion, unavailability, impatience with questions, and condescending language or voice intonation. Workplace incivility has been defined as ‘a low-intensity deviant behaviour with ambiguous intent to harm the target, in violation of workplace norms for mutual respect’.3 Uncivil behaviours are also described as ‘disruptive’5 and ‘unprofessional’.6 Experiencing incivility has been argued to lead to negative cognitive and behavioural outcomes for staff (rumination, reducing work effort, spending time worrying and taking frustration out on patients), leading some authors to liken it to ‘a pathogen that can quickly and silently sicken a team, department, and organisation as well as customers and other external stakeholders.’7
In relation to healthcare settings, the focus in medical literature has been on perceptions of incivility8 and on its effects on quality and safety,9,10 team cohesion and performance,7,11–19 staff physical and mental health (leading to burnout, stress and depression),7,20 staff satisfaction21 and staff retention,22 especially among nurses. Several studies also explore the preventive measures that can be taken.23–25 To this end, it has been crucial to establish the predictors and triggers of incivility in healthcare teams,26 including high workload, communication or coordination issues, patient safety concerns, lack of support and poor leadership. Organisational culture can normalise incivility, and tolerance of low-level poor behaviour might eventually enable more serious misbehaviour.6 Research has effectively demonstrated how a culture of civility, teamwork and engagement is vital for the long-term success of medical practices.27,28 Speaking-up skills have also been found to be effective in reducing the frequency and impact of unprofessional behaviours.6 Other interventions, as highlighted by the NHS Leadership Academy, include managing work-related stress, managing with kindness, civility and respect, managing incivility and disrespect, understanding discrimination and managing to avoid discrimination. Therefore, identifying and targeting uncivil behaviours among medical staff are fundamental to reducing their consequences in healthcare delivery.
While numerous studies have investigated the impact of interprofessional incivility in nursing, few have examined how incivility affects physicians' medical performance, service and patient care. These toxic dynamics can manifest as ‘vertical’ or ‘horizontal/lateral’ abuse, depending on whether incivility happens between members of staff differently positioned in an organisational hierarchy or between members of staff at the same level, respectively. In the context of this review, ‘medical performance’ signifies the aspects of functional ability required in health professions, whereas ‘service’ refers to specific activities that are part of the job, such as on-scene response, assessment, stabilisation, initial treatment as directed and transport to the appropriate receiving facility (ie trauma centre or hospital) for medical emergency or trauma patients. ‘Patient care’ refers to the services rendered by members of the health professions for the benefit of a patient.
This review of the effects of incivility on physicians' performance, service and patient care will elucidate its specific impact on various areas of healthcare delivery.
Methodology
Search strategy
In January 2021, I conducted a computerised literature search of four databases (PubMed, EMBASE, Cochrane Library and CINAHL). Keywords were generated after an initial pilot search and review of the existing literature to ensure that they were broad enough to capture relevant articles while filtering irrelevant material. Only references published in English were sought, without restriction on location or date. I reviewed the bibliographies of all the papers included in the initial shortlist to identify any further studies for inclusion. Duplicate records were removed before selection. Reference and citation tracking were also carried out.
Inclusion and exclusion criteria
I included studies the participants of which were employed in healthcare and engaging in forms of interprofessional incivility in clinical and patient care, with no restriction as to the type, department, location or place of work (hospital, GP surgery, etc). The main inclusion criterion was that at least one of the members of the team be a consultant (studies restricted to nurses and medical students only were excluded).
The study design in relevant articles had to be observational and feature some form of measurement (quantitative, qualitative or mixed methodology) for ‘incivility’ and ‘civility’, such as RDA in interprofessional dynamics. The impact of interprofessional in/civility was restricted to observational studies analysing medical performance, service and patient care.
I only considered studies examining face-to-face interprofessional interactions or staff–patient interactions; telephone-only, email and technology–human interactions were excluded. Only articles in peer-reviewed journals, with empirical findings related to interprofessional (in)civility, were considered.
I specifically excluded papers not in English, studies in non-medical settings (eg nursing), intervention studies, non-peer-reviewed material, theses, dissertations and review/theoretical papers. Studies conducted in psychiatric hospitals were also excluded because of the potentially higher prevalence of patient incivility in such settings.
Screening
The shortlisted articles underwent abstract screening and any articles potentially reporting relevant data were selected for full-text screening; the benefit of doubt was given when inclusion was uncertain. Lastly, a full-text review was carried out to exclude articles that did not present empirical data or did not focus on the actual effects of incivility on medical performance, service or patient care.
Risk of bias and quality assessment
Quantitative studies were assessed with the Medical Education Research Study Quality Instrument (MERSQI). Within the full-text review, the definitions of ‘civility’ and ‘incivility’ were noted, along with authors, title, link, DOI, method/s, participants, results and conclusions of the effects on medical performance, service and patient care (Table 1).
Medical Education Research Quality Instrument for qualitative studiesa
Findings
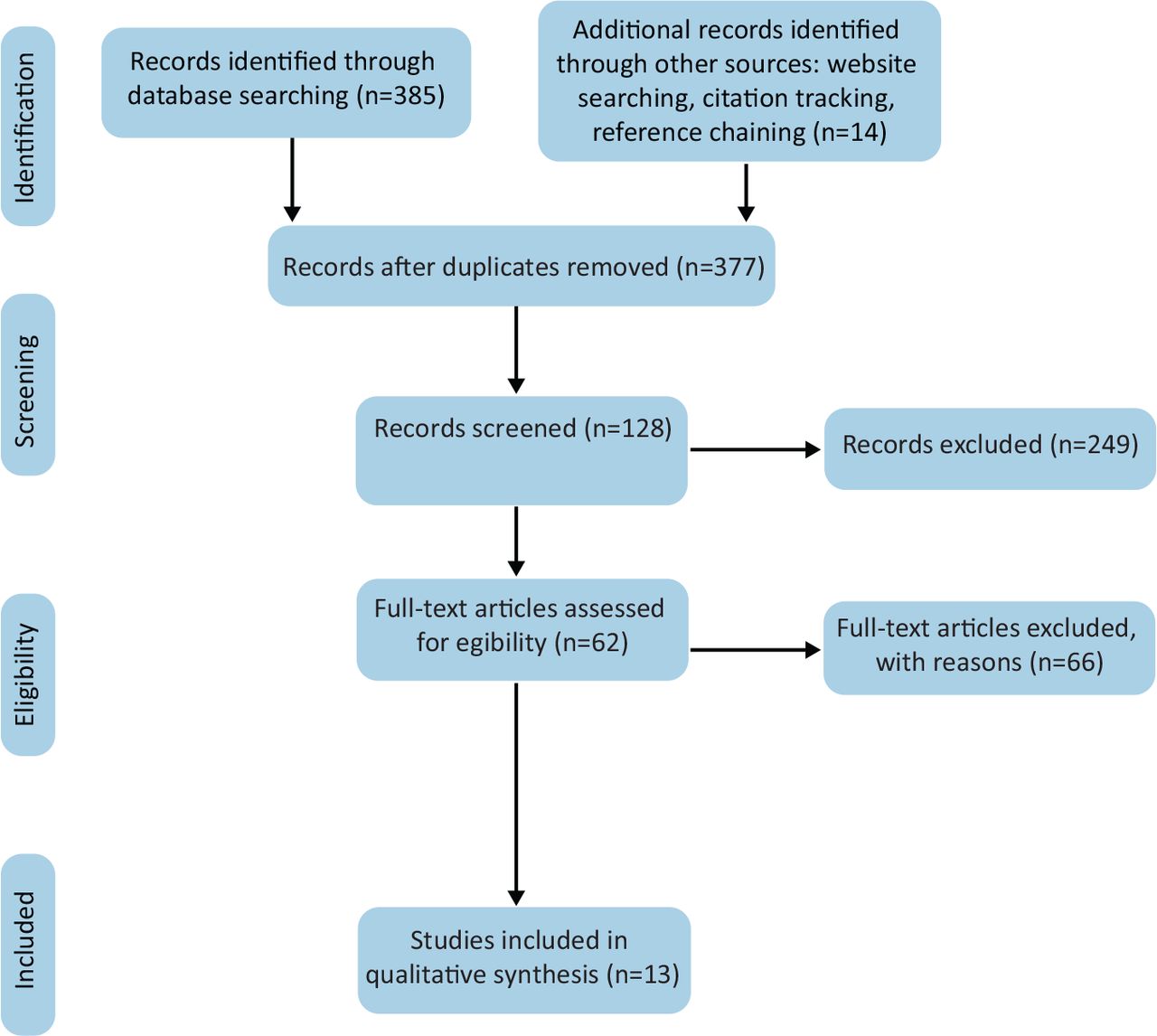
The database searches retrieved 399 records, reduced to 277 after deduplication. Following broad and narrow screening, 13 peer-reviewed papers were considered suitable for inclusion in the review (Fig 1).2,5,6,14,29–34,35–37 The findings are reported here in a narrative format, with descriptive results of the studies presented first, followed by separate discussions of the impact of incivility on medical performance and service, and on patient care.

Study workflow.
Overview of studies
The included studies were geographically heterogeneous: five (38%) were conducted in the USA, three (23%) in Israel, two (15%) in the UK, and one in each of Egypt, Iran and Australia. Methodological approaches also varied: four studies (31%) reported mixed quantitative–qualitative data, and nine studies (61%) qualitative data only.
The studies comprised 26,534 participants and differed considerably in population size and type: five (38%) studies involved more than 1,000 participants, five (38%) between 237 and 1,000, and three (23%) involved 160 participants or fewer (Table 2).
Overview of included studies (Continued)
MERSQI scores for quantitative studies were relatively low (mean score = 7.8, range 6.5–12), and methodological limitations were often similar across studies. More recent publications showed higher scores (Table 1).
Impact of incivility on medical performance and service
The literature suggests that the effects of interprofessional incivility on medical performance are both psychological and clinical. The former include stress, frustration, lack of concentration and negative impacts on communication, collaboration, information transfer, and workplace relationships. Clinical effects, resulting from the cognitive impairment caused by the psychological effects, were found in an early study to include adverse events (AEs), medical errors, threats to patient safety, patient mortality, and decreased quality of care and patient satisfaction,36 and were later confirmed by two more studies35,37 focusing on the negative impact of disruptive behaviours on medical performance, service and patient care.
In one study focusing on accident and emergency (A&E) departments, 57% of participants reported witnessing disruptive behaviours by physicians and 52% witnessed disruptive behaviours by nurses; 32.8% associated disruptive behaviour with the occurrence of AEs, 35.4% with medical errors, 24.7% with compromised patient safety, 35.8% with poor quality of care and 12.3% with patient mortality; 18% reported being aware of a specific AE that had occurred as a direct result of disruptive behaviour.35 An examination of ‘disruptive surgeon behaviours’ in a perioperative environment reported snowball effects of increasingly frequent surgical errors, diminished respect for surgeons, feelings of powerlessness and decreased willingness to help. Heightened anxiety among team members impaired decision making and communication.5
Lateral incivility within the NHS was assessed in one study using a mixed method (survey and focus groups) to describe the extent, context and impact of RDA communication between doctors. It was reported that 31% of doctors described being subject to RDA communication multiple times per week, with junior and registrar doctors affected twice as often as consultants. This research uniquely gathered data by specialty, reporting higher rates of incivility in radiology, general surgery, neurosurgery and cardiology. Of the respondents, 40% reported that RDA moderately or severely affected their working day. The context for RDA communication was described in thematic terms of workload, lack of support, patient safety, hierarchy and culture, whereas its impact was described as both personal (emotional distress and substance abuse) and professional (demotivation, inefficient working practices and avoidant behaviours).2
Another A&E study focused on physician–nurse interactions, showing that physicians gave more importance to nurse–physician relationships than did nurses (90% versus 70%). In addition, 81% of physicians and 52% of nurses exhibited disruptive behaviours perceived to result in adverse outcomes, such as stress (97%), job dissatisfaction and compromised patient safety (53%), poor quality of care (72%) and errors (70%). Errors were correlated with decreased concentration, fatigue, impaired nurse–physician relationships, reduced team collaboration and communication, and reduced information flow.31 In another study, 93.3% of respondents expressed concern about disruptive behaviour by physicians, usually in the form of refusal to cooperate; 39.2% had previously experienced such behaviours, and 78.3% experienced at least one incident monthly.34
Studies using simulation-based methodologies found that even mild incivility caused significant declines in team performance and care outcomes. One study focused on the effect of rudeness on the collaborative mechanisms of teams, demonstrating how this not only affected individual staff members,14 but also resulted in diminished performance across all team outcomes (eg diagnostic and intervention scores) and process parameters (eg information sharing and communication). Thus, rudeness can debilitate intervention acuity, resulting in poorer medical treatment and severe clinical outcomes, particularly in intensive care units.33
Another simulation-based study examined how incivility influenced the performance of anaesthesiology residents by randomly assigning participants to either a normal or ‘rude’ environment during a validated, simulated operating room crisis. Of the control participants, 91.2% were rated as performing at their expected level, compared with only 63.6% of those exposed to incivility. Incivility had a particularly negative impact on vigilance, communication and teamwork, causing diagnostic errors and oversight of crucial elements, such as bolusing intravenous fluids, reducing the anaesthetic agent and calling for blood in a timely fashion.30 Exposure to rude behaviour was associated with poorer performance on cognitive tasks, reduced creativity, flexibility and analytical skills, diminished recall of tasks, impaired quality of performance and limited helpful and prosocial attitudes. The adverse effects on diagnostic and procedural performance were mediated by decreased information sharing and diminished help seeking, respectively. Exposure to rudeness weakened the collaborative mechanisms (communication, helping, and information and workload sharing) that underpin team-based medical care, and was also significantly associated with team members' state depletion during the shift in which the event occurred: state depletion scores were strongly correlated with proximity to the rudeness event for at least 24 h after it occurred (p=0.013).29
The negative impact of unprofessional behaviours on teamwork was more frequently reported by nurses, employees under 35 (more likely to be in junior positions), and management and administrative staff in non-clinical positions,6 all of which ultimately affected patient care and quality of service.
Impact of incivility on patient care
This review indicates that the effects of interprofessional incivility on medical performance and service have repercussions on four main areas of patient care: patient satisfaction, patient safety, surgical and medical complications, and mortality.
In a 2008 survey, 77% of respondents (88% of nurses and 51% of physicians) reported witnessing disruptive behaviour of physicians, and 65% (73% of nurses and 48% of physicians) reported witnessing it by nurses. Respondents agreed that disruptive behaviours were linked with AEs (67%), medical errors (71%) and patient mortality (27%).37 A 2012 study reported similar findings on the actual incidence of incivility on patient satisfaction (78%), care (53%) and mortality outcomes (22%).35
Elsewhere, team members reported feeling concern for the safety of patients when surgeons reacted to a situation by behaving disruptively; furthermore, instead of attending to the procedure and the safety of the patient, perioperative team members would become engrossed in de-escalating and pacifying the surgeon to mitigate further outbursts.5 A focused investigation of the effect of incivility (‘unprofessional behaviour’) in surgery, collating observations from 13,653 patients and 202 surgeons, demonstrated that patients whose surgeons had higher numbers of co-worker reports about unprofessional behaviour over the previous 36 months appeared to be at increased risk of surgical and medical complications.32
When the focus was on patient safety outcomes (AEs, protocol compliance failure and poor team information sharing), 28 AEs were reported, including: errors and delays in transfer of information regarding patient medical condition and care; inappropriate, unnecessary or delayed treatments; medication errors; patient identification errors; postoperative complications unrelated to the natural course of the patient's disease; accidents while transferring patients between departments; medical recording errors; delayed or erroneous diagnoses; iatrogenic infections; poor operation of medical devices; and un- or misidentified laboratory samples. State depletion was marginally and inversely correlated with other forms of medical service, such as medication and hand hygiene protocol compliance.33
Discussion
Interest in the impact of interprofessional incivility on healthcare provision has only emerged in recent years, as attention has shifted from overt unprofessional behaviours to subtler, yet equally damaging interactions. The effects of interprofessional incivility on medical performance and service cannot be disjointed from their repercussions on patient care. Decreased vigilance, reduced capacity for decision making and diagnosis, and impaired teamwork, communication and information flow all ultimately affect patient care in terms of satisfaction, safety, complications and mortality, with such outcomes as misdiagnosis, iatrogenic complications, medication errors and poor treatment. What has clearly emerged is the snowball effect of incivility, which affects not only the mental health and performance of individual staff members, but also collaboration and information sharing within teams.
The systemic nature of incivility emerges in most studies, suggesting that interventions should also be systemically designed. Identifying and measuring the manifestations and effects of incivility are particularly challenging. Most of the studies included adopted questionnaire- and/or survey-based qualitative methods; whereas the diffusion of the phenomenon in healthcare, and its effects, were readily reported, direct observations (eg by prospective and systematic monitoring of uncivil interactions or review of hospital surveillance systems) were scarce. Only two studies used measurement methods other than participants' perceptions, and the methodological quality of many of the studies reviewed was comparatively low. However, this particular field of study has only recently emerged; therefore, the pioneering character of the work might offset, in part, any methodological weaknesses and, in fact, methodological quality appeared improved in more recent studies. This highlights the need for more high-quality empirical research based on objective observations and measurements of the effects of incivility.
The literature review showed that no specific gender, age or ethnic groups could be identified as particularly likely targets. Certain specialties, such as neurology and radiology, might be at higher risk; incivility also appears to be perceived more by nurses and junior medical staff, suggesting that they are its main targets, aside from patients. There are in fact indications that seniority, often associated with higher organisational rank, is associated with decreased experience of incivilities, implying that higher task proficiency and status are protective factors. However, the possibility remains that the most-protected categories are in fact those that inflict incivility on others, especially if such attitudes are entrenched in institutional culture.
Study strengths and limitations
At present, there is a wealth of theoretical and empirical papers on incivility in nursing, but few focus on uncivil behaviours among consultants/physicians and their impact on patient care. On the one hand, the diversity of the papers included (in terms of geographical setting, methodology and scope) allowed a multifocal assessment of the phenomenon. The research included was conducted with nurses, medical, managerial and administrative staff, in addition to consultants/physicians, shedding light on the phenomenon from different perspectives and, in particular, on the ways in which incivility among medical staff affects the staff themselves first, and patients in turn.
On the other hand, there are inherent limitations to this analysis, because of the heterogeneous definitions used for the same behaviours (disruptive, unprofessional and RDA), the variety of people involved in a ‘network of incivility’ (administrative and managerial staff, nurses, consultants/physicians, patients and families), and the disparate tools and methods used to measure incivility. Moreover, different understandings of the nature of incivility could introduce bias into self-reports of incivility exposure. Most of the reported findings are based on subjective judgements and observations from participants, who might have been more likely to volunteer for the studies after experiencing incivility or, conversely, might have avoided participation so as not to draw attention to their experiences. Unprofessional behaviour by surgeons might have also gone unreported, leading to misclassification of primary exposure.
Most studies did not use a prescriptive measure for incivility, such as the Workplace Incivility Scale38; neither were participants usually provided with clear a priori definitions of ‘incivility’, ‘disruptive behaviour’ or ‘unprofessional behaviour’. Nevertheless, because a participant's response to incivility is dictated by their experience of the situation, researchers had no choice but to rely on subjective self-reports. Undeniably, the above definitions overlap in meaning and manifestations; future studies should agree on a common definition for low-intensity behaviour with ambiguous intent to harm the target and, most crucially, on a common scale to measure its effects.
Even within such limitations, however, this review highlights behaviours that have been unnoticed for too long despite their dramatic impact on healthcare delivery.
Conclusion
Interprofessional incivility has a significant impact on medical performance, service and patient care. It affects medical, physical and cognitive skills, teamwork and professional communication, and patient safety at different levels. The resulting health damage impacts various professional and nonprofessional categories, from healthcare staff to patients and their families. Incivility emerges as a systemic issue that urgently requires systemic interventions. This report demonstrates that, over the past 15 years, incivility and disruptive behaviours in healthcare have become a concern in several countries, and that research on this topic is moving from qualitative methods to empirical approaches, such as simulations. The NHS and other British healthcare organisations are likely to benefit from using these findings to design targeted interventions and explore commissioning of further research.
Summary
Acknowledgement
Grateful thanks to Caroline Kamau, PhD supervisor at Birkbeck, University of London, for assistance with the manuscript through to submission.
- © Royal College of Physicians 2023. All rights reserved.
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.